Introduction
Pulmonary sarcomatoid carcinomas (SCs) are a
heterogeneous group of non-small cell lung carcinomas with a rare
histological subtype, and they have been reported to have a poor
prognosis (1–3,5). The
overall survival rate of pulmonary SC is significantly lower than
that for other non-small cell lung carcinomas (1,2,10). The
different types of pulmonary SC include pleomorphic carcinoma (PC),
spindle cell carcinoma, giant cell carcinoma, carcinosarcoma and
pulmonary blastoma (1). The
diagnosis of pulmonary SC is difficult using small biopsy specimens
and typically requires resection specimens (1). Pulmonary SC predominantly occurs in
males with a mean age of 60 years at diagnosis and who are heavy
smokers (1,2,4,6). PC,
the most common subtype of pulmonary SC according to the World
Health Organization classification of histological cancer, accounts
for 0.3% of all invasive lung malignancies of high grade with an
aggressive clinical course. The mean or median survival time of
patients with PC ranges from five to 35 months (1,2). This
subtype of SC tumor occurs more frequently in the thorax than do
true sarcomas. Written informed consent was obtained from the
patient’s family.
Case report
A previously healthy 46-year-old male presented with
progressive swelling and mass formation in the right popliteal
region. The patient had a three-month history of progressive
post-popliteal soreness and tightness behind the knee, particularly
when the knee was extended or fully flexed. The patient was
subsequently admitted to the Neurology Department of Tri-Service
General Hospital (Tapei, Taiwan). In March 2012, magnetic resonance
imaging (MRI) showed a large lobulated cystic mass filled with
debris or tissue thickening, measuring approximately 5.9×5.4×8.6 cm
over the popliteal fossa (Fig. 1).
The complete blood count results were as follows: White blood cell
count, 14.69×109/l; hemoglobin count, 96 g/l; platelet
count, 240×109/l; and serum calcium, 13.9 mg/dl. The
patient immediately underwent surgery for resolution of the
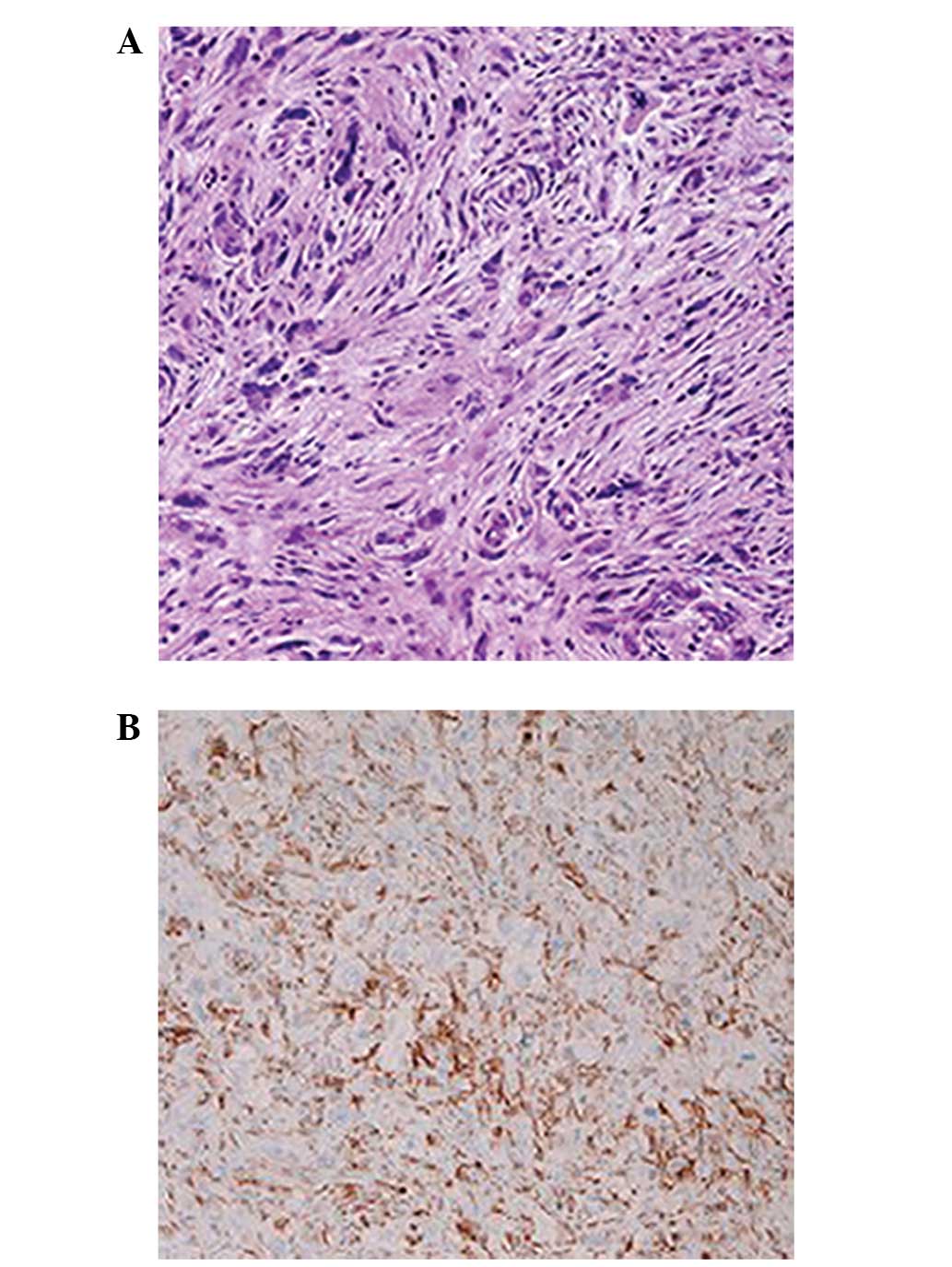
neurological symptoms. Pathological evaluation of the popliteal
mass showed a poorly differentiated carcinoma, with sarcomatoid
changes characterized by a solid and focal individual tumor
composed of marked pleomorphic tumor cells of the soft tissue
(Fig. 2A). Immunohistochemistry
showed that the popliteal mass was positive for Ki67, p53, p63 and
vimentin (Fig. 2B). The
morphological and immunohistochemical features were comparable with
those of metastatic SC. Fluorodeoxyglucose (FDG)-positron emission
tomography (PET) was performed immediately, and FDG uptake was
observed in the lungs and the right para-aortic and popliteal
regions. Based on these findings, the final histological diagnosis
was a pulmonary metastatic squamous cell carcinoma with sarcomatoid
changes and a pleomorphic subtype. Systemic chemotherapy was
initiated following diagnosis; it consisted of a combination of
cisplatin [(100 mg intravenous (i.v.) on day one)] and paclitaxel
(115 mg i.v. on day one and 130 mg (i.v.) on day eight) for eight
days. However, the patient developed progressive consciousness
disturbance and shortness of breath following chemotherapy. The
serum levels of calcium and parathyroid hormone-related protein
were 18.9 mg/dl and 3.3 pmol/l, respectively, and PET revealed no
bony metastasis. Hypercalcemia occurred as a paraneoplastic
syndrome of pulmonary SC. The patient was treated with hydration,
urgent hemodialysis, i.v calcitonin and bisphosphonates. Due to the
weak condition of the patient, anticancer treatment was
discontinued. However, dyspnea developed and the patient developed
pneumonia four days after the first course of chemotherapy. The
patient’s family refused further treatment and intervention due to
the poor prognosis. The patient succumbed to healthcare-acquired
pneumonia in May 2012 with severe sepsis due to a Pneumocystis
jiroveci infection.
Discussion
The present report describes a case of pulmonary PC
complicated by a soft tissue mass in the right posterior knee with
progressive post-popliteal soreness and stiffness. Pulmonary PCs
are rare, accounting for 0.3% of all invasive lung malignancies,
and they frequently present as large tumors with a mean size of 5–8
cm (range, 1–28 cm) (1,2). However, in the present case, the
patient presented with a rare clinical profile of multiple nodules
in the lungs and metastases to the right para-aortic and popliteal
regions, rather than a single solid mass in the lung. On the basis
of fluid distention of the gastrocnemio-semimembranosus bursa, the
unilateral popliteal mass without redness, local heat or trauma
history was first thought to be a Baker cyst, also termed a
popliteal cyst. However, the possibility of a malignant neoplasm
should not be ruled out despite an MRI showing a single large
lobulated cystic mass that is considered to be benign. The present
case highlights the importance of a correct diagnosis.
Pretherapeutic examinations, such as chest radiography, abdominal
sonography or computed tomography, should be the basis for the
diagnosis of a mass lesion in an unusual or usual site, as observed
in the present case of a popliteal mass lesion.
Pathologically, the majority of these tumors can be
classified using light microscopy alone. The diagnosis of these
tumors requires a resected specimen, largely owing to the
histological heterogeneity and pleomorphism of the tumor. Small
biopsy specimens with adequate cytological material presented with
loose clusters of poorly differentiated epithelial cells, giant
cells, malignant spindle cells and a necrotic background with
neutrophils and lymphocytes, which are highly indicative of PC
(6). The spindle cells and giant
cells of PC usually stain with epithelial markers such as
pancytokeratin (i.e. AE1/AE3), CAM 5.2, CK18 and EMA; however, in a
small percentage of cases, the staining results may be negative. In
the present case report, immunohistochemistry showed that the mass
was positive for Ki67, p53, p63 and vimentin (15). The morphological and
immunohistochemical features were compatible with those of
metastatic SC.
Systemic chemotherapy with a single course of
paclitaxel and cisplatin was unsuccessful. The patient developed a
paraneoplastic syndrome consisting of hypercalcemia, and eventually
acquired pneumonia. A previous case report indicated that pulmonary
PC responds well to a combination of gemcitabine and docetaxel
(7); however, other studies support
the view that pulmonary PC responds poorly to chemotherapy and
targeted therapy (8,11–14).
To date, no standard chemotherapy regimen for pulmonary PC has been
established, and our case indicates that pulmonary PC responds
poorly to combination chemotherapy with paclitaxel and cisplatin.
In our case, hypercalcemia associated with pulmonary PC showed
aggressive disease progression and a poor prognosis. The addition
of combination therapies (i.v. calcitonin and bisphosphonates) to
anticancer drugs for paraneoplastic hypercalcaemia may be
beneficial for improving patient prognosis.
In conclusion, pulmonary sarcomatoid neoplasms are
rare, and we report here the first case of pulmonary PC with
multiple metastases to the right posterior knee. The present case
indicates that pulmonary PC with paraneoplastic hypercalcemia
responds poorly to combination chemotherapy with paclitaxel and
cisplatin. The addition of combination therapies, such as i.v.
calcitonin and bisphosphonates, to anticancer drugs may be
beneficial in cases of paraneoplastic hypercalcemia, which is
associated with aggressive disease progression and a poor
prognosis. Notably, we emphasize that pretherapeutic examinations
should be the basis for the diagnosis of a mass lesion at either an
unusual or usual site, such as the popliteal mass lesion presented
in this case report.
References
|
1
|
Travis WD: Sarcomatoid neoplasms of the
lung and pleura. Arch Pathol Lab Med. 134:1645–1658.
2010.PubMed/NCBI
|
|
2
|
Mochizuki T, Ishii G, Nagai K, et al:
Pleomorphic carcinoma of the lung: clinicopathologic
characteristics of 70 cases. Am J Surg Pathol. 32:1727–1735. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Blaukovitsch M, Halbwedl I, Kothmaier H,
Gogg-Kammerer M and Popper HH: Sarcomatoid carcinomas of the lung -
are these histogenetically heterogeneous tumors? Virchows Arch.
449:455–461. 2006. View Article : Google Scholar
|
|
4
|
Rossi G, Cavazza A, Sturm N, et al:
Pulmonary carcinomas with pleomorphic, sarcomatoid, or sarcomatous
elements: a clinicopathologic and immunohistochemical study of 75
cases. Am J Surg Pathol. 27:311–324. 2003. View Article : Google Scholar
|
|
5
|
Pelosi G, Sonzogni A, De Pas T, et al:
Review article: pulmonary sarcomatoid carcinomas: a practical
overview. Int J Surg Pathol. 18:103–120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Choi HS, Seol H, Heo IY, et al:
Fine-needle aspiration cytology of pleomorphic carcinomas of the
lung. Korean J Pathol. 46:576–582. 2012. View Article : Google Scholar
|
|
7
|
Ichiyama T, Tanabe T, Agatsuma T, et al: A
case of a pulmonary pleomorphic carcinoma with fever which
responded well to chemotherapy. Nihon Kokyuki Gakkai Zasshi.
48:214–218. 2010.(In Japanese).
|
|
8
|
Ushiki A, Koizumi T, Kobayashi N, et al:
Genetic heterogeneity of EGFR mutation in pleomorphic carcinoma of
the lung: response to gefitinib and clinical outcome. Jpn J Clin
Oncol. 39:267–270. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nakazawa T, Hirono Y, Koneri K, et al: A
case of stomach metastasis of pleomorphic carcinoma of the lung
with hypercalcemia. Nihon Shokakibyo Gakkai Zasshi. 109:1204–1212.
2012.(In Japanese).
|
|
10
|
Martin LW, Correa AM, Ordonez NG, et al:
Sarcomatoid carcinoma of the lung: a predictor of poor prognosis.
Ann Thorac Surg. 84:973–980. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Matsubara Y, Tateishi M, Okuyama T, et al:
The operated case of 89 year-old patient with pleomorphic carcinoma
of the lung. Fukuoka Igaku Zasshi. 103:182–185. 2012.(In
Japanese).
|
|
12
|
Avila Martínez RJ, Marrón Fernández C,
Hermoso Alarza F, et al: Primary pulmonary sarcomatoid carcinomas.
Arch Bronconeumol. 24:pii: S0300–2896(12)00335–3. 2013.(In English,
Spanish).
|
|
13
|
Wakizaka K, Otani Y, Aiyama T, et al:
Pulmonary pleomorphic carcinoma with rapid growth causing death in
a short period after surgery; report of a case. Kyobu Geka.
65:1184–1187. 2012.(In Japanese).
|
|
14
|
Vieira T, Duruisseaux M, Ruppert AM, et
al: Pulmonary sarcomatoid carcinoma. Bull Cancer. 99:995–1001.
2012.
|
|
15
|
Pelosi G, Melotti F, Cavazza A, et al: A
modified vimentin histological score helps recognize pulmonary
sarcomatoid carcinoma in small biopsy samples. Anticancer Res.
32:1463–1473. 2012.
|