Introduction
A raised prostate specific antigen (PSA) level is
the first sign of prostate cancer in the majority of asymptomatic
patients, although subjects with high-risk disease may exhibit PSA
levels within the normal range (1).
These patients are only diagnosed early in cases with unexpected
evidence of urinary symptoms and/or prostate nodules that are
identified during a digital rectal examination. More frequently,
patients with PSA levels within the normal range are diagnosed with
prostate cancer later, in association with the presence of symptoms
due to tumor spread or metastatic disease. Of these patients, few
are subsequently clinically evaluated and treated using definitive
treatments with curative intent (2). The clinical evaluation for tumor
staging includes pelvic nuclear magnetic resonance (NMR), computed
tomography (CT) and total bone scans, while choline positron
emission tomography (PET) is currently used to investigate the
presence of distant metastases or locally advanced tumor spread.
PET [11C]- and [18F]-choline derivatives have
also been successfully used to monitor patients following surgery,
radiotherapy or hormonal treatments. However, false negative
results have been previously reported. The use of choline for
prostate cancer imaging is based on increased phosphorylcholine
levels and elevated phosphatidylcholine turnover in prostate cancer
cells. choline PET has also been previously evaluated in the early
detection of prostate cancer with conflicting results (3–7). By
contrast, PET and PET-CT with fluorodeoxyglucose (FDG) have
demonstrated a limited sensitivity for prostate cancer detection,
but may easily identify a positive result in undifferentiated,
biologically aggressive and metastatic tumors (8). A recent study by Minamimoto et
al(9) investigated the FDG-PET
screening cancer program using 155,456 subjects and identified a
37.0% PET sensitivity in patients with prostate cancer. To date, a
low importance has been assigned to FDG-PET to investigate the
potential identification of patients with aggressive primary
prostate cancer among subjects with low PSA levels. The present
study reports a case series of six patients with normal PSA serum
levels, who underwent FDG-PET due to other causes. The PET results
were positive at the prostate and the patients were subsequently
diagnosed with high-risk prostate cancer. Written informed consent
was obtained from the patients.
Case reports
Case 1
A 61-year-old patient presented with no significant
urinary symptoms, a total PSA serum level of 3.9 ng/ml and a body
mass index (BMI) of 24.4. The patient was suspected of having
multiple myeloma due to the presence of osteolytic areas on the
skull, which were observed on an X-ray following a consultation
with the otorhinolaryngologist due to a chronic nasal obstruction,
asthenia, slight anaemia and a headache. FDG-PET was suggested by
the hematologist and was identified to be positive at the prostate
and oropharynx. The digital rectal examination (DRE) was negative
for nodules and prostate cancer was not suspected. An 18-core
prostate biopsy was then performed resulting in five bilateral
positive cores and a pathological diagnosis of prostate
adenocarcinoma (Gleason score 6; 3+3). The total bone scan was
negative. The patient underwent a retropubic radical prostatectomy
with pelvic limphadenectomy. The pathological evaluation
demonstrated pT2cN0 prostate adenocarcinoma involving the two lobes
and the right apex (Gleason score 8; 5+3), with negative margins.
The total PSA levels were 0.05 and 0.12 ng/ml at the three- and
six-month follow-up appointments, respectively. Adjuvant
conformational radiotherapy was then administered with a cumulative
dose of 70 Gy and completed just a month later. At the six-month
follow-up appointment, the PSA value had increased to 0.8
ng/ml and the PET-FDG result was positive at the prostatic fossa,
which was the single remaining location of the disease.
Case 2
A 72-year-old patient presented with no significant
urinary symptoms and a BMI of 21.8. The total PSA serum level at
the time of diagnosis was 3.27 ng/ml. Asthenia and back pain were
investigated by spinal plain X-rays. The total bone scan was
negative. An early suspicion of multiple myeloma indicated the
requirement for FDG-PET, which was positive at the prostate gland.
The DRE was negative for nodules or prostate indurations. The
18-core prostate biopsy was positive for prostate adenocarcinoma in
two cores on the left lobe (Gleason score 6; 3+3). The patient was
administered radiotherapy with a cumulative dose of 70 Gy. The
total PSA level was 0.3 ng/ml following six months of the
treatment. The final FDG-PET result was negative.
Case 3
A 70-year-old patient presented with no urinary
clinical symptoms and a BMI of 23.6. The total PSA level was 2.7
ng/ml. The patient had already been diagnosed with myasthenia
gravis, muscle weakness and fatigue. FDG-PET was performed to
investigate the possible presence of a thymoma, but instead
revealed a positive result at the prostate gland. The 18-core
prostate biopsy revealed the presence of a prostatic adenocarcinoma
on the left lobe (Gleason score 7; 4+3). The patient underwent a
radical retropubic prostatectomy and the pathological stage was
classified as pT2cN0. The PSA level was 0.02 at 6 months
post-surgery. The final FDG-PET result was negative.
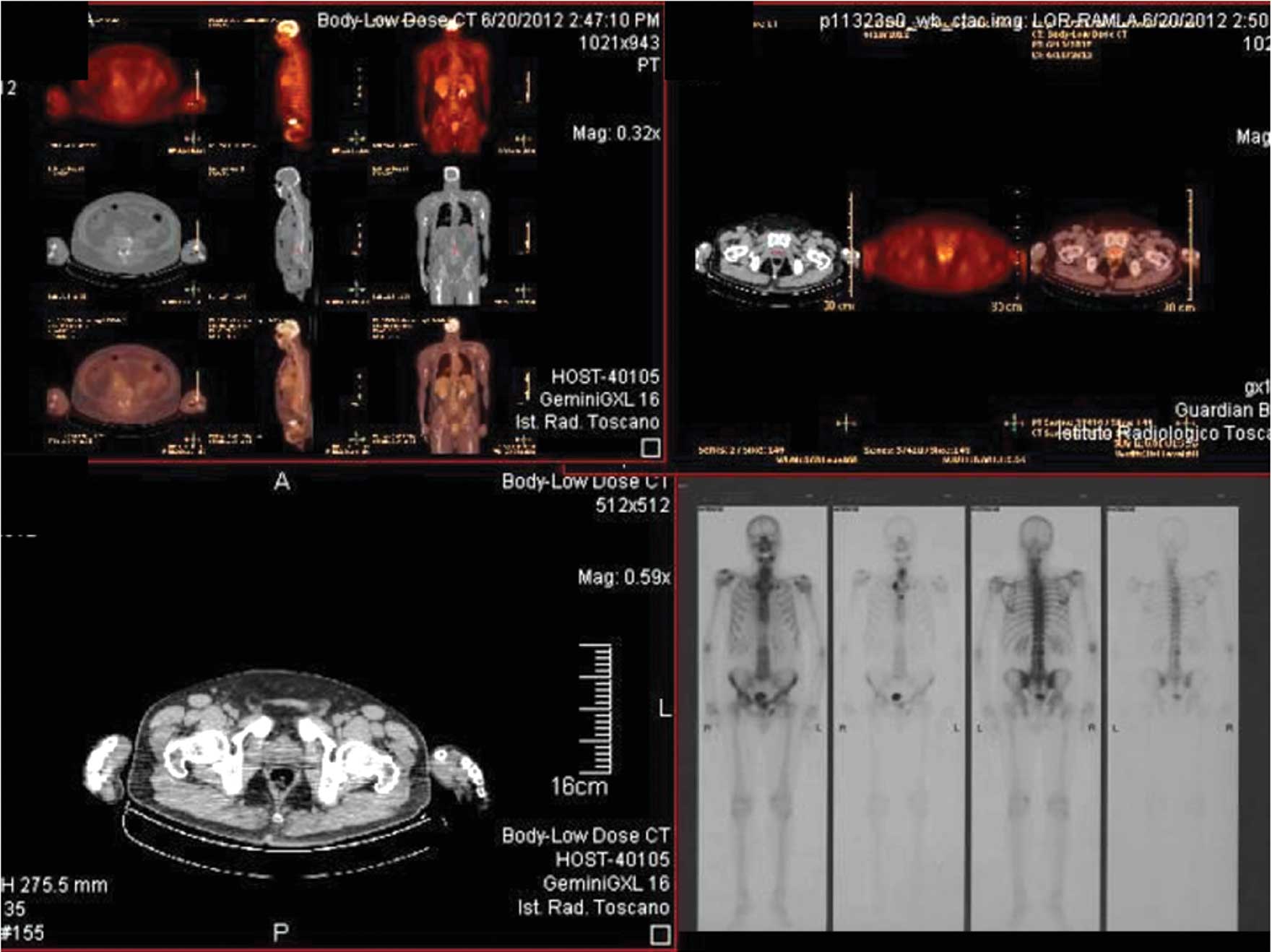
Case 4
A 52-year-old patient with a BMI of 30.2 presented
with asthenia and back pain, which were later confirmed as the
first non-specific signs of prostate cancer. FDG-PET was performed
due to a suspected case of multiple myeloma, and a positive signal
was revealed at the prostate (Fig.
1). The PSA level was 2.0 ng/ml and the DRE was negative. An
18-core random prostate biopsy was positive for prostate cancer on
the left lobe (Gleason score 6; 3+3). The bone scan and NMR
transrectal coil imaging were negative. The patient underwent a
retropubic radical prostatectomy. The pathological stage was
classified as pT2aN0 (Gleason score 6; 3+3). No clinical signs or
symptoms of disease were present at one month post-surgery.
Case 5
A 64-year-old patient with a BMI of 28.5 presented
with no pain or urinary symptoms. A hyperplastic and painful
cervical lymph node was investigated using FDG-PET, which revealed
a positive signal at the prostate. The PSA level was 2.18 ng/ml and
the DRE was negative. The patient was diagnosed with prostate
cancer following a 12-core prostate biopsy with cancer diffusion to
the two lobes (Gleason score 7; 4+3) and subsequently underwent a
retropubic radical prostatectomy. The pathological stage was
classified as pT2cN0 (Gleason score 8; 4+4). The patient was
observed to have no evidence of disease at a follow-up appointment,
7 months after surgery (PSA level, <0.01 ng/ml). The final
FDG-PET result was negative.
Case 6
A 68-year-old patient with a BMI of 29.1 presented
with no pain or urinary symptoms. The patient had already been
diagnosed with and treated for systemic non-Hodgkin lymphoma and
now periodically underwent clinical and imaging monitoring. The
FDG-PET identified a positive signal at the prostate, with a PSA
level of 1.56 ng/ml and a negative DRE. Prostate cancer was
diagnosed following a 12-core prostate biopsy with bilateral cancer
diffusion (Gleason score 8; 4+4). The patient underwent a
retropubic radical prostatectomy. The pathological stage was
classified as pT3bN0 (Gleason total score 8; 4+4). The PSA level
was <0.01 after 12 months and the final FDG-PET was negative. No
apparent recurrences were observed for non-Hodgkin lymphoma or
prostate cancer.
Overall results
The pre-biopsy PSA levels of the six cases ranged
from 1.56 to 3.9 ng/ml, with a median value of 2.4 ng/ml. The
pathological evaluation demonstrated high-risk prostate cancer
diagnoses in four of the five cases that underwent radical
prostatectomies, while the one patient who was administered
external beam radiotherapy was diagnosed with low-risk prostate
cancer on the basis of the pathological analysis of the prostate
biopsy. The disease staging was performed by NMR phased array and
total bone scanning in all the patients without significant results
in terms of primary tumor or tumor metastases identification.
Clinical organ-confined prostate cancer was identified in all the
cases on the basis of positive prostate core biopsies and positive
FDG-PET signaling. Five patients, all <70 years old, underwent
radical prostatectomies and one patient, who was 72 years old, was
administered radiotherapy. The pathological investigations
evidenced high-risk prostate cancer in four of the five patients
that were treated by surgery (Gleason scores 7–10), one of whom had
previously been diagnosed with low-risk disease. Four patients were
observed to have organ-confined diseases (three pT2c and one pT2a;
Gleason scores 5+3, 4+3, 3+3 and 4+4, respectively) and one patient
exhibited extra capsular disease (pT3b Gleason score 4+4). All the
cases that were treated by surgery had negative surgical margins.
The post-operative PSA levels remained at <0.02 ng/ml in three
cases at a mean eight-month follow-up time, but increased to 0.12
ng/ml following five months in the last case. The patient who was
>70 years old and was previously treated with radiotherapy
(Gleason score 3+3) at prostate biopsy, revealed a PSA level of 0.3
ng/ml following three months with stable disease (Table I). All the patients displayed
negative FDG-PET signaling at the six months (range, 1–12 months)
follow-up.
 | Table IPatient characteristics and medical
histories. |
Table I
Patient characteristics and medical
histories.
| Case | Age, years | BMI | Cause of clinical
suspicion FDG-PET | Site of positive
FDG-PET signaling | PSA, ng/ml | Biopsy | Clinical stage | Treatment | Pathological
stage | Pathological Gleason
score | Follow-up,
months | Final status |
|---|
| 1 | 61 | 24.47 | Suspicion of
myeloma | Prostate and
oropharynx | 3.90 | 3+3 bilateral | T0 | RP | pT2cN0 | 5+3 | 6 | Increased PSA,
negative FDG-PET |
| 2 | 72 | 21.80 | Suspicion of
myeloma | Prostate | 3.27 | 3+3 left lobe | T0 | RT | ND | | 6 | PSA<0.02, negative
FDG-PET |
| 3 | 70 | 23.66 | Myasthenia | Prostate | 2.70 | 4+3 left lobe | T0 | RP | pT2cN0 | 4+3 | 6 | PSA<0.01, negative
FDG-PET |
| 4 | 52 | 30.20 | Suspicion of
myeloma | Prostate | 2.00 | 3+3 left lobe | T0 | RP | pT2aN0 | 3+3 | 1 | Not yet
evaluated |
| 5 | 64 | 28.50 | Latero cervical lymph
node | Prostate | 2.18 | 4+3 bilateral | T0 | RP | pT2cNo | 4+4 | 7 | PSA<0.1, negative
FDG-PET |
| 6 | 68 | 29.10 | Non-Hodgkin
lymphoma | Prostate | 1.56 | 4+4 bilateral | T0 | RP | pT3bN0 | 4+4 | 12 | PSA<0.02, negative
FDG-PET |
Discussion
This is the first series of patients with apparently
normal PSA levels, positive FDG-PET signaling and subsequent
diagnoses of high-risk prostate cancer. Patients with PSA levels
within the normal range of 0–4 ng/ml are usually only diagnosed
with prostate cancer in cases of concomitant urinary and/or pain
symptoms that are associated with the local extent and metastatic
diffusion of the disease. Data obtained from the prostate cancer
prevention trial (PCPT) indicates that up to 15% of males with a
normal screening test (PSA level <4 ng/ml and negative digital
rectal examination) have biopsy-detectable prostate cancer
(10). By contrast, PSA screening
is associated with substantial unfavorable effects. In the European
Randomized Study of Screening for Prostate Cancer (ERSPC) screening
group, the cumulative incidence was 7.4% compared with 5.1% in the
control group, and over-diagnosed cancers were frequently treated
with higher risks of adverse events (11,12).
Due to these reasons, PSA level determination may be considered as
an independent factor in the early diagnosis of prostate cancer.
choline PET and PET/computed tomography (CT) have been scarcely
used in the primary diagnosis of prostate cancer and with
conflicting results, but they are currently used for the disease
staging and monitoring of patients following treatment (8). Testa et al(13) compared the diagnostic performance of
magnetic resonance imaging (MRI), 3-dimensional magnetic resonance
spectroscopy (MRS), combined MRI and MRS and
[11C]-choline PET/CT for imaging primary prostate
cancer. The sensitivity of choline PET/CT was observed to be lower
(55%) in comparison with MRS alone (81%) or MRS in combination with
NMR (88%). By contrast, Yamaguchi et al(14) identified a higher sensitivity of
choline PET (100%) compared with MRI alone (60%) or in combination
with MRS (65%). The mean PSA values were 13.91 (range, 2.5–70) and
23.4 (range, 4.3–93.9) in the two series, respectively. Two
patients with prostate cancer and normal PSA serum levels of 2.5
and 3.1 ng/ml at diagnosis, respectively, were included in the
series by Testa et al(13),
but advanced pathological stage (pT3a) and high-risk disease
(Gleason score 4+3) was identified in one patient without specific
information with regard to the sensitivity to choline PET imaging.
Although a relatively low FDG uptake has been previously attributed
to prostate cancer due to its slow metabolic rate and lower
expression of glucose transport proteins, Hwang et
al(15) analyzed FDG-PET/CT
images from 12,037 subjects showing abnormal hypermetabolism in the
prostate. A total of 120 patients were observed to exhibit abnormal
FDG-PET/CT signaling, but 38 of these were subsequently
investigated by prostate biopsy as a consequence of an abnormal
total PSA serum level determination and/or the clinical suspicion
of cancer at DRE (15). Of the 38
patients, 23 were confirmed to have prostate cancer with a median
PSA level of 49.7 ng/ml. The cumulative results indicated that
hypermetabolism in the prostate was incidentally detected in 1.5%
of the patients, but only 65.2% underwent further clinical
evaluation by DRE and/or serum PSA level determination (15). No data on patients with apparently
normal PSA levels were thus collected (15). All the cases that were included in
the present series had no urinary symptoms or clinical suspicions
of prostate cancer and had normal PSA levels. Thus, the clinical
diagnosis of prostate cancer was incidental. In the course of an
FDG-PET cancer screening program in Japan based on a four-year
nationwide survey conducted on 155,456 asymptomatic subjects,
Minamimoto et al(9)
identified positive findings indicating possible cancer in 16,955
cases (10.9%). The overall number of cancers that were actually
detected was 1,912, but prostate cancer was identified in 165
patients, with a FDG-PET sensitivity of 37.0% (9). It may be concluded that approximately
one-third of subjects with prostate cancer with positive FDG-PET
findings may also have altered PSA levels. Decreased PSA levels in
prostate cancer patients may have confounding factors, including
the concomitant use of medical therapies, such as hormones, statins
and non-steroidal anti-inflammatory drugs, and/or a higher BMI.
Wright et al(16) observed
that an increased BMI (<25, 25–29 and >30) was proportional
to a decline in the geometric PSA values (1.18, 1.13 and 0.94,
respectively) and hat obese males had lower age-adjusted PSA levels
compared with males of a normal weight. The patients that were
enrolled in the study had no previous medical treatments, none were
obese and the BMI was <25, with the exception of one case. Thus,
the PSA values may be considered to have been homogeneously
measured. Helfand et al(17)
identified that a panel of 17 risk alleles and a family history of
prostate cancer is associated with an increased risk of the
disease, even amongst patients with normal PSA levels and DRE.
These data were not confirmed by the results that were obtained in
the present series, as none of the patients that were investigated
had a family history of prostate cancer. A recent study by
Koochekpour et al(18)
demonstrated a possible characterization of prostate cancer tumor
cells in association with their metabolism. The metabolism of
aggressive cancers may be altered by the presence of glutamate
receptor 1 (GRM1) antagonists with subsequent development of the
Warburg effect in the case of tumor-related induced hypoxia.
Koochekpour et al(18)
observed significantly higher serum glutamate levels in tumors with
a Gleason score of >8 than in those with a Gleason score of
<7 among African-Americans compared with Caucasian Americans.
Glutamate metabolism alterations may represent a justification of
possible positive FDG-PET signaling in patients with aggressive
prostate cancer and a biomarker to be used in the future to
characterize potentially evolutive or indolent prostate cancers.
The main limitation of the present study consists of the
non-consecutive patient selection that was due to the incidental
diagnosis of prostate cancer in response to apparently normal PSA
values. In all these cases, the total PSA measurement was not
functional as a prognostic variable for monitoring the patients,
while FDG-PET was imperative to determine the evidence of possible
metastatic sites.
In conclusion, FDG-PET has been used to define the
clinical suspicion for prostate cancer in a small series of
asymptomatic patients with normal PSA levels. This phenomenon may
be justified with a strong correlation between the metabolism of
tumor cells and mitochondrial activity due to the Warburg effect.
FDG-PET may be considered for future studies in order to
characterize the aggressive behavior of primary prostate cancers in
patients with normal PSA levels.
References
|
1
|
Artibani W: Landmarks in prostate cancer
diagnosis: the biomarkers. BJU Int. 110(Suppl 1): S8–S13. 2012.
View Article : Google Scholar
|
|
2
|
Wallner LP, Frencher SK, Hsu JW, et al:
Changes in serum prostate-specific antigen levels and the
identification of prostate cancer in a large managed care
population. BJU Int. 111:1245–1252. 2013. View Article : Google Scholar
|
|
3
|
Ackerstaff E, Glunde K and Bhujwalla ZM:
Choline phospholipid metabolism: a target in cancer cells? J Cell
Biochem. 90:525–533. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kwee SA, Coel MN, Lim J and Ko JP:
Prostate cancer localization with 18fluorine fluorocholine positron
emission tomography. J Urol. 173:252–255. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reske SN, Blumstein NM, Neumaier B, et al:
Imaging prostate cancer with 11C-choline PET/CT. J Nucl Med.
47:1249–1254. 2006.PubMed/NCBI
|
|
6
|
Martorana G, Schiavina R, Corti B, et al:
11C-choline positron emission tomography/computerized tomography
for tumor localization of primary prostate cancer in comparison
with 12-core biopsy. J Urol. 176:954–960. 2006. View Article : Google Scholar
|
|
7
|
Scher B, Seitz M, Albinger W, et al: Value
of 11C-choline PET and PET/CT in patients with suspected prostate
cancer. Eur J Nucl Med Mol Imaging. 34:45–53. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Swartzenböck S, Souvatzoglou M and Krause
BJ: Choline PET and PET/CT in primary diagnosis and staging of
prostate cancer. Theranostics. 2:318–330. 2012.PubMed/NCBI
|
|
9
|
Minamimoto R, Senda M, Jinnouchi S, et al:
The current status of an FDG-PET cancer screening program in Japan,
based on a 4-year (2006–2009) nationwide survey. Ann Nucl Med.
27:46–57. 2013.PubMed/NCBI
|
|
10
|
Thompson IM, Tangen C and Goodman P: The
prostate cancer prevention trial: design, status and promise. World
J Urol. 21:28–30. 2003.PubMed/NCBI
|
|
11
|
Schröder FH, Hugosson J, Roobol MJ, et al;
ERSPC Investigators. Screening and prostate-cancer mortality in a
randomized European study. N Engl J Med. 360:1320–1328.
2009.PubMed/NCBI
|
|
12
|
Heijndijk EA, Wever EM, Auvinen A, et al:
Quality of life effects of prostate-specific antigen screening. N
Engl J Med. 367:595–605. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Testa C, Schiavina R, Lodi R, et al:
Prostate cancer: sextant localization with MR imaging, MR
spectroscopy, and 11C-choline PET/CT. Radiology. 244:797–806. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yamaguchi T, Lee J, Uemura H, et al:
Prostate cancer: a comparative study of 11C-choline PET and MR
imaging combined with proton MR spectroscopy. Eur J Nucl Med Mol
Imaging. 32:742–748. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hwang I, Chong A, Jung SI, et al: Is
further evaluation needed for incidental focal uptake in the
prostate in 18-fluoro-2-deoxyglucose positron emission
tomography-computed tomography images? Ann Nucl Med. 27:140–145.
2013. View Article : Google Scholar
|
|
16
|
Wright JL, Lin DW and Stanford JL: The
effect of demographic and clinical factors on the relationship
between BMI and PSA levels. Prostate. 71:1631–1637. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Helfand BT, Kan D, Modi P and Catalona WJ:
Prostate cancer risk alleles significantly improve disease
detection and are associated with aggressive features in patients
with a ‘normal’ prostate specific antigen and digital rectal
examination. Prostate. 71:394–402. 2011.PubMed/NCBI
|
|
18
|
Koochekpour S, Majumdar S, Azabdaftari G,
et al: Serum glutamate levels correlate with Gleason score and
glutamate blockade decreases proliferation, migration, and invasion
and induces apoptosis in prostate cancer cells. Clin Cancer Res.
18:5888–5901. 2012. View Article : Google Scholar
|