Introduction
Salivary gland tumors form in the tissues of
salivary glands. The incidence of these tumors varies worldwide and
is between 0.4–13.5/100,000 individuals annually, with a malignant
tumor rate of ~0.4–2.6/100,000 (1).
In Mainland China, salivary gland tumors account for 2.3% of all
human tumors and ~20% of oral and maxillofacial tumors. Among these
tumors, parotid gland tumors are the most common of salivary gland
tumors, followed by submandibular gland minor salivary and
sublingual gland tumors. With changes in lifestyle and an
increasingly elderly population, the incidence of parotid gland
tumors is also increasing. However, the etiology of parotid gland
tumors remains to be defined, although, previous studies indicate
that there are various risk factors (such as tobacco smoking,
alcohol consumption and a previous history of radiotherapy)
associated with the development of parotid gland tumors. Previous
studies have indicated that mobile phone usage may increase the
incidence of parotid gland tumors (2). However, the development of parotid
gland tumors, similar to the majority of other tumors, is
associated with multiple risk factors. Alteration of various tumor
suppressor genes and activation of oncogenes are important in
parotid gland tumor development and progression (3–7).
However, the underlying molecular mechanisms responsible for their
alteration and activation require further investigation. Therefore,
the present study focused on the role of human papillomavirus (HPV)
infection in the development of parotid gland tumors.
Notably, HPV has previously been shown to induce
human types of cancer and it is capable of infecting human
keratinocytes and mucous membranes. HPV is a small (45–55-nm in
diameter), non-enveloped double-stranded and closed circular DNA
tumor virus. HPV infects epithelial tissues through microabrasions
or other epithelial trauma by delivery of the viral genome to the
host cell nucleus. HPV exists in the following three forms in
infected cells: i) Integrated, DNA virus in the host cell
chromosome; ii) episomal, DNA virus that is free from the cell
chromosome; and iii) episomal and integrated. While the majority of
the known types of HPV cause no symptoms in almost all patients,
specific types of HPV may cause warts and cancer in humans. For
example, HPV E6 and E7 proteins inactivate two tumor suppressor
proteins, p53 and pRb. The correlation between HPV and head and
neck cancer has been previously well documented in the literature
(8–10). Several studies have demonstrated
that 50–90% of squamous cell carcinoma of the oropharynx, tongue
and tonsils, are associated with HPV infection (11–13).
The majority of previous studies have only focused on the role of
HPV infection in squamous cell tumors (14,15),
however, specific studies have shown that HPV infection may also
play a role in glandular epithelial tumors (16,17).
Thus, the current study utilized flow-through hybridization and
gene chip technology, an analytical technique with high sensitivity
and specificity. Specifically, 37 common types of HPV were analyzed
in 59 cases of paraffin-embedded specimens of parotid gland tumor
tissues to identify the correlation between HPV subtype infection
and the development of parotid gland tumors.
Materials and methods
Study population
In total, 59 cases of parotid gland tumor tissue
samples were obtained from the Department of Pathology, Shanghai
Pudong New Area Gongli Hospital (Shanghai, China) between 2004 and
2011. All patients were diagnosed with parotid gland tumors
histopathologically and included 35 males and 24 females with an
age range between 23 and 89 years (56.7±16.2 years old). Among the
59 cases, 52 were benign tumors (36 mixed tumor, 3 adenoma, 12
gland lymphoma and 1 myoepithelioma) and 7 were malignant tumors (3
adenocarcinoma, 1 adenoid cystic carcinoma, 1 mucoepidermoid
carcinoma and 2 other cases). All patients had not previously been
treated with any radiotherapy or chemotherapy prior to surgery.
Tumor tissue samples were fixed in 10% formalin and embedded in
paraffin.
In addition, normal oral mucosa tissues from 20
normal healthy volunteers were also obtained from the hospital and
fixed in formalin and embedded in paraffin. Of the healthy
volunteers, 50% were male and female, respectively, with an age
range between 24 and 62 years (37.9±15.6 years). The study was
approved by the hospital review board and each patient and
volunteer signed an informed consent form.
DNA extraction, polymerase chain reaction
(PCR) amplification and flow-through hybridization
Genomic DNA was first extracted from each tissue
specimen. In brief, paraffin-embedded tissue samples from all 59
cases of parotid gland tumors and 20 healthy volunteers were
randomly arranged and three consecutive tissue sections (10-μm
thick) were subjected to DNA extraction using a DNA extraction kit
(Chaozhou Hybribio Biochemical Co., Ltd., Chaozhou, China)
according to the manufacturer’s instructions. Next, the DNA samples
were amplified by PCR using a PCR reagent kit (Chaozhou Hybribio
Biochemical Co., Ltd.). The two consensus primers, MY09 and MY11,
that amplify the most conserved HPV L1 region and have been widely
used in previous clinical and epidemiological studies, were used as
controls: MY09, 5′-CGTCCMARRGGAWACTGATG-3′; and MY11,
5′-GCMCAGGWCATAAYAATGC-3′. Specifically, PCR amplification
contained 1 μl DNA sample in 25 μl PCR mixtures. The PCR conditions
were as follows: DNA predenaturation at 95°C for 9 min, followed by
40 cycles of 95°C for 20 sec, 55°C for 30 sec, 72°C for 30 sec and
a final extension at 72°C for 5 min. Next, the PCR products were
subjected to DNA flow-through hybridization. Briefly, 20 μl PCR
product was added to a low-density cDNA microarray containing one
of the following 37 HPV type-specific oligonucleotide probes: HPV
6, 11, 16, 18, 26, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52,
53, 54, 55, 56, 57, 58, 59, 61, 66, 67, 68, 69, 70, 71, 72, 73, 82,
83, 84 and CP8304. The manufacturer’s instructions for the HPV
GenoArray test kit (Qiagen, Hilden, Germany) were followed for
flow-through hybridization and biotin enzyme-color reaction for ≤1
h. Distilled water and HPV 18 were used as the negative and
positive controls, respectively.
Data evaluation
Biotinylated DNA was used as biotin-control points
to check the reliability and producibility of the assays utilized.
In addition, internal control (IC) spots were used as quality
control spots for PCR, thermal denaturation and hybridization
processes. If no inhibiting factors were identified in the PCR
system, IC spots appear; if one of the two control spots does not
appear, the experiments were repeated for that particular specimen.
Next, all experimental results were obtained by visual inspection
of assayed data. The positive results appeared as clear blue-purple
dots. The HPV-positive points were evaluated by matching them to
the distribution map of HPV subtypes on the film.
Statistical analysis
All data were summarized as positive or negative for
each case and then statistically analyzed by SPSS 11.5 software
(SPSS, Inc., Chicago, IL, USA) and χ2 test. P<0.05
was considered to indicated a statistically significant
difference.
Results
Detection of HPV DNA in parotid gland
tumor and normal control tissues
PCR amplification and flow-through hybridization
detection of 37 subtypes of HPV were performed in tissue specimens
of parotid gland tumors and normal oral mucosa. The results are
shown in Tables I and II. Specifically, the total HPV-positive
rate in the 59 tissue specimens of parotid gland tumors was 57.6%
(34/59), including 59.6% (31/52) in benign parotid gland tumors and
42.9% (3/7) in malignant parotid gland tumors. HPV infection in
normal oral mucosa tissue samples was negative. A statistically
significant difference was identified in HPV infection between the
parotid gland tumor specimens and normal control group
(χ2=20.234; P<0.05), whereas, the HPV-positive rates
between benign and malignant parotid gland tumors were not
significantly different (χ2=0.189; P>0.05). In the 34
cases of HPV-positive samples, no statistically significant
difference was identified in gender distribution
(χ2=0.008; P=0.928).
 | Table IExpression of HPV in parotid gland
tumor and normal control tissues. |
Table I
Expression of HPV in parotid gland
tumor and normal control tissues.
| | HPV expression | |
|---|
| |
| |
|---|
| Group | n | Positive, n (%) | Negative, n (%) | P-value |
|---|
| Control | 20 | 0 (0.0) | 20 (100.0) | |
| Parotid gland
tumor | 59 | 34 (57.6) | 25 (42.4) | 0.000 |
| Table IIExpression of HPV in benign and
malignant parotid gland tumor tissues. |
Table II
Expression of HPV in benign and
malignant parotid gland tumor tissues.
| | HPV expression | |
|---|
| |
| |
|---|
| Group | n | Positive, n (%) | Negative, n (%) | P-value |
|---|
| Benign tumors | 52 | 31 (59.6) | 21 (40.4) | |
| Malignant tumors | 7 | 3 (42.9) | 4 (57.1) | 0.664 |
Distribution of HPV types in benign and
malignant parotid gland tumor tissues
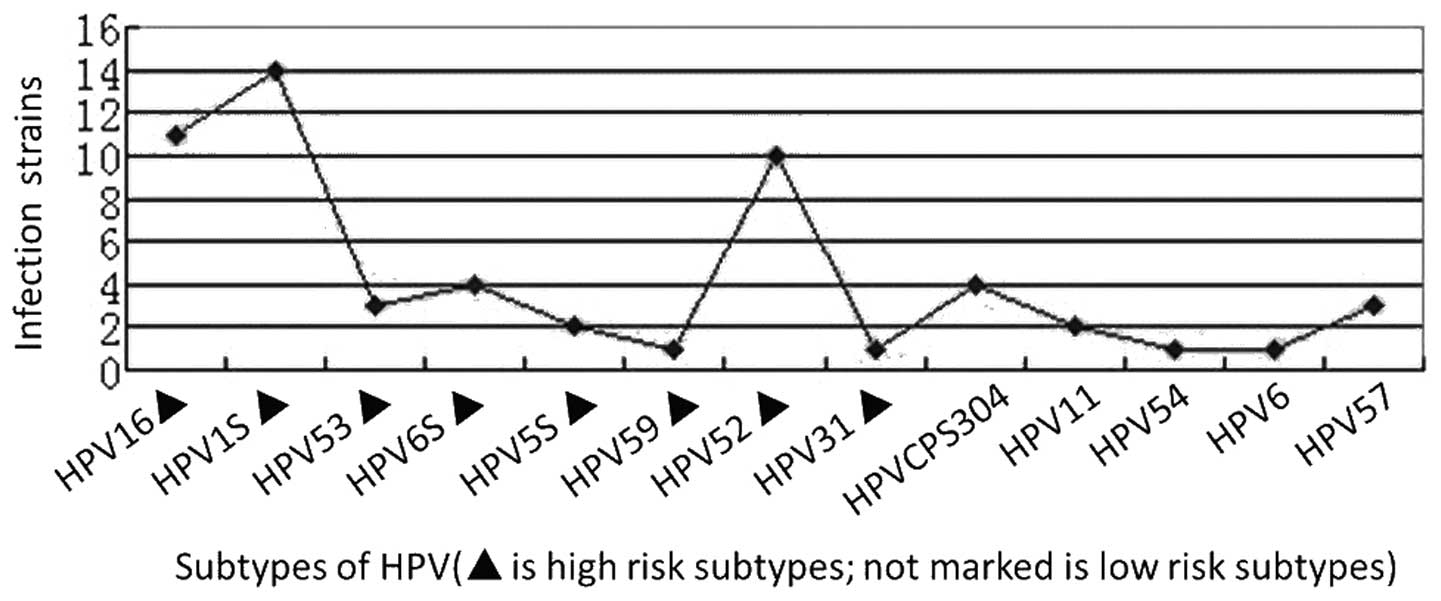
Next, HPV positivity was analyzed in the 34
HPV-positive cases. A total of 57 strains of HPV were identified in
these 34 cases, which included 13 subtypes of HPV. The specific
distribution of HPV subtypes is shown in Fig. 1. In total, 5 low-risk types,
including 11 strains of HPV, represented 19.3% of the total number
of detected strains. The predominant subtypes were HPV CP8304 and
57, accounting for 5% of the total number of detected strains. In
addition, 46 strains of HPV belonged to 8 high-risk types and
accounted for 80.7% of the total number of detected strains. The
predominant subtypes were HPV 16, 18 and 52, representing 19.3,
24.6 and 17.5% of the total number of detected strains,
respectively. The distribution of HPV subtypes in benign and
malignant parotid gland tumors are shown in Tables III and IV, respectively.
| Table IIIDistribution of HPV subtypes in benign
parotid gland tumor tissues. |
Table III
Distribution of HPV subtypes in benign
parotid gland tumor tissues.
| Pathological
classification | n | Low-risk HPV
subtypes | High-risk HPV
subtypes |
|---|
|
|
|---|
| 11 | 54 | 57 | 6 | CP8304 | 53 | 68 | 58 | 52 | 16 | 18 | 31 | 59 |
|---|
| Mixed tumor | 36 | 1 | 1 | 1 | 1 | 3 | 3 | 3 | 1 | 8 | 8 | 8 | 1 | 0 |
| Adenolymphoma | 12 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 2 | 0 | 0 |
| Adenoma | 3 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 |
| Myoepithelioma | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Total | 52 | 2 | 1 | 3 | 1 | 3 | 3 | 3 | 1 | 10 | 9 | 12 | 1 | 1 |
| Table IVDistribution of HPV subtypes in
malignant parotid gland tumor tissues. |
Table IV
Distribution of HPV subtypes in
malignant parotid gland tumor tissues.
| | Low-risk HPV
subtypes | High-risk HPV
subtypes |
|---|
| |
|
|
|---|
| Pathological
classification | n | CP8304 | 68 | 58 | 16 | 18 |
|---|
| Adenocarcinoma | 3 | 0 | 0 | 0 | 1 | 1 |
| Adenoid cystic
carcinoma | 1 | 0 | 0 | 0 | 0 | 0 |
| Mucoepidermoid
carcinoma | 1 | 1 | 0 | 1 | 1 | 0 |
| Others | 2 | 0 | 1 | 0 | 0 | 1 |
| Total | 7 | 1 | 1 | 1 | 2 | 2 |
Single and multiple HPV infections in
parotid gland tumor tissue specimens
It was determined whether single or multiple HPV
infections were present in parotid gland tumor tissue specimens.
The results showed that a single or mixed HPV infection by multiple
types was detected in specific single tissue samples. The infection
rates of single and multiple types were 47.1 (16/34) and 52.9%
(18/34), respectively. In the mixed infection, double infections
were the most common at 77.8% (14/18), triple infections were 16.7%
(3/18) and infections by four types were 5.6% (1/18) (Table V).
| Table VDistribution of HPV infection by
single or multiple subtypes in benign and malignant parotid gland
tumor tissues. |
Table V
Distribution of HPV infection by
single or multiple subtypes in benign and malignant parotid gland
tumor tissues.
| Group | n | Single subtype
infection, n (%) | Mixed infection,
high- and low-risk subtypes, n (%) | Mixed infection,
high-risk subtypes, only, n (%) | Mixed infection,
low-risk subtypes only, n |
|---|
| Benign tumor | 31 | 16 (51.6) | 6 (19.4) | 9 (29.0) | 0 |
| Malignant
tumor | 3 | 0 (0.0) | 1 (33.3) | 2 (66.7) | 0 |
| Total | 34 | 16 (47.1) | 7 (20.6) | 11 (32.3) | 0 |
Discussion
In the current study, the presence of infection by
various HPV genotypes was determined in 59 cases of parotid gland
tumor tissue specimens and compared with 20 cases of normal oral
mucosa specimens using a rapid flow-through hybridization of
nucleic acid molecular gene chip technology. This technique differs
from immunohistochemical staining and PCR due to its high
sensitivity and specificity, accuracy and reliability. The HybriMax
technique was used to rapidly detect 37 HPV genotypes for mixed HPV
infections. The hybridization background was clean and required a
small volume of reagents.
In the present study, 57.6% (34/59) of the parotid
gland tumor tissue specimens were HPV-positive, whereas, the normal
oral mucosa samples were HPV-negative. The results indicated that
HPV infection may promote the development of parotid gland tumors.
Furthermore, HPV infection rates in benign and malignant parotid
gland tumor tissue specimens were 59.6 (31/52) and 42.9% (3/7),
respectively, which were not statistically different. HPV 16, 18
and 52 were the predominant HPV types detected in the parotid gland
tumor tissue samples. Previous studies have shown that HPV
infection rates vary between 0 and 77.8% in parotid gland tumor
tissues (8–10,18–21).
These significant variations are due to differences in geographical
factors, the number of tissue specimens studied and detection
methods of HPV subtypes. Previous studies have also shown that
parotid gland tumors are predominantly infected by HPV 16 and 18
types (22–25), which is consistent with the results
of the current study. The majority of previous studies on HPV
investigated cervical diseases and have shown that HPV infection
rates increase with the degree of cervical lesions aggravated
(26–28). Other studies have shown that
increased HPV-positive rates correlate with increments of nasal
inverted papilloma pathological classifications and clinical stages
(29–31. However, in the current study, no significant differences
were identified in HPV-positive rates between benign and malignant
parotid gland tumors.
Previous results have demonstrated that infection
with mixed or multiple HPV subtypes is associated with the severity
of cervical disease (i.e. with an increase in the severity of
cervical lesions, multiple infections of HPV occurred). However,
subsequent studies have indicated a decline in infections by
multiple HPV types and that cervical squamous cell carcinoma is
infected by a single high-risk HPV type (32). In addition, infection by multiple
HPV types may facilitate the induction of atypical hyperplasia of
nasal inverted papilloma (29). The
current study showed that parotid gland tumors infected with a
single HPV subtype or multiple types were 47.1 and 52.9%,
respectively, indicating that parotid gland tumors are more prone
to infection by multiple HPV types. However, it remains to be
elucidated how HPV infection promotes the development of this type
of tumor.
Parotid glands are localized below and in front of
the external acoustic meatus within the mandibular fossa and the
deep surface of the mandibular ramus. Normally, it is difficult to
obtain patient consent to collect normal parotid gland tissues due
to its anatomical location. The parotid gland is
histoembryologically similar to oral mucosa; thus, in the current
study, oral mucosa was used as a normal control. Previous results
have shown that infection with high-risk HPV types is a risk factor
for oral cancer, the effects of which may surpass that of tobacco
smoking in the development of oral cancer (33). The transmission of HPV may occur
through oral sex and infect the oral throat and tonsils. The
results from a previous meta-analysis (34) of 5,681 patients with head and neck
squamous cell carcinoma showed that HPV infection increased the
risk of developing head and neck squamous cell carcinoma. In view
of the association between the anatomy of the oral cavity and
parotid gland, future studies are likely to investigate the
correlation between HPV infection and development of oral cancer
and parotid gland tumors. HPV-positive oral cancer and parotid
gland tumors are likely to be compared with HPV-negative tissue
samples for tumor types and gene expression.
Results of the present study indicate that HPV
infection is associated with the development of parotid gland
tumors, particularly infection by the high-risk HPV subtypes, HPV
16, 18 and 52. Our study demonstrates the association between HPV
infection and parotid gland tumors by flow-through hybridization
and gene chip.
Acknowledgements
The present study was supported, in part, by a grant
from the Shanghai Pudong New Area Science and Technology
Development Foundation (no. PKJ2012-Y27) and by a grant from the
Shanghai Health Bureau of the Pudong New Area of Outstanding Young
Medical Talents Fund (no. PWRq2010-03).
References
|
1
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: Salivary glands. World Health Classification of
Tumours Pathology and Genetics of Head and Neck Tumours. IARC
Press; Lyon: 2005
|
|
2
|
Lönn S, Ahlbom A, Christensen HC, et al:
Mobile phone use and risk of parotid gland tumor. Am J Epidemiol.
164:637–643. 2006.
|
|
3
|
Schorderet DF and Munier FL: Oncogenes and
anti-oncogenes: the genetics of cancer. Praxis (Bern 1994).
85:1019–1022. 1996.(In French).
|
|
4
|
Yu Chen, Kun Tian, Ning Geng, et al: The
expression of matrix metalloproteinases and their tissue inhibitors
in pleomorphic adenoma. Zhonghua Kou Qiang Yi Xue Za Zhi. 40:58–61.
2005.(In Chinese).
|
|
5
|
Brennan PA, Umar T, Buckley J, et al:
Expression of nitric oxide synthase in pleomorphic adenomas of the
parotid. Br J Oral Maxillofac Surg. 38:338–342. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xiang GL, Zhi SR, Chen W, et al:
Expression and clinical significance of COX-2 and cyclinD1 in PA
and CPA. Zhonghua Kou Qiang Ke Za Zhi. 3:131–134. 2007.(In
Chinese).
|
|
7
|
Wang TL and Song M: Advances on
tumorigenesis of salivary pleomorphic adenomas. Kou Qiang Zuo Mian
Wai Ke Za Zhi She. 6:423–426. 2009.(In Chinese).
|
|
8
|
Ragin CC, Modugno F and Gollin SM: The
epidemiology and risk factors of head and neck cancer: a focus on
human papillomavirus. J Dent Res. 86:104–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fakhry C and Gillison ML: Clinical
implications of human papillomavirus in head and neck cancers. J
Clin Oncol. 24:2606–2611. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hwang HS, Yang HS and Hong MK: Detection
of human papillomavirus (HPV) in sinonasal inverted papillomas
using polymerase chain reaction (PCR). Am J Rhinol. 12:365–366.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jo VY, Mills SE, Stoler MH and Stelow EB:
Papillary squamous cell carcinoma of the head and neck: frequent
association with human papillomavirus infection and invasive
carcinoma. Am J Surg Pathol. 33:1720–1724. 2009. View Article : Google Scholar
|
|
12
|
Auluck A, Hislop G, Bajdik C, Poh C, Zhang
L and Rosin M: Trends in oropharyngeal and oral cavity cancer
incidence of human papillomavirus (HPV)-related and HPV-unrelated
sites in a multicultural population: the British Columbia
experience. Cancer. 116:2635–2644. 2010.
|
|
13
|
Andrews E, Seaman WT and Webster-Cyriaque
J: Oropharyngeal carcinoma in non-smokers and non-drinkers: a role
for HPV. Oral Oncol. 45:486–491. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shi Q, Xiao K, Wei W, et al: Associations
of TP53 mutations, codon 72 polymorphism and human papillomavirus
in head and neck squamous cell carcinoma patients. Oncol Rep.
30:2811–2819. 2013.PubMed/NCBI
|
|
15
|
Morbini P, Dal Bello B, Alberizzi P, et
al: Oral HPV infection and persistence in patients with head and
neck cancer. Oral Surg Oral Med Oral Pathol Oral Radiol.
116:474–484. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhao C, Li Z and Austin RM: Cervical
screening test results associated with 265 histopathologic
diagnoses of cervical glandular neoplasia. Am J Clin Pathol.
140:47–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kasamatsu E, Cubilla AL, Alemany L, et al:
Type-specific human papillomavirus distribution in invasive
cervical carcinomas in Paraguay. A study of 432 cases. J Med Virol.
84:1628–1635. 2012. View Article : Google Scholar
|
|
18
|
Vageli D, Sourvinos S, Ioannou M, et al:
High-risk human papillomavirus (HPV) in parotid lesions. Int J Biol
Markers. 22:239–244. 2007.PubMed/NCBI
|
|
19
|
Chen J, Fan C, We A, et al: Infection of
human papillomavirus and parotid gland tumor. J New Med. 7:149–150.
1997.
|
|
20
|
Liang Z, Fu W and Chu Y: Detection of
human papillomavirus in salivary gland tumors. J Xi’An Med Uni.
3:386–388. 1999.(In Chinese).
|
|
21
|
Song J, Wang J, et al: Study on
relationship between expression of C2erbB22 and PCNA, HPV infection
and salivary gland tumors. J Shanxi Med. 38:702–705. 2009.(In
Chinese).
|
|
22
|
Zhao C, Li Z and Austin RM: Cervical
screening test results associated with 265 histopathologic
diagnoses of cervical glandular neoplasia. Am J Clin Pathol.
140:47–54. 2013. View Article : Google Scholar
|
|
23
|
Xiao W, Liu S, Wang L, Li H, Wu W and Wang
Z: Meta analysis of the relationship between human papilloma virus
and nasal inverted papilloma. Lin Chung Er Bi Yan Hou Tou Jing Wai
Ke Za Zhi. 27:572–576. 2013.(In Chinese).
|
|
24
|
Sun P, Chen XP, Pei F, et al: Relationship
between nasal inverted papilloma and human papillomavirus subtypes.
Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 45:310–313. 2010.(In
Chinese).
|
|
25
|
Lu SS, Zou R and Xu JW: Relationship
between prognosis of nasal inverted papilloma and human
papillomavirus types. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za
Zhi. 40:195–198. 2005.(In Chinese).
|
|
26
|
Sharma C, Khan MA, Mohan T, Shrinet J,
Latha N and Singh N: A synthetic chimeric peptide harboring human
papillomavirus 16 cytotoxic T lymphocyte epitopes shows therapeutic
potential in a murine model of cervical cancer. Immunol Res. Oct
31–2013.(Epub ahead of print).
|
|
27
|
Okadome M, Saito T, Tanaka H, et al:
Potential impact of combined high- and low-risk human
papillomavirus infection on the progression of cervical
intraepithelial neoplasia 2. J Obstet Gynaecol Res. Oct
22–2013.(Epub ahead of print).
|
|
28
|
Mendoza LP, Arbiza J, Paez M, et al:
Distribution of human papillomavirus genotypes in Paraguayan women
according to the severity of the cervical lesion. J Med Virol.
83:1351–1357. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sun P, Zhang Y, Ma R, Chen Q, et al: A
association of lesion scope of nasal inverted papilloma with human
papillomavirus (HPV) subtypes. Chin J Otorhinolaryngol Integrat
Traditional Western Med. 2:125–127. 1322011.(In Chinese).
|
|
30
|
Xiao W, Liu S, Wang L, Li H, Wu W and Wang
Z: Meta analysis of the relationship between human papilloma virus
and nasal inverted papilloma. Lin Chung Er Bi Yan Hou Tou Jing Wai
Ke Za Zhi. 27:572–576. 2013.PubMed/NCBI
|
|
31
|
Zhong Z, Yan A, Jiang F, Wei H and Jiang
X: The study on the relationship between human papillomavirus
infection and pathogenesis of nasal inverted papilloma and its
malignant transformation. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke
Za Zhi. 24:209–211. 2010.
|
|
32
|
Wang H and Qian YL: Human papillomavirus
types and their related diseases. Zhongguo Yi Xue Ke Xue Yuan Xue
Bao. 29:678–684. 2007.(In Chinese).
|
|
33
|
Tachezy R, Klozar J, Rubenstein L, et al:
Demographic and risk factors in patients with head and neck tumors.
J Med Virol. 81:878–887. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dayyani F, Etzel CJ, Liu M, et al:
Inhibition of apoptosis in human papillomavirus (HPV) on cancer
risk and overall survival in head and neck squamous cell carcinomas
(HNSCC). Head Neck Oncol. 2:152010. View Article : Google Scholar : PubMed/NCBI
|