Introduction
Rectal cancer is the common cause of cancer-related
mortality in the United States, with ~40,290 new cases in 2012
(1). Rectal tumors spread locally
and metastasize to distant sites. The liver is the most common site
of metastasis, followed by the regional lymph nodes, lungs and bone
(2). The most important prognostic
factor in rectal adenocarcinoma is the stage of the tumor, which
also indicates the therapeutic strategy. However, accurate
detection of rectal carcinoma remains a diagnostic challenge.
Although surgery is the most effective primary treatment for rectum
carcinoma patients in early stage, it may not be suitable for
patients with disseminated metastasis. Therefore, due to incorrect
staging, certain patients with disseminated disease may be
subjected to unnecessary surgery that may result in considerable
morbidity (3). By detecting disease
and predicting resectability, positron emission tomography-computed
tomography (PET-CT) offers an efficient means to manage such
patients. A PET-CT scanner combines PET and CT cameras, and is a
new device with significant diagnostic potential. Compared with PET
alone, PET-CT shows significant increase in the certainty of lesion
localization and characterization of rectal adenocarcinoma
(4).
Case report
A 67-year-old male, diagnosed with stage III rectal
adenocarcinoma, was admitted to West China Hospital (Chengdu,
China) for abdominal rectal resection in May 2010. Postoperative
pathological examination indicated mucosal adenocarcinoma, invading
the whole intestinal wall and tumor cells were identified in 4/4
mesenteric lymph nodes.
The patient was treated by chemotherapy with
oxaliplatin, calcium folinate and fluorouracil every 14 days for
seven cycles. In March 2011, PET-CT revealed a left lower lobe
nodule with mildly increased glucose metabolism. The largest
standardized uptake value (SUV) was 2.38, which exhibited
metastatic possibility. The pulmonary nodule was surgically removed
and the postoperative pathological diagnosis was a poorly
differentiated adenocarcinoma arising from primary rectal
adenocarcinoma. The tumor was diagnosed as invading the visceral
pleura and immunohistochemical staining showed caudal-type homeobox
transcription factor 2 (CDX-2)(+), mucin-1(+), cytokeratin 7
(CK7)(+) and thyroid transcription factor-1 (TTF-1)(−) in the tumor
cells (Fig. 1).
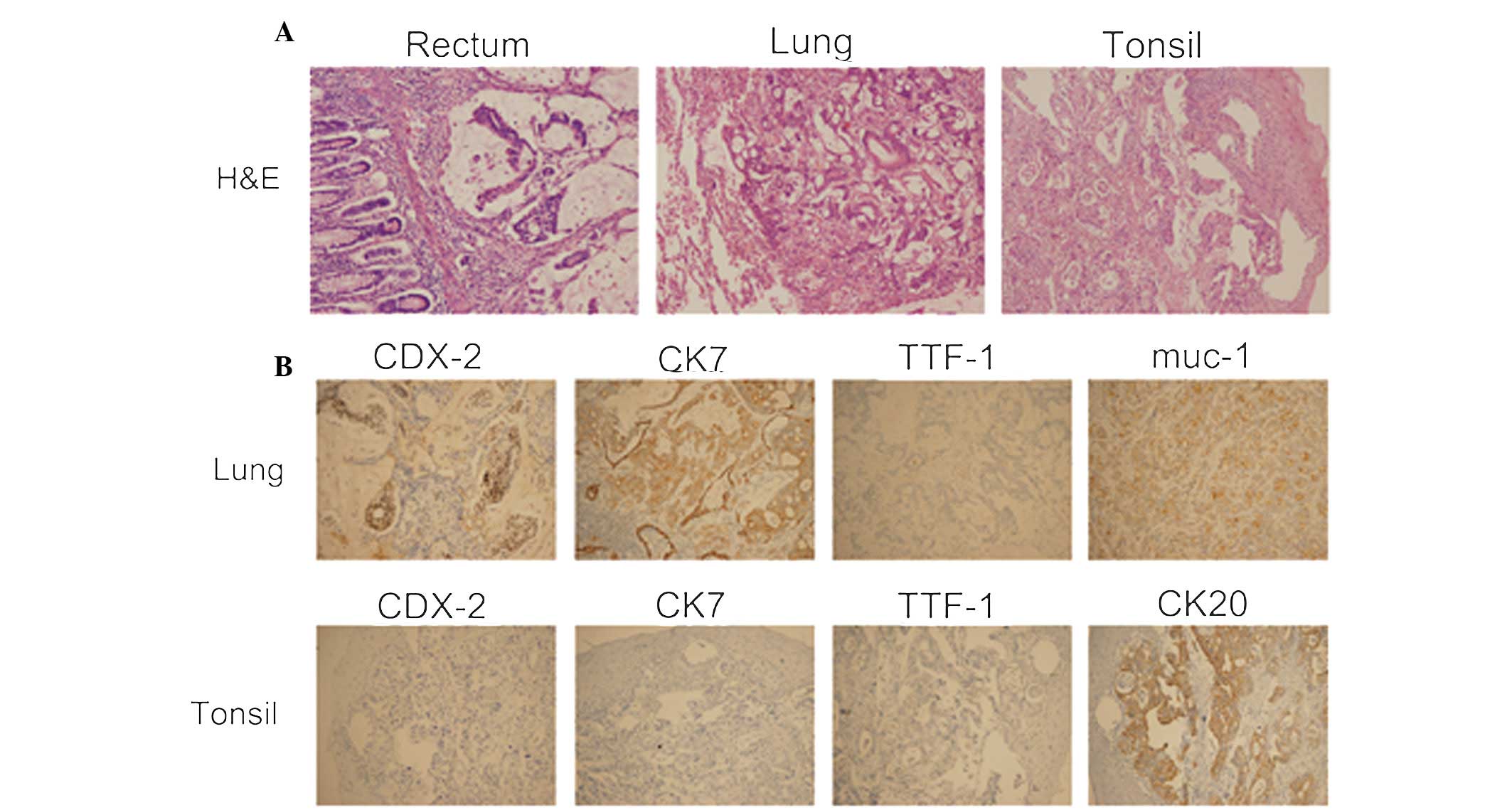 | Figure 1(A) Hematoxylin and eosin staining of
the tumor cells in the rectum, lung and tonsil. (B)
Immunohistochemical staining of the lung showed CDX-2(+), muc-1(+),
CK7(+) and TTF-1(−) in the tumor cells. Immunohistochemical
staining of the tonsil showed CDX-2(−), CK20(+), CK7(−) and
TTF-1(−) in the tumor cells, confirming metastasis from colorectal
adenocarcinoma (magnification, ×400). CDX-2, caudal type homeobox
transcription factor 2; muc-1, mucin-1; CK7, cytokeratin 7; TTF-1,
thyroid transcription factor-1. |
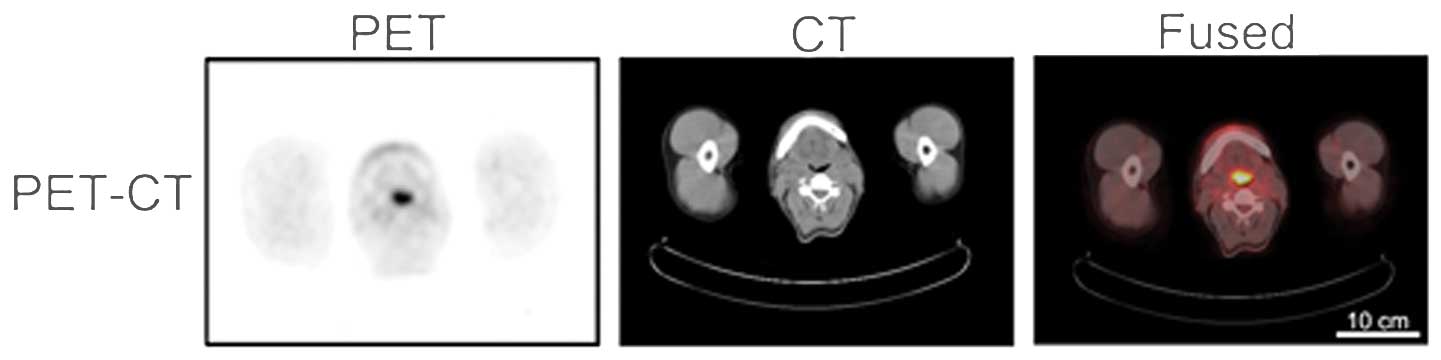
Subsequently, the patient was treated by
chemotherapy with 50 mg TS-1 twice daily. In November 2011, PET-CT
revealed that the tonsil was swollen and the largest SUV was 8.08
(Fig. 2). Pathological examination
was performed on the tonsil mass and the results indicated
adenocarcinoma. Immunohistochemical staining showed CDX-2(−),
CK20(+), CK7(−) and TTF-1(−) in the tumor cells, confirming
metastasis from colorectal adenocarcinoma (Fig. 1). The patient was then treated by
chemotherapy with irinotecan, calcium folinate and fluorouracil
every 14 days for four cycles; however, the patient succumbed to
progression of the disease.
Discussion
PET-CT scanning is important in oncology; functional
and anatomical images are captured in a single scanning process.
The PET-CT approach offers extensive possibilities for improving
the diagnosis of primary and metastatic tumors (5). In the present case report, the patient
denied any fever, pharyngalgia or night sweats. Thus, PET-CT was
considered to be the best tool to identify insidious metastasis,
improving radiotherapy planning and monitoring the effects of
chemotherapy.
Identification of the primary tumor site is a
challenging issue, which has prognostic and therapeutic
significance. In the current case report, PET-CT revealed a mass in
the left side of the tonsil. To identify the original site of the
tumor, immunohistochemistry was performed and the results indicated
a CK7(−)/CK20(+) phenotype, which confirmed colorectal carcinoma
(6).
Malignant tumors seldom metastasize to the oral
cavity. When this occurs, such metastasis is usually from various
organs, including the lung, breast and rectum. According to
previous studies, a few cases of metastatic localization have been
identified from the colon and rectum, including the gingival,
alveolar mucosa and tongue (7–9). The
current case report presents a case of a 67-year-old male with
tonsil metastasis from rectal adenocarcinoma. To the best of our
knowledge, this is the first recorded instance of tonsil metastasis
from rectal adenocarcinoma.
Since inflammatory and reactive lesions are common
in the oral cavity, it is challenging to diagnose the rare case of
rectal metastatic tumors in the tonsil. Occasionally, patients with
tonsil metastasis clinically mimic patients with the primary tonsil
neoplasm or tonsillitis. Therefore, it must be considered in the
differential diagnosis of patients with unexplained pharyngalgia
and antiadoncus. Careful examination, as well as a
multidisciplinary approach, is recommended to validate the clinical
suspicion. In conclusion, the current case report presents a unique
case of tonsil metastasis from rectal adenocarcinoma and the
oncologist must recognize the possibility of tonsil metastasis from
malignant disease, such as colorectal cancer.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar
|
|
2
|
Welch JP and Donaldson GA: The clinical
correlation of an autopsy study of recurrent colorectal cancer. Ann
Surg. 189:496–502. 1979.PubMed/NCBI
|
|
3
|
Delbeke D, Vitola JV, Sandler MP, Arildsen
RC, Powers TA, Wright JK Jr, Chapman WC and Pinson CW: Staging
recurrent metastatic colorectal carcinoma with PET. J Nucl Med.
38:1196–1201. 1997.PubMed/NCBI
|
|
4
|
Mottaghy FM, Sunderkötter C, Schubert R,
et al: Direct comparison of [18F]FDG PET/CT with PET alone and with
side-by-side PET and CT in patients with malignant melanoma. Eur J
Nucl Med Mol Imaging. 34:1355–1364. 2007.
|
|
5
|
Beyer T, Townsend DW, Brun T, Kinahan PE,
Charron M, Roddy R, Jerin J, Young J, Byars L and Nutt R: A
combined PET/CT scanner for clinical oncology. J Nucl Med.
41:1369–1379. 2000.PubMed/NCBI
|
|
6
|
Rubin BP, Skarin AT, Pisick E, Rizk M and
Salgia R: Use of cytokeratins 7 and 20 in determining the origin of
metastatic carcinoma of unknown primary, with special emphasis on
lung cancer. Eur J Cancer Prev. 10:77–82. 2001. View Article : Google Scholar
|
|
7
|
Davidson NG and Wilson A: Tongue
metastasis from adenocarcinoma of the rectum. J Laryngol Otol.
103:322–323. 1989. View Article : Google Scholar
|
|
8
|
Tomikawa M, Higuchi Y, Saku M, Takeshita
M, Yoshida K and Sugimachi K: Carcinoma of the colon metastatic to
the lower gingiva. Dig Surg. 18:333–335. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Torosian MH, Botet JF and Paglia M: Colon
carcinoma metastatic to the thigh - an unusual site of metastasis.
Report of a case. Dis Colon Rectum. 30:805–808. 1987. View Article : Google Scholar
|