Introduction
Neoplasms of the fallopian tube are the least common
tumors of the female reproductive system. To date, mature teratoma
of the fallopian tube associated with incomplete uterine
mediastinum has not been reported and ∼60 cases of mature teratoma
of the fallopian tube have been reported worldwide. None of the
reported cases were diagnosed preoperatively. The pathogenesis of
teratoma of the fallopian tube remains poorly understood. Tumors
are accidentally discovered and confirmed by pelvic surgery, as a
result of diagnosis of uterine fibroids, ovarian cysts and cesarean
sections. It has been hypothesized that teratomas originate from
the germ cells, as teratomas are found most frequently in the
gonads. The karyotype of all benign teratomas is 46,XX. Surgery is
used to treat teratomas and the prognosis of this disease is
generally good (1–5). In the present case report, the patient
was presented to The Second Xiangya Hospital of Central South
University (Changsha, China) with fertility issues. The
postoperative diagnosis was incomplete uterine mediastinum and
mature cystic teratoma of the fallopian tube. One year after
surgery, the patient became pregnant and gave birth to a healthy
baby. Written informed consent was obtained from the patient.
Case report
Patient presentation
A 23-year-old female (gravida 0, para
0) who had been married for two years was admitted to The Second
Xiangya Hospital of Central South University (Changsha, China) with
fertility issues. The patient reported intermittent lower abdominal
pain for 8 months. The individual’s menstrual cycle was regular.
Pelvic examination revealed a stationary cystic mass of ∼8×3 cm in
the left adnexal region; the right adnexa and the uterus were
normal. The patient’s family history was negative for any
hereditary diseases. Serum concentrations of C12 were within the
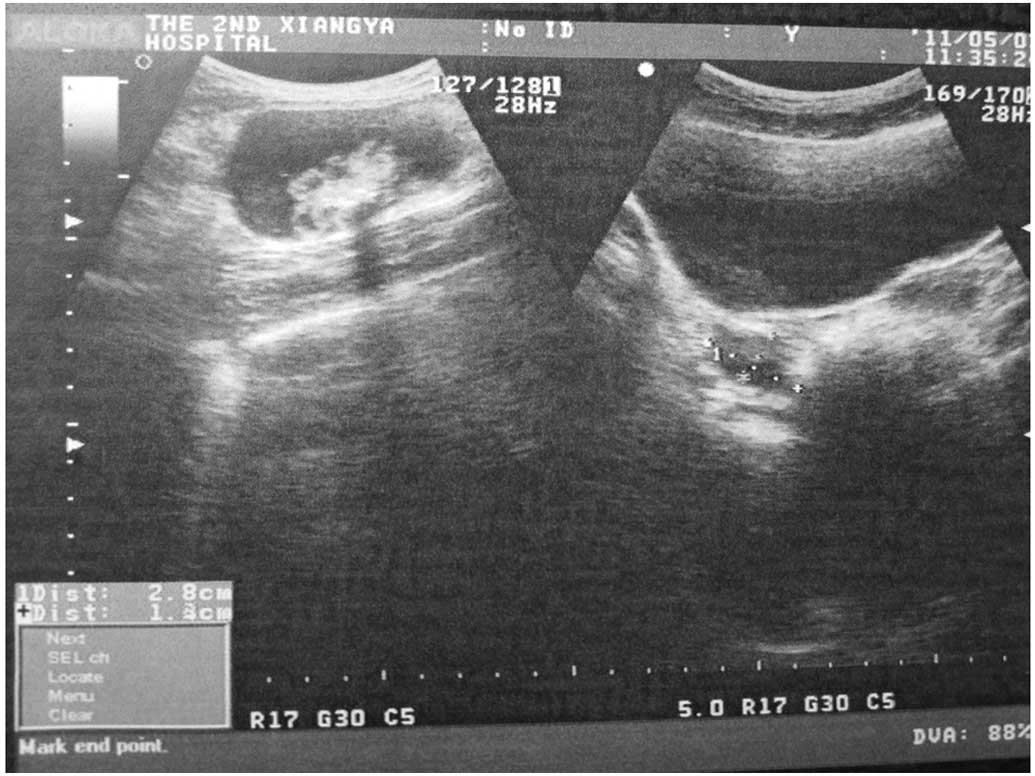
normal limits. Ultrasound examination revealed that the endometrium
was unclear, and a cystic mass of ∼8×4 cm to the right of
hypogastic region was observed. The mass contained foci of
calcification of ∼3×2 cm (Figs. 1
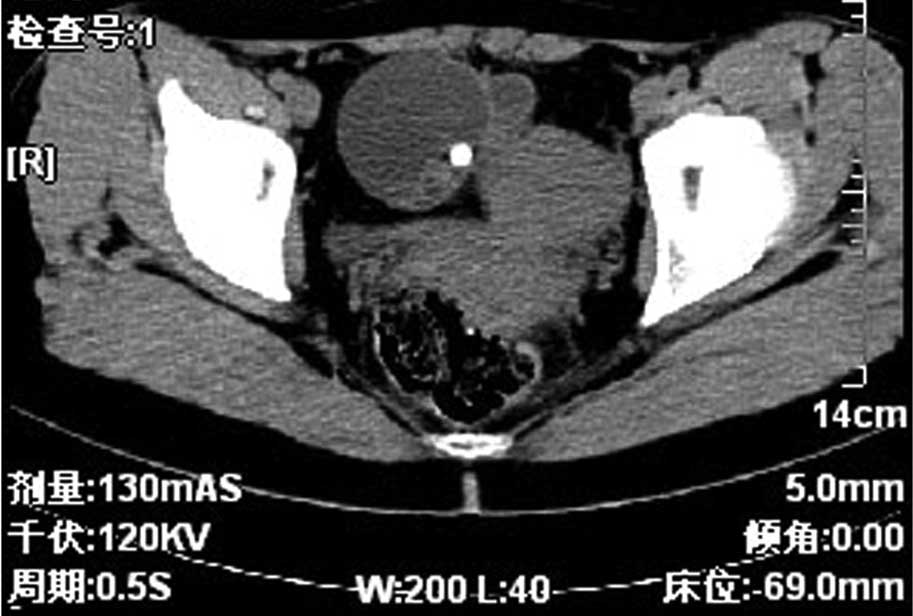
and 2). A pelvic computed
tomography (CT) scan revealed a 6×4.5 cm cystic mass in the left
pelvis, which was suspected to represent a cystic teratoma of the
left ovary (Fig. 3). The density of
the uterine body was irregular as shown by enhanced B sonography,
which did not eliminate the presence of uterine disease.
Surgical procedures
The patient underwent surgery with a diagnosis of
cystic teratoma of the left ovary, incomplete uterine mediastinum
and infertility. At the time of surgery, incomplete mediastinum (∼2
mm) was observed at the bottom of the uterus. The left fallopian
tube appeared to be distended by ∼8×3 cm, and contained
cream-colored sebaceous material and hair. The left ovary and the
right adnexa were normal. The patient subsequently underwent left
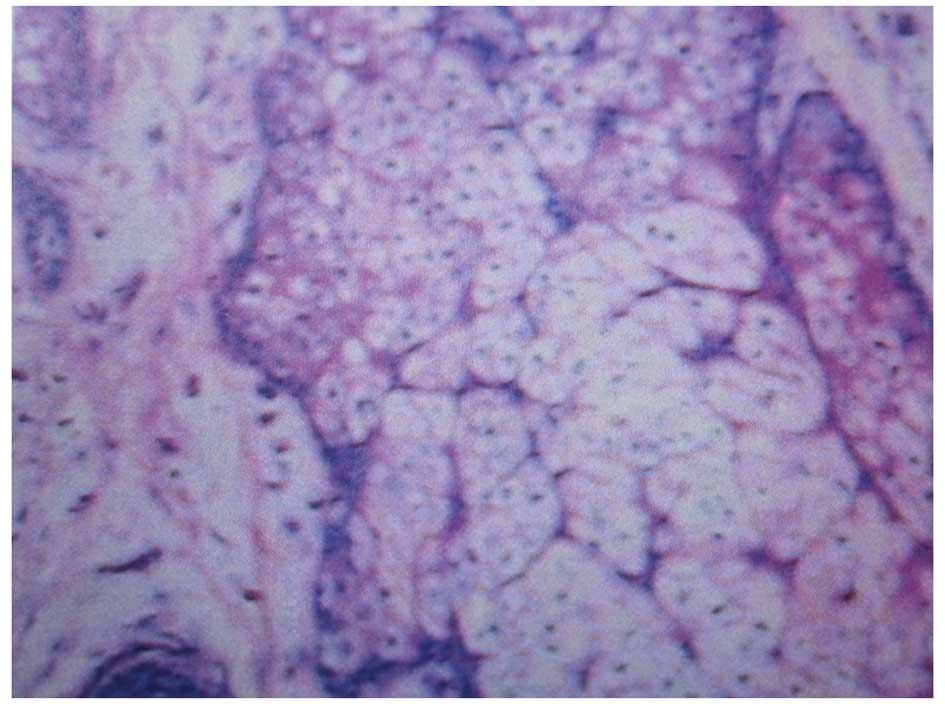
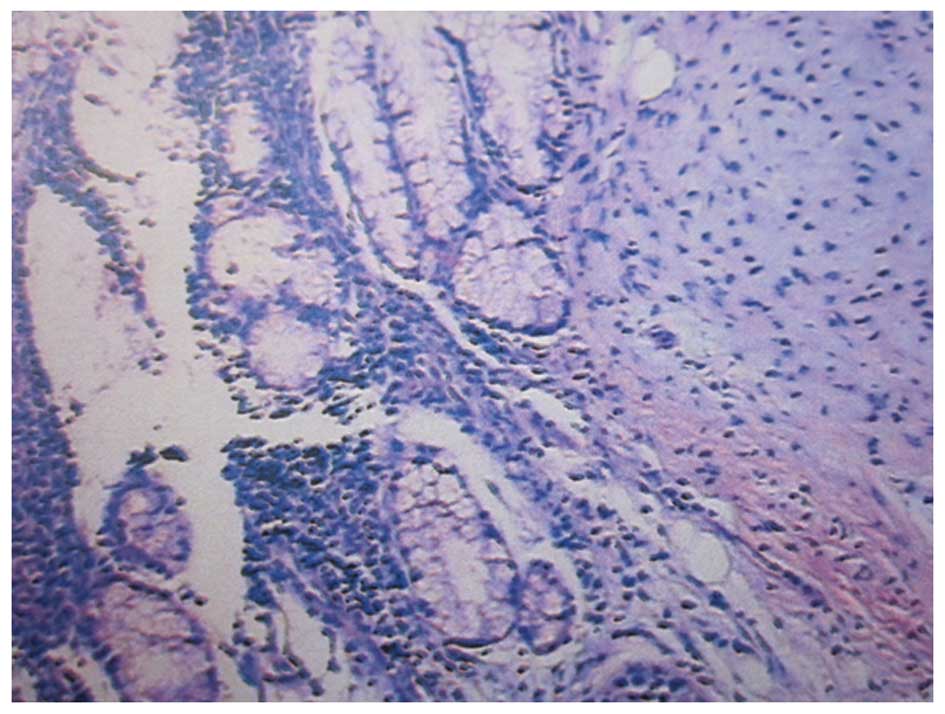
salpingectomy and uterine septum incision. The post-operative
recovesry was uneventful. The ampullary portion of the left
fallopian tube was histologically diagnosed as mature cystic
teratoma (Figs. 4 and 5).
Discussion
Tubal teratoma may be associated with other
neoplasms (6,7), struma ovarii, ectopic pregnancy
(8,9), uterine leiomyomatosis (10) and endometrial adenocarcinoma
(11) (Table I). The present case study is the
first in the literature to report a mature cystic teratoma of the
fallopian tube associated with incomplete uterine mediastinum
(11). In addition, the teratoma in
the present case was the largest of all reported cases of mature
cystic teratomas of the fallopian tube. The diversity of teratoma
behavior is likely to reflect the varied biological potential of
different stem cells, including germ and pluripotent embryonic
cells. Benign teratoma of the fallopian tube is composed of tissues
of ectodermal, mesodermal and endodermal origin in any combination
(1). Teratomas are initially of
mesodermal origin with abundant mesenchymal stroma; however, it
eventually develops endodermal and ectodermal derivatives with
airway-lining enterocytes, thyroid, brain and skin appendages
(12). The majority of cases of
benign teratoma of the fallopian tube occur in patients in their
40s and are cystic and exhibit significant variations in size. The
majority of benign teratomas of the fallopian tube are unilateral
and are common in 1/3 of the fallopian tube or the outer edge of
the fallopian tube. The tumors tend to be small and contain
sebum-like material with hairs. Fallopian tube teratomas have been
associated with reduced parity, menstrual irregularity, leukorrhea,
post-menopausal bleeding and abdominal pain. Procedures, including
analysis of serum C12 levels, pelvic CT scan, ultrasound
examination (13) and
hysterosalpingography (12), are
useful for diagnosis. The prognosis of the disease is good. In the
present case, the patient was 23 years-old; however, the teratoma
was larger compared with other studies (14–19).
The majority of tubal teratomas are benign. In the current case,
the patient suffered from incomplete uterine mediastinum, which was
due to paramesonephric duct convergence insufficiency. Intermittent
lower abdominal pain has been reported in other cases, consistent
with the current case; however, the patient was originally admitted
to hospital due to infertility. One year following the surgery, the
individual became pregnant.
 | Table I.Tubal teratomas in the literature. |
Table I.
Tubal teratomas in the literature.
| First author
(ref.) | Complication | Age, years | Graviditya and parity | Side | Size, cm | Other |
|---|
| Baginski | Ectopic
pregnancy | 33 | G2P2 | L | Egg | Increased hCG |
| Roberts | Ectopic
pregnancy | 29 | G0P0 | L | 4×2 | Increased hCG |
| Neumann | Ectopic
pregnancy | 36 | G0P0 | L | 3.4×1 | Increased hCG |
| Zelinger | Ectopic
pregnancy | 30 | G2P2 | L | 1×1.5 | Increased hCG |
| Massouda | Ectopic
pregnancy | 24 | G0P0 | R | 2.5×1 | Increased hCG |
| Kutteh | Ectopic
pregnancy | 25 | G3P3 | L | 2×2 | Increased hCG |
| Chao | Uterine
leiomyomatosis | 40 | G6P2 | L | 4.0×2.2×1.2 | Normal C12 |
| Hoda | Struma salpingis | 44 | | L | 0.2 | A 7.0-cm mucinous
cystadenoma of the contralateral ovary |
| Roncati | Endometrial
adenocarcinoma | 67 | G4P4 | L | 0.5×0.6 | |
| PC | Incomplete uterine
Mediastinum | 23 | G0P0 | L | 8×3 | Normal C12 |
In conclusion, benign teratomas commonly occur in
the ovaries, but are rarely found in the fallopian tubes. Although
the present case was a cystic teratoma, immature tissues were not
identified by microscopic examination of the specimens by several
pathologists. Therefore, a diagnosis of a benign mature cystic
teratoma originating in the fallopian tube was reported for this
patient.
References
|
1.
|
Mutter GL: Teratoma genetics and stem
cells: a review. Obstet Gynecol Surv. 42:661–670. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Norris HJ, Zir HJ and Barson WL: Immature
(malignant) teratoma of the ovary: a clinical and pathologic study
of 58 cases. Cancer. 37:2359–2372. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Corfman PA and Richart RM: Chromosome
number and morphology of benign cystic teratoma. N Engl J Med.
271:1241–1244. 1964. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Rashad MN, Fathalla RM and Kerr MG: Sex
chromatin and chromosome analysis in ovarian teratomas. Am J Obstet
Gynecol. 96:461–465. 1966.PubMed/NCBI
|
|
5.
|
Linder D, McCaw BK and Hecht F: Pathogenic
origin of benign ovarian teratoma. N Engl J Med. 292:63–66. 1975.
View Article : Google Scholar
|
|
6.
|
Hoda SA and Huvos AG: Struma salpingis
associated with struma ovarii. Am J Surg Pathol. 17:1187–1189.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Mazzarella P, Okagaki T and Richart RM:
Teratoma of the uterine tube. Obstet Gynecol. 39:381–388.
1972.PubMed/NCBI
|
|
8.
|
Pai MR, Naik R and Baliga P: Mature cystic
teratoma of the fallopian tube associated with ectopic pregnancy. J
Indian Med Assoc. 95:881997.PubMed/NCBI
|
|
9.
|
Kutteh WH and Albert T: Mature cystic
teratoma of the fallopian tube associated with an ectopic
pregnancy. Obstet Gynecol. 78:984–986. 1991.PubMed/NCBI
|
|
10.
|
Chao TJ, Chao J, Kuan LJ, Li YT, Kuo TC,
Chang YC and Nieh S: Mature solid teratoma of the fallopian tube
associated with uterine leiomyomas. J Chin Med Assoc. 71:425–427.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Roncati L, Barbolini G, Ghirardini G and
Rivasi F: Mature solid teratoma of the fallopian tube mimicking
metastasis of endometrial adenocarcinoma: a case report. Int J Surg
Pathol. 18:561–563. 2010.PubMed/NCBI
|
|
12.
|
Fujiwara S, Yamashita Y, Yoshida Y, Terai
Y, Okuda K and Ohmichi M: Mature cystic teratoma of the fallopian
tube. Fertil Steril. 94:2708–2709. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Johnson C and Hansen KA: Mature cystic
teratoma of the fallopian tube. Fertil Steril. 86:995–996. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Yoshioka T and Tanaka T: Mature solid
teratoma of the fallopian tube: case report. Eur J Obstet Gynecol
Reprod Biol. 89:205–206. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Baginski L, Tazigi R and Sandstad J:
Immature (malignant) teratoma of the fallopian tube. Am J Obstet
Gynecol. 160:671–672. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Roberts D: A case of ectopic gestation
removal, by abdominal section with a dermoid tumor of the extremity
of the left tube. Lancet. 2:1164–1165. 1903.
|
|
17.
|
Neumann HO: Teratoma der tube. Arch
Gynaekol. 130:766–774. 1927.(In German).
|
|
18.
|
Zelinger BB, Grinvalsky HT and Fields C:
Simultaneous dermoid cyst of the tube and ectopic pregnancy. Obstet
Gynecol. 15:340–343. 1960.PubMed/NCBI
|
|
19.
|
Massouda D, Wortham GF III and Oakley JL:
Tubal pregnancy associated with a benign cystic teratoma of the
fallopian tube. A case report. J Reprod Med. 33:563–564.
1988.PubMed/NCBI
|