Introduction
Orthotopic ileal neobladder construction following
radical cystectomy is accepted as a novel method of urinary
diversion. To date, numerous types of neobladders have been
reported (1–5). The reservoir should be detubularized
and compliant with a low end filling pressure (6,7).
Daytime and night-time urinary incontinence, urethral or
anastomotic strictures and a failure to empty the bladder
substitute, thus requiring intermittent or permanent
catheterization, may distract substantially from any perceived
quality of life advantages of an orthotopic bladder reconstruction
(8,9). The present study aimed to compare the
early and late urodynamic assessment of the orthotopic N-shaped
neobladder in patients who had undergone a radical cystectomy and
ileal bladder substitution for muscle-invasive bladder cancer and
to provide urodynamic evidence for the improvement of this
technique.
Materials and methods
Patients and surgical technique
A total of 52 male patients with muscle-invasive
bladder cancer who fulfilled the WHO bladder cancer criteria (2004
revision) were enrolled in the present study (10). The 52 patients with bladder cancer
were confirmed using pathology examinations. The patients underwent
a radical cystectomy and orthotopic N-shaped neobladder
substitution and were scheduled for early (3 months) and late (12
months) urodynamic evaluations. Of the 52 patients, 6 succumbed to
cancer, leaving 46 patients available for the early and late
evaluations. The staging of the muscle-invasive bladder cancer was
assessed using the TNM staging system for bladder cancer revised by
the American Joint Committee On Cancer (AJCC) (11). All the patients were clinically
staged as N0M0 pre-operatively by computerized tomography (Philips,
Amsterdam, Holland) of the abdomen/pelvis, chest X-ray (Siemens,
Munich, German) and nuclear bone scan (Siemens). The mean age of
the patients was 60.9 years. Uroflowmetry, cystometry and urethral
pressure profilometry were analyzed at 3–12 months following the
surgery. Females were excluded from this analysis since the number
of females with muscle-invasive bladder cancer is small, which may
affect the functional outcome. All the patients provided their
written informed consent prior to the initiation of the study.
All the cystectomies and bladder substitutions were
performed as previously described by Zhou et al(12). A 35-cm ileal segment was isolated
15–20 cm proximal to the ileocecal valve (Fig. 1). The length of the intestinal
segment that was used for the reservoir was recorded at the
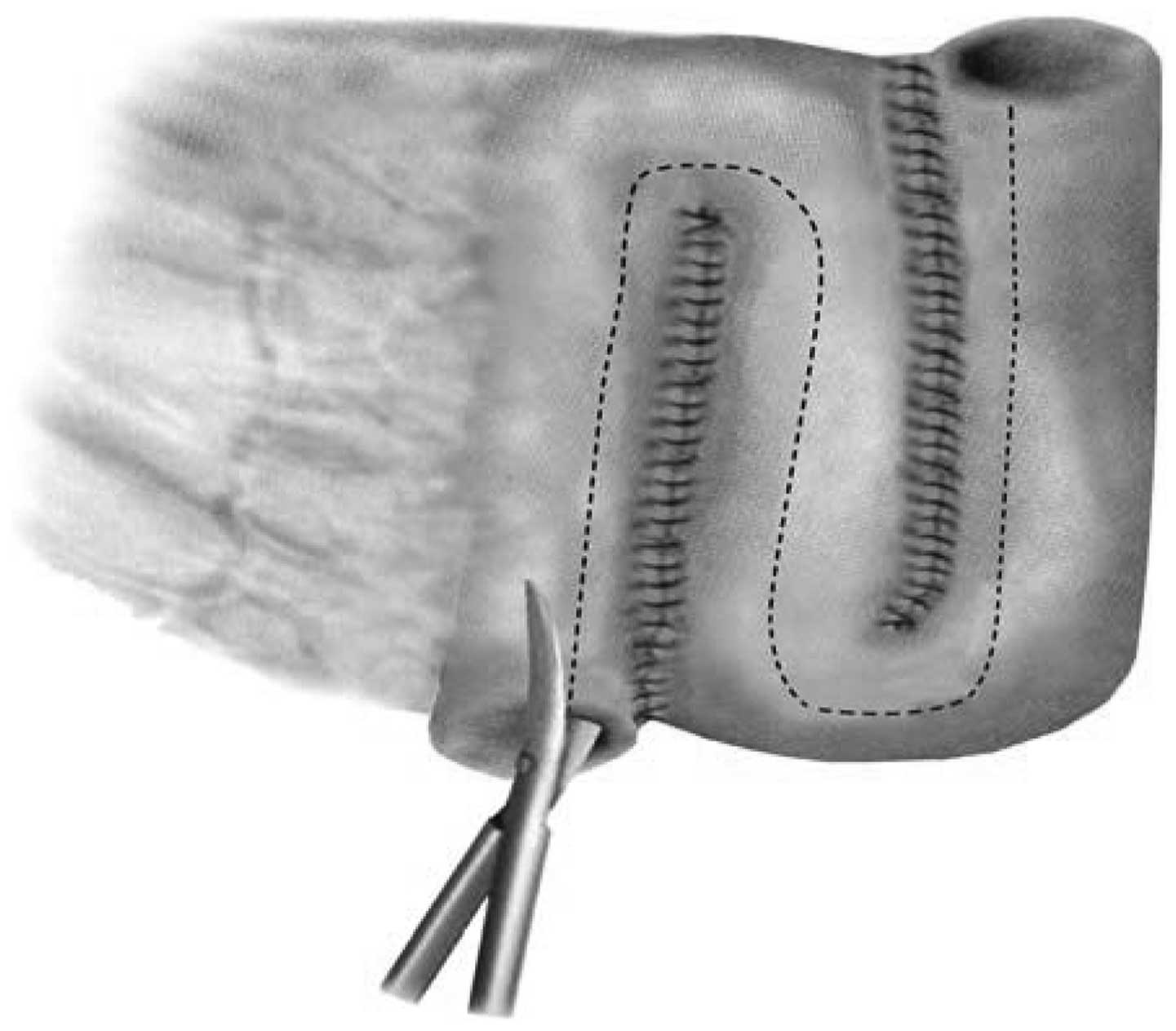
surgery. The distal loop (~35 cm in length) was lowered in an N
shape. The ileal segment was then split open along the
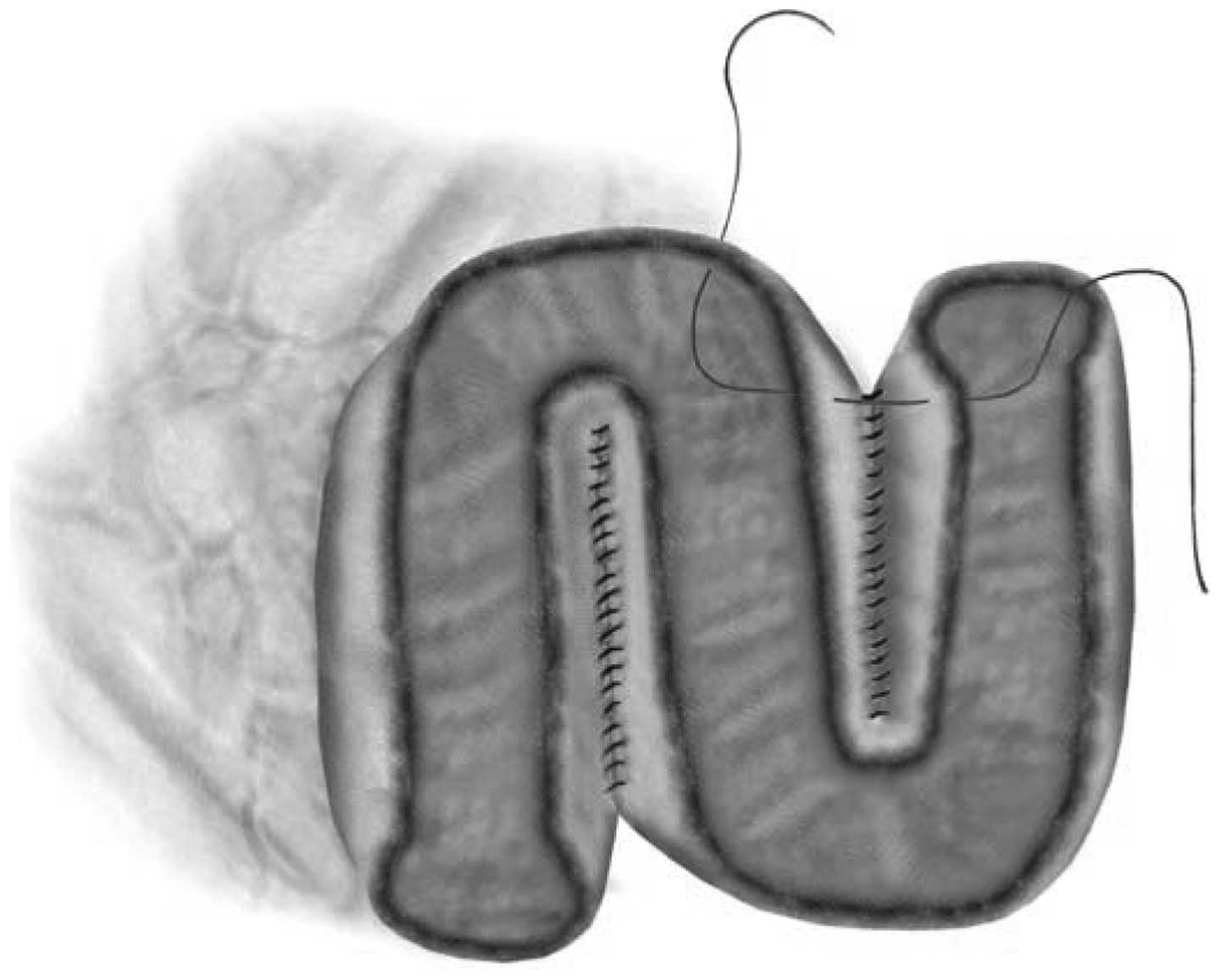
antimesenteric border (Fig. 2). The
proximal loop was folded in a reversed N shape and the inner
opposite borders were then sutured side-to-side. This was tied to
the opposite edge of the lower ileal segment to obtain an oval
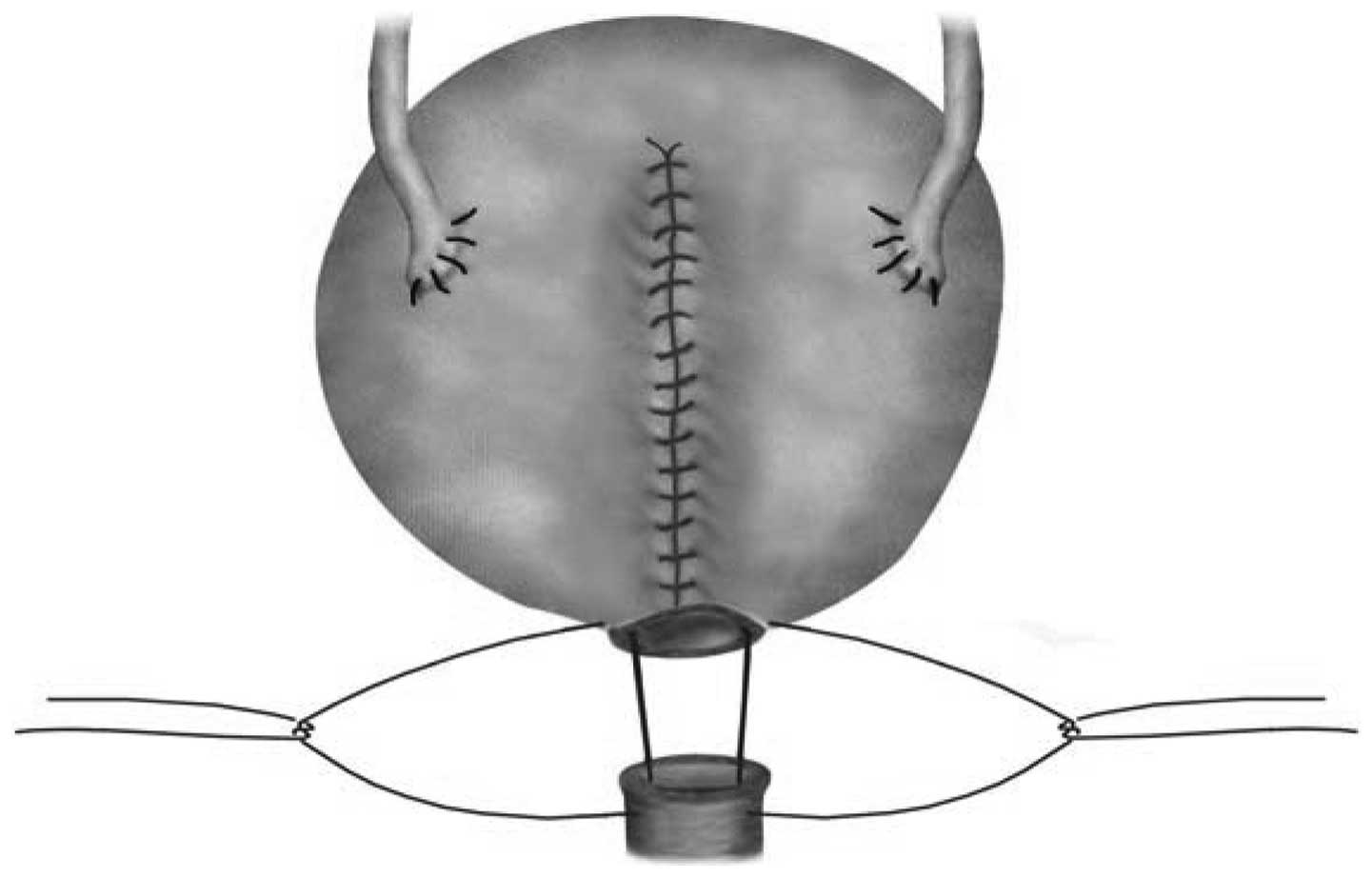
refashioned reservoir (Fig. 3). A
ureteroileal anastomosis was performed bilaterally using the Nesbit
technique in an open end-to-side fashion (Fig. 4).
Urodynamic studies
The urodynamic analysis was performed using the
BONITO UDS600 Urodynamic system (Laborie, Ontario, Canada). The
urodynamic studies consisted of uroflowmetry, cystometry, urethral
pressure profilometry and post-void residual (PVR) urine volume
determination. Following the placement of a 10F transurethral dual
channel catheter and a 10F rectal balloon catheter (Laborie,
Mississauga, ON, Canada), the neobladder was filled at a rate of 50
ml/min with saline solution (Qingdao Huaren Pharmaceutical Co.,
Ltd., Qingdao, China) at room temperature. Uroflowmetry, cystometry
and urethral pressure profilometry were analyzed at 3–12 months
following the surgery. The parameters that were evaluated were the
neobladder capacity, the pressure at the maximal capacity, urine
leakage, the presence, amplitude and number of intrinsic
contractions, the PVR urine volume and the urethral pressure
profile. The maximum urine flow rate (Qmax) was measured
by uroflowmetry. The early (3, 6 and 9 months) and late (12 months)
urodynamic results were compared.
Follow-up
Each patient was followed up at 3, 6, 9 and 12
months post-operatively and then yearly in a prospective protocol
that included clinical, metabolic and radiological assessment from
the standpoint of the oncological follow-up and lower urinary tract
function. In the case of elevated serum creatinine levels or
hydronephrosis, a renal scan using technetium-99m
(99mTc)-diethylenetriamine-pentaacetic-acid was
performed.
To assess the lower urinary tract function in
detail, voiding and continence diaries (frequency/volume chart for
2–3 days) and a standardized questionnaire were completed at 3, 6,
9 and 12 months following the surgery and annually thereafter. The
questionnaire assessed the presence and degree of daytime and
night-time urinary incontinence; described as mucus only, few
drops, a spoonful, approximately half a glass, a glass full and
almost all. The questionnaire also analyzed the frequency of
daytime and night-time urinary incontinence episodes and the number
of absorbent pads used day and night. Full continence was defined
as daytime and night-time dryness without the requirement for a pad
or condom catheter.
Statistical analysis
The statistical analysis was performed using SPSS
13.0 software (SPSS, Inc., Chicago, IL, USA). The correlation
analysis was performed using the Pearson correlation test. The data
are expressed as the mean ± standard deviation. P<0.05 was
considered to indicate a statistically significant difference
between the early and late urodynamic assessments.
Results
The mean age of the patients was 60.9±7.6 years
(range, 49–72 years). The mean pressure of the neobladders was
<15 cm H2O at volumes of <400 ml and 22.4 cm
H2O at 100% capacity at 6 months. The mean pressure of
the contractions was <40 cm H2O at 6 months. The mean
filling pressure following the surgery was relatively stable. The
results demonstrated that the mean filling pressure levels were
significantly higher at 3 months than at 6 months following the
surgery. The differences between the levels at 6, 9 and 12 months
showed no statistical significance. When comparing the urodynamic
characteristics at 9 months with those at 12 months, no significant
changes were observed in the cystometric capacity. The mean PVR
volume was 58 ml. A mean voiding peak of 16.2 ml/sec was obtained
using the Valsalva maneuver. The daytime and night-time continence
rates were 90 and 60%, respectively, at 12 months. The
questionnaires concerning the quality of life revealed no
difference between the patient group and healthy group. The
urodynamic evaluation is shown in Table
I.
 | Table IUrodynamic evaluation of 46 male
patients. |
Table I
Urodynamic evaluation of 46 male
patients.
| Follow-up
(months) |
|---|
|
|
|---|
| Urodynamic index | 3 | 6 | 9 | 12 |
|---|
| Maximum bladder
capacity (ml) | 386.0±46.6 | 403.5±49.7 | 414.9±45.0 | 444.9±97.0 |
| PVR urine volume
(ml) | 41.3±10.6 | 38.5±4.6 | 36.2±8.9 | 32.4±7.9 |
| Flow (ml/sec) | 14.0±2.0 | 16.2±2.2 | 17.6±4.8 | 19.9±2.6 |
| Pressure at maximum
capacity (cm H2O) | 21.4±3.6 | 18.2±4.0 | 17.7±3.1 | 16.5±3.7 |
| Pressure at
Qmax (cm H2O) | 46.2±4.7 | 48.9±4.7 | 52.7±4.8 | 53.2±5.5 |
Discussion
Neobladder substitution has currently become the
standard for urinary diversion due to good long-term functional
results (13–15). Various segments of bowel have been
used extensively for bladder augmentation or replacement, including
detubularized ileum, detubularized sigmoid colon and the right
colon with or without a patch of ileum. When measuring the quality
of life of patients with orthotopic bladder substitutions,
functional voiding is a significant factor (8,9). The
present study aimed to compare the early and late urodynamic
assessments of the orthotopic N-shaped neobladder in patients who
had undergone a radical cystectomy and ileal bladder substitution
for muscle-invasive bladder cancer and to provide urodynamic
evidence for the improvement of this technique.
The success of orthotopic bladder substitutions to
store urine, and thus provide urinary continence, relies on a
sufficient functional reservoir capacity, detubularization of the
intestinal segment to reduce intravesical pressure and the
preservation of the external urethral sphincter tonus (6,7). The
reservoir should be detubularized and compliant with a low end
filling pressure (6,7). The detubularization and overfolding of
the ileal segment creates the maximum radius that concomitantly
results in a four-fold increase in the volume. The mathematical
model offered by Hinman (16) and
animal studies conducted by Shaaban et al(17) have shown that the mainstay of
creating a low-pressure, high-volume reservoir is by the
detubularization and reconfiguration of the intestinal segments. In
the present study, the mean maximum cystometric pouch capacity was
526 ml and the pressure levels during the filling phase of the
orthotopic bladder were relatively low. Only a 30-cm ileal segment
was used for the reconstruction of the neobladder. Compared with
other procedures, the length of the intestinal segment that was
used for the reservoir was the shortest. The mean pressure of
contractions was <40 cm H2O. In a native bladder, the
pressures are usually <5–10 cm H2O during the filling
cystometry. However, in a neobladder of intestinal origin, it is
accepted that pressures of up to 40 cm H2O may be safely
tolerated in terms of preserving the upper urinary tract functions.
Therefore, with its low pressure, the N-shaped neobladder appears
to present no risk to the upper urinary tract. The present study
identified that the mean filling pressure following the surgery was
relatively stable, with the exception of at 3 and 6 months. The
differences between the 6-, 9- and 12-month time-points showed no
statistical significance. In the present study, the maximal
capacity was stable at 6 and 12 months and the PVR urine volume was
<100 ml in the majority of the cases, thus showing that the
reservoir capacity remained stable at 6 months. The high compliance
of the ileal neobladder is the main factor in achieving near-normal
voiding patterns and preserving the upper urinary tract. Bachor
et al(18) stated that high
compliance levels were associated with the preservation of the
upper urinary tract with a pouch pressure of 25 cm H2O.
In the present study, the group mean Qmax value and PVR
urine volume were 16.2 ml/sec and 58 ml, respectively.
Overdistension with a loss of wall tension should be avoided, as it
may produce incomplete emptying. Porru et al(19) observed that only patients with a
capacity of >700 ml had a significant PVR urine volume (>100
ml). In the present study, the maximal capacity was stable at 6
months and the PVR urine volume was <100 ml in the majority of
the cases.
In the present study, orthotopic neobladder
replacement following radical cystectomy was well accepted by the
patients and provided a good health-related quality of life as a
result of a near-normal daytime and night-time continence status.
Continence following orthotopic urinary diversion is dependent on
an intact urethral sphincter function and an intact pelvic floor,
which are able to maintain a resistance pressure across the
urethral continence zone that exceeds the pressure generated within
the diversion (9,20,21).
Additional factors that may affect continence include the urethral
length and sensitivity, the patient age and mental status, an
intact pelvic nerve supply to the rhabdosphincter, the completeness
of voiding and the presence or absence of bacteriuria (22). Early (median follow-up, 9 months)
and long-term (median follow-up, 62 months) daytime continence
rates have been reported as 80 and 90% (23), respectively. In the present study,
the daytime continence rate was 90%, which is in parallel with
other studies.
The night-time incontinence of a neobladder occurs
due to the absence of a neurological feedback and sphincter
detrusor reflex, the relaxation of the pelvis and a decreased
sphincter tonus at night (9). The
night-time continence rate in the present study was 60% and
therefore below the rates that have been reported in other studies
(18,21). Nocturnal continence has a
statistically significant positive correlation with the maximal
urethral closure pressure and a negative correlation with the
maximal contraction amplitude and the pressures at mid- and maximal
capacity (24). Age is also a
contributing factor in the establishment of continence. Careful
patient selection is as significant as the surgical technique that
is applied during the bladder substitution procedure in order to
achieve a good continence status. To reduce enuresis, patients may
be instructed to limit fluid intake following an evening meal, to
void prior to going to sleep and to set on an alarm clock to awaken
and void once or twice during the night. This education is aimed at
reactivating the perception of the desire to void during sleep to
obtain an improved control of the neobladder (23).
With regard to the quality of life of the patient,
no evidence has been identified to support an advantage of one type
of orthotopic reconstruction over another (25). In the present study, the majority of
the aspects of life quality, including the urinary symptoms and
continence rate, were evaluated using the European Organisation for
Research and Treatment of Cancer (EORTC) QLQ-C30 and BLM30
questionnaires and the results were judged as excellent.
In the present study, the orthotopic N-shaped
neobladder maintained stable urodynamic parameters and function and
was associated with a good quality of life. The urodynamic
parameters of the neobladder were similar to those of a normal
urinary bladder. The construction of an orthotopic continent
globular ileal bladder required a shorter ileal segment compared
with those of other similar procedures. According to the present
data, the orthotopic N-shaped neobladder is a valid treatment
option for treating muscle-invasive bladder cancer.
References
|
1
|
Burkhard FC, Kessler TM, Springer J and
Studer UE: Early and late urodynamic assessment of ileal orthotopic
substitutes combined with an afferent tubular segment. J Urol.
175:2155–2161. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pagano F, Artibani W, Ligato P, Piazza R,
Garbeglio A and Passerini G: Vescica ileale Padovana: a technique
for total bladder replacement. Eur Urol. 17:149–154.
1990.PubMed/NCBI
|
|
3
|
Lee KS, Montie JE, Dunn RL and Lee CT:
Hautmann and Studer orthotopic neobladders: a contemporary
experience. J Urol. 169:2188–2191. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hautmann RE, de Petriconi R, Gottfried HW,
Kleinschmidt K, Mattes R and Paiss T: The ileal neobladder:
complications and functional results in 363 patients after 11 years
of follow up. J Urol. 161:422–428. 1999.PubMed/NCBI
|
|
5
|
Steven K and Poulsen AL: The orthotopic
Kock ileal neobladder: functional results, urodynamic features,
complications and survival in 166 men. J Urol. 164:288–295. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Studer UE and Zingg EJ: Ileal orthotopic
bladder substitutes. What we have learned from 12 years’ experience
with 200 patients. Urol Clin North Am. 24:781–793. 1997.PubMed/NCBI
|
|
7
|
Burkhard FC and Studer UE: Orthotopic
bladder substitution. Curr Opin Urol. 10:343–349. 2000. View Article : Google Scholar
|
|
8
|
Weijerman PC, Schurmans JR, Hop WC,
Schröder FH and Bosch JL: Morbidity and quality of life in patients
with orthotopic and heterotopic continent urinary diversion.
Urology. 51:51–56. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Steers WD: Voiding dysfunction in the
orthotopic neobladder. World J Urol. 18:330–337. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Eble JN, Sauter G, Epstein JI, et al; The
International Agency for Research on Cancer, . WHO Classification
of Tumours: Pathology and Genetics of Tumours of the Urinary System
and Male Genital Organs. 1st edition. IARC Press; Lyon, France:
2004
|
|
11
|
Edge SB, Byrd DR, et al: AJCC Cancer
Staging Manual. 7th edition. Springer; New York, NY: 2010
|
|
12
|
Zhou RX, Yang JY, Zhang XS, et al: In situ
continent globular ileal neobladder (report of 26 cases). Chin J
Urol. 23:464–466. 2002.
|
|
13
|
Hautmann RE, Volkmer BG, Schumacher MC,
Gschwend JE and Studer UE: Long-term results of standard procedures
in urology: the ileal neobladder. World J Urol. 24:305–314. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Studer UE, Burkhard FC, Schumacher M, et
al: Twenty years experience with an ileal orthotopic low pressure
bladder substitute - lessons to be learned. J Urol. 176:161–166.
2006.PubMed/NCBI
|
|
15
|
Miyake H, Furukawa J, Takenaka A, Yamanaka
N and Fujisawa M: Long-term functional outcomes in patients with
various types of orthotopic intestinal neobladder. Int J Urol.
15:612–615. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hinman F Jr: Selection of intestinal
segments for bladder substitution: physical and physiological
characteristics. J Urol. 139:519–523. 1988.PubMed/NCBI
|
|
17
|
Shaaban AA, el-Nono IH, Abdel-Rahman M and
Ghoneim MA: The urodynamic characteristics of different ileal
reservoirs: an experimental study in dogs. J Urol. 147:197–200.
1992.PubMed/NCBI
|
|
18
|
Bachor R, Frohneberg D, Miller K, Egghart
G and Hautmann R: Continence after total bladder replacement:
urodynamic analysis of the ileal neobladder. Br J Urol. 65:462–466.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Porru D, Dore A, Usai M, et al: Behaviour
and urodynamic properties of orthotopic ileal bladder substitute
after radical cystectomy. Urol Int. 53:30–33. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hautmann RE: Urinary diversion: ileal
conduit to neobladder. J Urol. 169:834–842. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Light JK: Continence mechanisms following
orthotopic bladder substitution. Scand J Urol Nephrol Suppl.
142:95–97. 1992.PubMed/NCBI
|
|
22
|
World Health Organization (WHO) Consensus
Conference on Bladder Cancer. Hautmann RE, Abol-Enein H, Hafez K,
et al: Urinary diversion. Urology. 69(1 Suppl): S17–S49. 2007.
View Article : Google Scholar
|
|
23
|
Varol C and Studer UE: Managing patients
after an ileal orthotopic bladder substitution. BJU Int.
93:266–270. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Koraitim MM, Atta MA and Foda MK:
Orthotopic bladder substitution in men revisited: identification of
continence predictors. J Urol. 176:2081–2084. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gerharz EW, Månsson A, Hunt S, Skinner EC
and Månsson W: Quality of life after cystectomy and urinary
diversion: an evidence based analysis. J Urol. 174:1729–1736. 2005.
View Article : Google Scholar : PubMed/NCBI
|