Introduction
Malignant peripheral nerve sheath tumors (MPNSTs)
are believed to arise from Schwann cells or nearby cells with
perineural differentiation. The incidence of MPNSTs is one per
100,000 cases. In total, ~50% of MPNST cases arise in patients with
neurofibromatosis type 1 (NF1; von Recklinghausen’s disease) and
the five-year overall survival rate is 34% (1). Malignant triton tumors (MTTs) are a
subgroup of MPNSTs, which display rhabdomyosarcomatous
differentiation and follow a particularly aggressive course. MTTs
account for <10% of MPNSs, and are identified by focal evidence
of skeletal muscle differentiation within the MPNSTs. Positive
immunohistochemical staining for desmin, actin and myogenin is
evidence of skeletal muscle differentiation (1). A recent study reported that the
five-year survival rate and median survival time of patients with
MTT were 14% and 13 months, respectively (2). To date, >100 cases of MTTs have
been reported in the English literature (2). Regarding the original location, MTTs
occur predominantly in the head, neck and trunk regions (3). Only eight cases have previously been
observed in the mediastinum (Table
I) (3–10). The current study presents the case
of a 42-year-old male patient with an MTT arising from the anterior
mediastinum. To the best of our knowledge, this is the fourth
report that has been documented in the English literature worldwide
regarding an MTT localized in the anterior mediastinum. Written
informed consent was obtained from the patient.
 | Table IExisting cases reported in the English
literature of MTTs located in the mediastinum. |
Table I
Existing cases reported in the English
literature of MTTs located in the mediastinum.
| Case/year/
(reference) | Gender/age,
years | von Recklinghausen’s
disease | Location | Treatment | Recurrence/
residual | Follow-up |
|---|
| 1/1984/(4) | F/31 | Yes | Anterior
mediastinum | Palliative surgery
radiotherapy | Yes | Overall survival
time, 3 months |
| 2/1984/(5) | M/29 | Yes | Posterior
mediastinum | No surgery | Yes | Overall survival
time, 6 months |
| 3/1985/(3) | F/70 | No | Mediastinum | Palliative
surgery | Yes | Alive with disease at
53 months |
| 4/1991/(6) | M/39 | No | Posterior
mediastinum | Palliative surgery
chemoradiotherapy | Yes | Overall survival
time, 15 months |
| 5/1996/(7) | F/17 | Yes | Anterior
mediastinum | Palliative surgery
radiotherapy | Yes | Overall survival
time, 7 months |
| 6/2002/(8) | M/35 | Yes | Middle
mediastinum | Radical surgery | No | Alive at 18
months |
| 7/2003/(9) | M/22 | No | Posterior
mediastinum | Radical surgery
radiotherapy | No | Alive at 98
months |
| 8/2006/(10) | M/30 | No | Anterior
mediastinum | Palliative surgery
chemoradiotherapy | Yes | Alive with disease at
12 months |
Case report
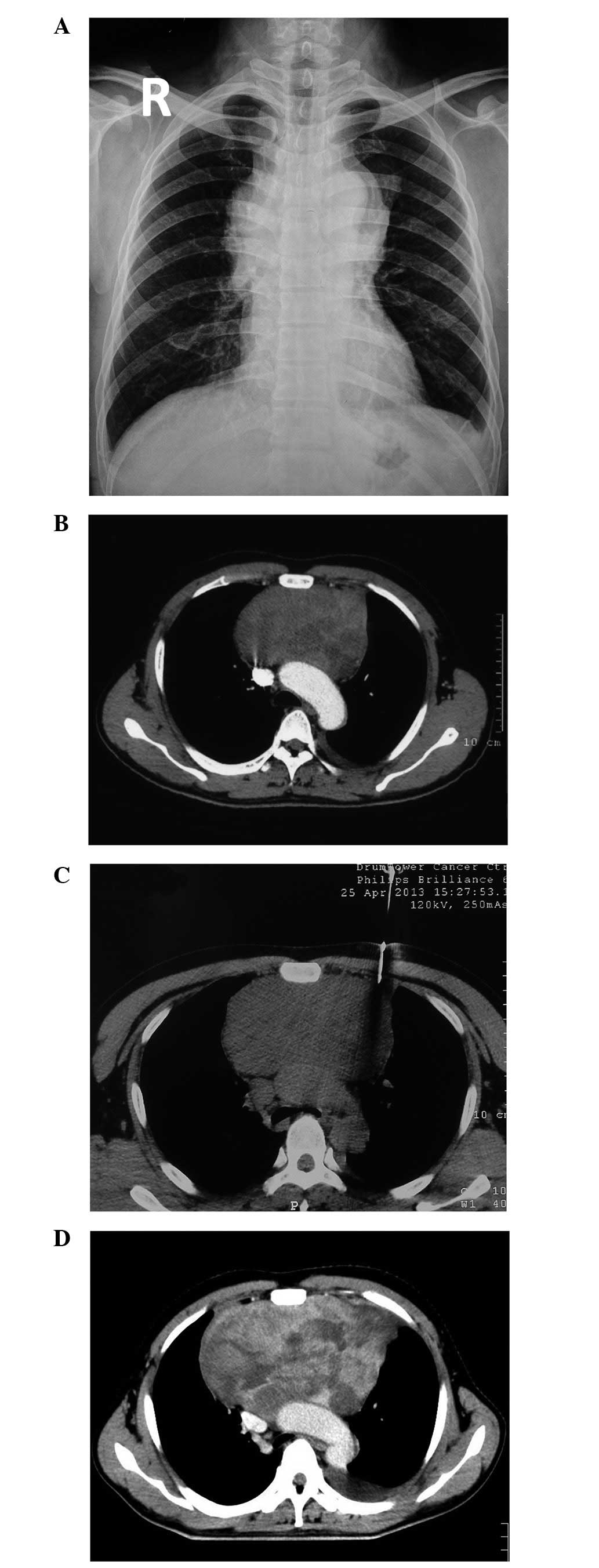
A 42-year-old male patient with a history of a dry
cough for 2 months and chest distress for 1 month was treated at
the clinic of Zhangjiagang Bo’ai Hospital (Suzhou, China) on April
23, 2013. The results of the chest radiograph (Fig. 1A) and enhanced computed tomography
(CT) scan (Fig. 1B) revealed a
large anterior mediastinal mass, measuring 14.8×12.0×11.5 cm in
size and invading the mediastinal great vessels. The patient was
then admitted to Nanjing Drum Tower Hospital (Nanjing, China) for
further assessment and therapy. In addition, a percutaneous core
cutting needle biopsy of the anterior mediastinal mass was
performed with CT guidance (Fig.
1C).
Pathological diagnosis of an MTT
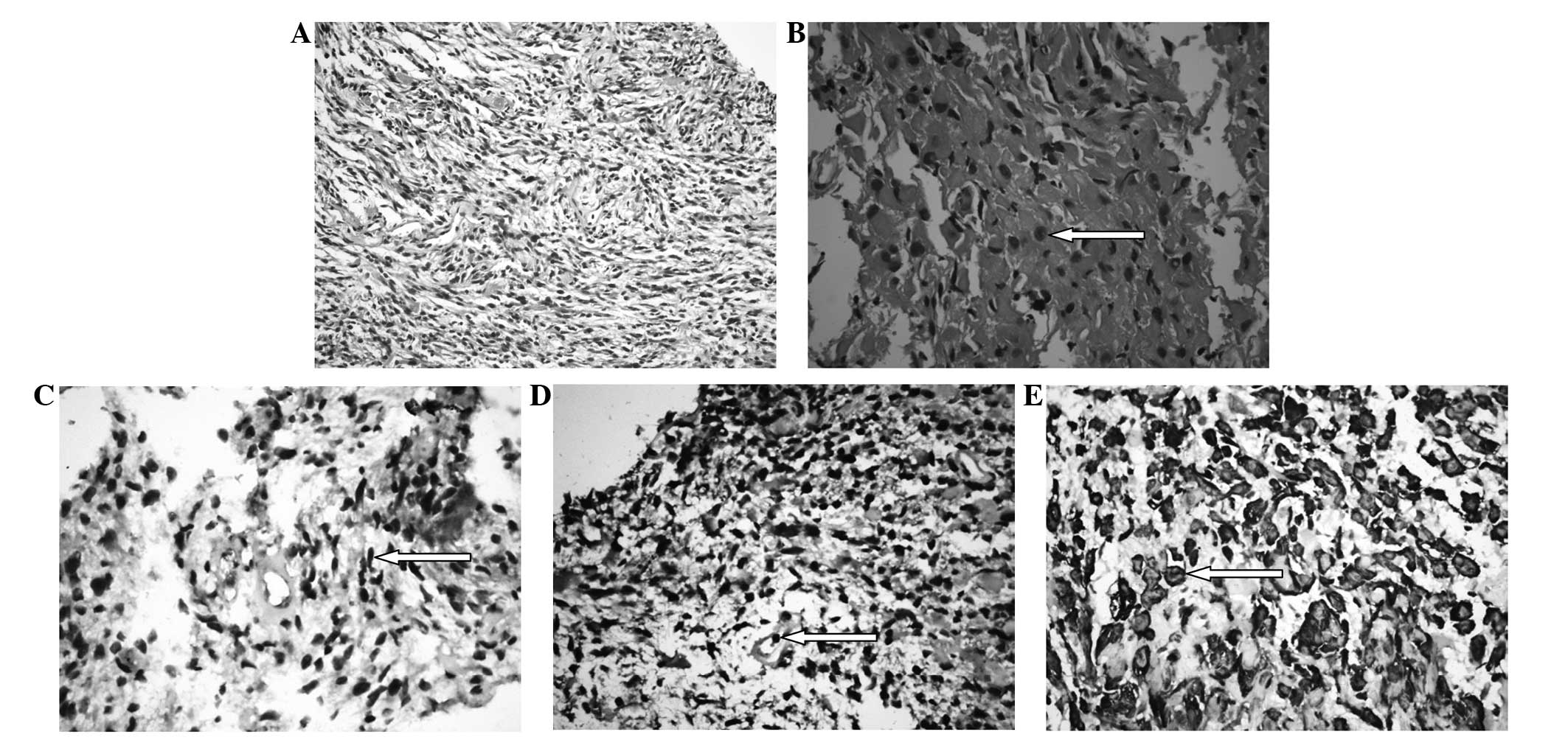
Histological analysis revealed a spindle cell tumor
with interlacing fascicles of wavy spindle cells and prominent
mitotic figures. Loose and impact arrangements were detected. In
certain focal areas, the tumor was comprised of round
rhabdomyoblasts, with abundant eosinophilic cytoplasm and eccentric
nuclei in a loose matrix. Immunohistochemical analysis revealed
that the spindle cells were positive for S-100, and the
rhabdomyoblasts were positive for myogenin and desmin, respectively
(Fig. 2). Simultaneously, the tumor
cells were negative for neuron-specific enolase, B-cell lymphoma 2,
cytokeratin 19, cluster of differentiation (CD)57, myogenic
regulatory protein, neuronal nuclear antigen and smooth muscle
actin.
Considering the locally advanced staging of the
anterior mediastinal MTT, surgical excision was ruled out. Chest
computed tomography re-examination revealed that the anterior
mediastinal MTT had enlarged rapidly to 17.0×15.0×12.0 cm on May
23, 2013 (Fig. 1D). Palliative
intensity-modulated radiotherapy with concurrent intravenous and
interstitial chemotherapy using liposomal paclitaxel was performed.
The patient remains alive with the disease and is currently
receiving traditional Chinese medicine.
Discussion
In 1932, Masson (11) was the first to describe a neurogenic
tumor accompanied by rhabdomyoblasts. In 1973, Woodruff et
al introduced the term MTT in a review of seven cases (12). The majority of pathologists use the
term MTT to refer to tumors that exhibit the features of MPNSTs and
contain rhabdomyoblastic elements, no matter what their location
(3).
Malignant tumors arising from Schwann cells of
peripheral nerves or within existing neurofibromas are collectively
referred to as MPNSTs. MTTs are a subgroup of MPNSTs, which have
been reported to display rhabdomyosarcomatous differentiation and
follow a particularly aggressive course (13). MTT accounts for <10% of MPNSTs
and is identified by focal evidence of skeletal muscle
differentiation within a MPNST. NF1 (von Recklinghausen’s disease)
has been associated with an increased risk of MPNST and MTT. In
total, ~69% of MTT cases are diagnosed in patients with von
Recklinghausen’s disease and occur in young male patients, whereas
the remaining 31% are sporadic cases mostly occurring in older
females (3). The results of
previous studies have differed with regard to the impact of NF1 on
the prognosis of patients with these tumors, although the general
consensus is that NF1 is a negative prognostic factor. In the
present study, the patient with anterior mediastinal MTT did not
suffer from von Recklinghausen’s disease.
The cell of origin of MTT remains unclear, although
the presence of neural cells and rhabdomyoblasts has led certain
authors to hypothesize that these two cell components were derived
from less-differentiated neural crest cells. These cells have
mesodermal and ectodermal differentiation potential and thus
possess the ability to develop skeletal and neural components.
Direct evidence for the potential of schwannoma cells to exhibit
myogenic differentiation has been previously shown (14). Immunohistochemical staining aids the
identification of the origin of cells. Nerve sheath differentiation
is confirmed by S-100 protein and Leu-7 (CD57) positivity, whereas
rhabdomyoblastic differentiation is confirmed by positivity to
desmin, actin and myogenin. In the present case, the neoplasm was
positive for S-100, desmin and myogenin, which indicated nerve
sheath and rhabdomyoblastic components (2).
Previously published literature has revealed a poor
prognosis for MTT. Local recurrence has been observed to be common
following tumor excision, while lymphatic invasion and lymph node
involvement has not been reported in patients with MTT. Given the
rarity of MTT, only case reports and small series of patients have
been studied. In 2012, McConnell and Giacomantonio published the
largest study to date, including a total of 124 MTT cases from the
English and French literature. In the study, the five-year survival
rate of MTT was 14%, which was comparable to the previously
published five-year survival rate of 11–12%, but significantly
worse than the five-year survival rate of other MPNSTs (34–52%).
The median survival time of patients with MTT was 13 months, the
overall local recurrence rate was 50% and the median time to
progression was 6 months. The study suggested that complete
surgical resection and adjuvant radiotherapy should be the gold
standard treatment for MTT. The study also concluded that
conventional chemotherapy does not appear to be of benefit
(2).
With regard to location, MTTs occur predominantly in
the head, neck and trunk regions. In total, ~20% of MTT cases arise
in the head and neck, with 32% in the trunk and 24% in the
extremities (15,16). To date, only eight cases located in
the mediastinum have been reported, among which, three were in the
anterior mediastinum, three in the posterior mediastinum and one in
the middle mediastinum (Table I).
To the best of our knowledge, this is only the fourth study of an
MTT localized in the anterior mediastinum that has been documented
in the English literature.
References
|
1
|
Scheithauer BW: Malignant peripheral nerve
sheath tumour (MPNST). WHO Classification of Tumours of the Central
Nervous System. Louis DN: World Health Organization Publ., Corp;
Lyon: pp. 160–162. 2007
|
|
2
|
McConnell YJ and Giacomantonio CA:
Malignant triton tumors-complete surgical resection and adjuvant
radiotherapy associated with improved survival. J Surg Oncol.
106:51–56. 2012. View Article : Google Scholar
|
|
3
|
Brooks JS, Freeman M and Enterline HT:
Malignant triton tumor. Natural history and immunohistochemistry of
nine new cases with literature review. Cancer. 55:2543–2549. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ducatman BS and Scheithauer BW: Malignant
peripheral nerve sheath tumors with divergent differentiation.
Cancer. 54:1049–1057. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Daimaru Y, Hashimoto H and Enjoji M:
Malignant ‘triton’ tumors: a clinicopathologic and
immunohistochemical study of nine cases. Human Pathol. 15:768–778.
1984.
|
|
6
|
Wong SY, Teh M, Tan YO and Best PV:
Malignant glandular triton tumor. Cancer. 67:1076–1083. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Otani Y, Morishita Y, Yoshida I, et al: A
malignant triton tumor in the anterior mediastinum requiring
emergency surgery: report of a case. Surg Today. 26:834–836. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bose AK, Deodhar AP and Duncan AJ:
Malignant triton tumor of the right vagus. Ann Thorac Surg.
74:1227–1228. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lang-Lazdunski L, Pons F and Jancovici R:
Malignant ‘triton’ tumor of the posterior mediastinum: prolonged
survival after staged resection. Ann Thorac Surg. 75:1645–1648.
2003.
|
|
10
|
Zisis C, Fragoulis S, Rontogianni D,
Stratakos G and Bellenis I: Malignant triton tumour of the anterior
mediastinum as incidental finding. Monaldi Arch Chest Dis.
65:222–224. 2006.PubMed/NCBI
|
|
11
|
Masson P: Recklinghausen’s
Neurofibromatosis, Sensory Neuromas and Motor Neuromas.
International Press; New York, NY: 1932
|
|
12
|
Woodruff JM, Chernik NL, Smith MC, Millett
WB and Foote FW Jr: Peripheral nerve tumors with
rhabdomyosarcomatous differentiation (malignant ‘triton’ tumors).
Cancer. 32:426–439. 1973.
|
|
13
|
Stasik CJ and Tawfik O: Malignant
peripheral nerve sheath tumor with rhabdomyosarcomatous
differentiation (malignant triton tumor). Arch Pathol Lab Med.
130:1878–1881. 2006.
|
|
14
|
Haddadin MH, Hawkins AL, Long P, et al:
Cytogenetic study of malignant triton tumor: a case report. Cancer
Genet Cytogenet. 144:100–105. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Victoria L, McCulloch TM, Callaghan EJ and
Bauman NM: Malignant triton tumor of the head and neck: a case
report and review of the literature. Head Neck. 21:663–670. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bhatt S, Graeme-Cook F, Joseph MP and
Pilch BZ: Malignant triton tumor of the head and neck. Otolaryngol
Head Neck Surg. 105:738–742. 1991.PubMed/NCBI
|