Introduction
Hepatocellular carcinoma (HCC), the sixth most
common cancer on a global scale, is the third major cause of
cancer-related mortalities and causes ~598,000 fatalities annually
(1). In recent years, ~81.5% of
HCCs have been correlated with chronic viral infection [hepatitis B
virus (HBV) and hepatitis C virus (HCV) infection], whereas 18.5%
have been associated with non-viral causes [HBV surface antigen
(HBsAg)-negative and HCV antibody (Ab)-negative] in mainland China
(2). For areas in which HBV
infection is prevalent, including China, the HBV vaccine has
dramatically decreased the incidence of HBV-related HCC (3). Recent developments in the management
of patients infected with HBV and/or HCV by specific antiviral
therapy, including interferon and nucleotide analogues, has also
led to a decrease of viral infection-related HCC development and
improved its prognosis (4,5). However, with the decrease of HBV
and/or HCV-related HCC, the incidence of non-viral HCC is gradually
increasing (6).
It has been estimated that 60–70% of patients with
HCC present with an intermediate to advanced stage of disease at
diagnosis, and the majority of the tumors are unresectable,
particularly the non-viral HCC patients who have not undergone a
surveillance program for viral-related HCC (7,8).
Transarterial chemoembolization (TACE) is the first-line of
treatment for unresectable HCC, and randomized controlled trials
have confirmed its benefits in improving the median survival rate
(9).
Recent studies have shown that components of
metabolic syndrome, including diabetes mellitus (DM), obesity and
hyperlipidemia, are significant risk factors for non-viral HCC
(10), and the presence of DM at
baseline is highly associated with the development of non-viral HCC
(11). Insulin resistance, which
plays a crucial role in the pathogenesis of DM, is closely
associated with the carcinogenesis of HCC through high energy
intake, increased cell proliferation and the suppression of
apoptosis (12). In addition,
systemic inflammation, which can induce insulin resistance through
reducing insulin sensitivity, is also involved in various stages of
HCC tumorigenesis (13–15). Further studies have demonstrated
that pre-existing DM can worsen the outcome of patients with HCC
undergoing surgical and non-surgical therapy (16–18),
and that systemic inflammation markers, including the neutrophil to
lymphocyte ratio (NLR), can also predict the survival of HCC
patients (19). However, little
information has been focused on the effect of pre-existing DM and
baseline NLR on the overall survival (OS) rate of non-viral HCC.
Therefore, it would be important to elucidate the association
between pre-existing DM, baseline NLR and OS in non-viral HCC. In
addition, the significance of pre-existing DM and baseline NLR in
non-viral HCC survival has not yet been explicitly explored.
The present study examined the clinical value of
pre-existing DM and the NLR, which were measured when patients with
non-viral HCC undergoing TACE were enrolled in a large number. The
present findings also evaluated the combined prognostic value of
pre-existing DM and NLR in predicting the OS rate of non-viral HCC
patients. Additionally, the correlation between pre-existing DM,
baseline NLR and other clinical pathological factors of non-viral
HCC was identified.
Patients and methods
Patient selection
A total of 138 patients with non-viral HCC that was
newly diagnosed between March 2002 and August 2012 at Tongji
Hospital, Huazhong University of Science and Technology (Wuhan,
Hubei, China) were prospectively collected and retrospectively
analyzed. HCC was diagnosed on the basis of a liver biopsy or
clinical criteria, including dynamic computed tomography (CT)
images and magnetic resonance imaging (MRI), with or without
elevated serum α-fetoprotein (AFP) levels (>200 ng/ml) (20). The patients with non-viral HCC were
defined as those who had serum that was negative for HBsAg and HCV
Ab. All the non-viral HCC patients received TACE treatment. The
present study was approved by the Ethics Committees of Huazhong
University of Science and Technology in accordance with the ethical
guidelines of the 1975 Declaration of Helsinki. Consent was
obtained from either the patient or the patient’s family.
TACE procedure
TACE treatment was a type of intra-arterial
chemotherapy using three combinations of 40 mg cisplatin, 6 mg
mitomycin C and 1,000 mg 5-fluorouracil, while the embolization
agents used were gelatin sponges and lipiodol (5–20 ml, according
to the tumor size).
Clinicopathological variables and
follow-up
Demographic data, including age and gender, were
collected at the time of diagnosis. Hematological data, including
neutrophil, lymphocyte and platelet counts, and biochemical data,
including aspartate aminotransferase (AST), alanine
aminotransferase (ALT), γ-glutamyl transpeptidase (GGT), alkaline
phosphatase (ALP), albumin, total bilirubin (TBIL), AFP, total
cholesterol and blood glucose levels and the international
normalized ratio (INR), were measured using an Abbott Aeroset
AutoAnalyzer (Abbott Diagnostics, Abbott Park, IL, USA) according
to standard techniques for each patient at the time of HCC
diagnosis. Anti-HCV Ab and HBsAg in sera were assayed using the EIA
Cobas Core Test (Hoffmann-La Roche, Ltd., Basel, Switzerland).
The diagnosis of pre-existing DM was based on the
presence of a fasting plasma glucose level of ≥7.0 mmol/l on at
least two occasions, a 2-h plasma glucose of ≥11.1 mmol/l in a 75-g
oral glucose tolerance test or the requirement for oral
hypoglycemic agents and/or insulin to control glucose levels. The
NLR was calculated by dividing the neutrophil count by the
lymphocyte count, and NLR measurements were obtained without
obvious infection. An elevated NLR was defined as ≥5, in agreement
with a previous study (19). The
presence of a portal vein tumor thrombus (PVTT) was detected by
means of ultrasound, a contrast-enhanced CT scan or MRI. The
maximum tumor diameter and number of tumors were measured by means
of ultrasound, dynamic CT scan or MRI. Hypertension was defined as
a systolic blood pressure of >140 mmHg or a diastolic blood
pressure of >90 mmHg on two occasions in the medical record of
the patient. The Child-Turcotte-Pugh classification, which is based
on the serum levels of bilirubin and albumin, prothrombin time
prolongation and the severity of encephalopathy and ascites, was
assessed. An elevated serum GGT was defined as >50 IU/l (normal
range, 11–50 IU/l) and an elevated serum ALP was >150 U/l
(normal range, 40–150 U/l). For surveillance of the OS rate of the
patients with HCC following TACE treatment, the time of the initial
TACE treatment was defined as day zero and patients were evaluated
every one to three months.
Statistical analysis
The differences between groups were analyzed using
Pearson’s χ2 test for the categorical variables, and a
one-way analysis of variance was used for the continuous variables.
Cox’s proportional hazard model was applied to explore the
independent prognostic value of each variable. A survival analysis
of the various clinical factors was carried out using Kaplan-Meier
statistics and compared by log-rank test. The correlation between
two variables was examined by Spearman’s correlation analysis. All
statistical analyses were conducted using SPSS, version 13.0 (SPSS,
Inc., Chicago, IL, USA). P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics
Between 2002 and 2012, a total of 138 patients with
non-viral HCC, who underwent initial treatment of TACE, were
recruited. All clinical variables were obtained from patients at
baseline at the time of recruitment into the study, and baseline
characteristics are shown in Table
I. The mean age was 56.8±12.5 years and the majority of
patients were male (n=99, 71.7%). At diagnosis, the number of
patients with pre-existing DM and elevated NLR was 34 (24.6%) and
46 (33.3%), respectively. In total, 105 (76.1%) patients were
classified as Child-Pugh class A, while 33 (23.9%) patients
belonged to Child-Pugh class B. The mean maximum tumor diameter was
8.7±4.5 cm and the number of patients with a solitary tumor was 63
(45.7%). The presence of a PVTT was recorded in 67 (48.6%)
patients. The number of patients who received one session of TACE
was 115 (83.3%), whereas the number who received >1 session was
23 (16.7%). The mean levels of serum ALT, AST, ALB, TBIL, ALP, GGT,
AFP, PLT, INR and NLR were 51.7±67.1 U/l, 70.6±85.2 U/l, 38.9±5.3
g/l, 17.9±24.8 μmol/l, 200.4±170.3 U/l, 201.0±230.0 U/l,
7697.3±21041.3 ng/ml, (189.9±96.1)x109/l, 1.06±0.11 and
4.55±2.71, respectively.
 | Table IBaseline characteristics of all
patients. |
Table I
Baseline characteristics of all
patients.
| Characteristics | Value |
|---|
| Age (years) | 56.8±12.5 |
| Gender (M/F) | 99/39 |
| Presence of DM
(yes/no) | 34/104 |
| NLR (≥5/<5) | 46/92 |
| Child-Pugh class
(A/B) | 105/33 |
| Maximum tumor
diameter (cm) | 8.7±4.5 |
| No. of tumors
(single/multiple) | 63/75 |
| Presence of PVTT
(yes/no) | 67/71 |
| No. of TACE
procedures (1/≥1) | 115/23 |
| ALT (U/l) | 51.7±67.1 |
| AST (U/l) | 70.6±85.2 |
| Albumin (g/l) | 38.9±5.3 |
| TBIL (μmol/l) | 17.9±24.8 |
| ALP (U/l) | 200.4±170.3 |
| GGT (U/l) | 201.0±230.0 |
| AFP (ng/ml) | 7697.3±21041.3 |
| Platelet count
(x109/l) | 189.9±96.1 |
| INR | 1.06±0.11 |
| NLR | 4.55±2.71 |
Prognostic factors affecting the survival
of patients with non-viral HCC
To identify the variables affecting the survival
rate of patients with non-viral HCC, the factors that exhibited a
potential impact on the prognosis of non-viral HCC were examined
(Table II). Of those factors,
elevated GGT [P=0.04; hazard ratio (HR), 1.519; 95% confidence
interval (CI), 1.019–2.265], tumor size (P=0.014; HR, 1.723; 95%
CI, 1.114–2.665), tumor multiplicity (P=0.03; HR, 1.483; 95% CI,
1.038–2.119), presence of a PVTT (P<0.001; HR, 4.336; 95% CI,
2.955–6.363), pre-existing DM (P=0.003; HR, 1.868; 95% CI,
1.239–2.816) and an elevated baseline NLR (P<0.001; HR 2.136;
95% CI, 1.466–3.114) were significantly associated with poorer
survival in the univariate analysis. The multivariate analysis
showed that the presence of a PVTT (P<0.001; HR, 4.235; 95% CI,
2.787–6.436), pre-existing DM (P=0.006; HR, 1.843; 95% CI,
1.190–2.854) and an elevated NLR (P<0.001; HR, 2.126; 95% CI,
1.429–3.165) were identified as independent poor prognostic factors
for patients with non-viral HCC who underwent TACE. When the
combination of pre-existing DM and elevated NLR was analyzed as one
factor, the combination of DM and NLR (P<0.001; HR, 2.235; 95%
CI, 1.488–3.357) together with the presence of a PVTT (P<0.001;
HR, 4.466; 95% CI, 2.924–6.822) were identified as independent
factors for poor survival compared with pre-existing DM or an
elevated NLR alone.
| Table IIUnivariate and multivariate analysis
of prognostic factors for OS rate by Cox’s regression model. |
Table II
Univariate and multivariate analysis
of prognostic factors for OS rate by Cox’s regression model.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| GGT (U/l) |
| Normal (n=36) | 1.519
(1.019–2.265) | 0.040 | 1.085
(0.707–1.666) | 0.707 |
| Elevated
(n=102) | | | | |
| Maximum tumor
diameter |
| <5 cm
(n=30) | 1.723
(1.114–2.665) | 0.014 | 1.379
(0.873–2.178) | 0.168 |
| ≥5 cm (n=108) | | | | |
| No. of tumors |
| Single (n=63) | 1.483
(1.038–2.119) | 0.030 | 1.119
(0.759–1.650) | 0.570 |
| Multiple
(n=75) | | | | |
| Presence of
PVTT |
| Absence
(n=71) | 4.336
(2.955–6.363) | <0.001 | 4.235
(2.787–6.436) | <0.001 |
| Presence
(n=67) | | | | |
| Presence of DM |
| Absence
(n=104) | 1.868
(1.239–2.816) | 0.003 | 1.843
(1.190–2.854) | 0.006 |
| Presence
(n=34) | | | | |
| NLR |
| <5 (n=92) | 2.136
(1.466–3.114) | <0.001 | 2.126
(1.429–3.165) | <0.001 |
| ≥5 (n=46) | | | | |
The prognostic value of the other metabolic
components, including the presence of hypercholesterolemia and
hypertension, was also examined in Cox’s regression model, and no
statistically significant difference between the presence of
hypercholesterolemia and hypertension and the absence of these
factors was observed in the univariate analysis (P>0.05).
Correlation between DM, NLR and clinical
factors of non-viral HCC patients
The presence of a PVTT in the patients with DM was
significantly increased compared with the patients without DM (67.6
vs. 42.3%). In contrast to patients with an elevated NLR, patients
with a normal NLR exhibited a significantly decreased presence of a
PVTT (42.4 vs. 60.9%) and more single liver tumors (52.2 vs.
32.6%), respectively.
The association between PVTT, elevated GGT and
pre-existing DM was further examined (Table III). The result demonstrated that
pre-existing DM was significantly correlated with the presence of a
PVTT (Spearman’s ρ, 0.218; P=0.01) and elevated GGT (Spearman’s ρ,
0.186; P=0.029). The correlation of the presence of a PVTT and the
number of tumors with an elevated NLR was also examined (Table III). The result identified that an
elevated NLR significantly correlated with the presence of a PVTT
(Spearman’s ρ, 0.174; P=0.041) and multiple tumors (Spearman’s ρ,
0.185; P=0.03).
| Table IIISignificant Spearman’s correlation
coefficients (ρ) for patients with or without DM and for those with
baseline/elevated NLR and the presence of PVTT or elevated GGT. |
Table III
Significant Spearman’s correlation
coefficients (ρ) for patients with or without DM and for those with
baseline/elevated NLR and the presence of PVTT or elevated GGT.
| With DM/without
DM | | NLR≥5/NLR<5 |
|---|
|
| |
|
|---|
| Variable | ρ | P-value | Variable | ρ | P-value |
|---|
| Presence of
PVTT | 0.218 | 0.01 | Multiple
tumors | 0.185 | 0.03 |
| Elevated GGT | 0.186 | 0.03 | Presence of
PVTT | 0.174 | 0.04 |
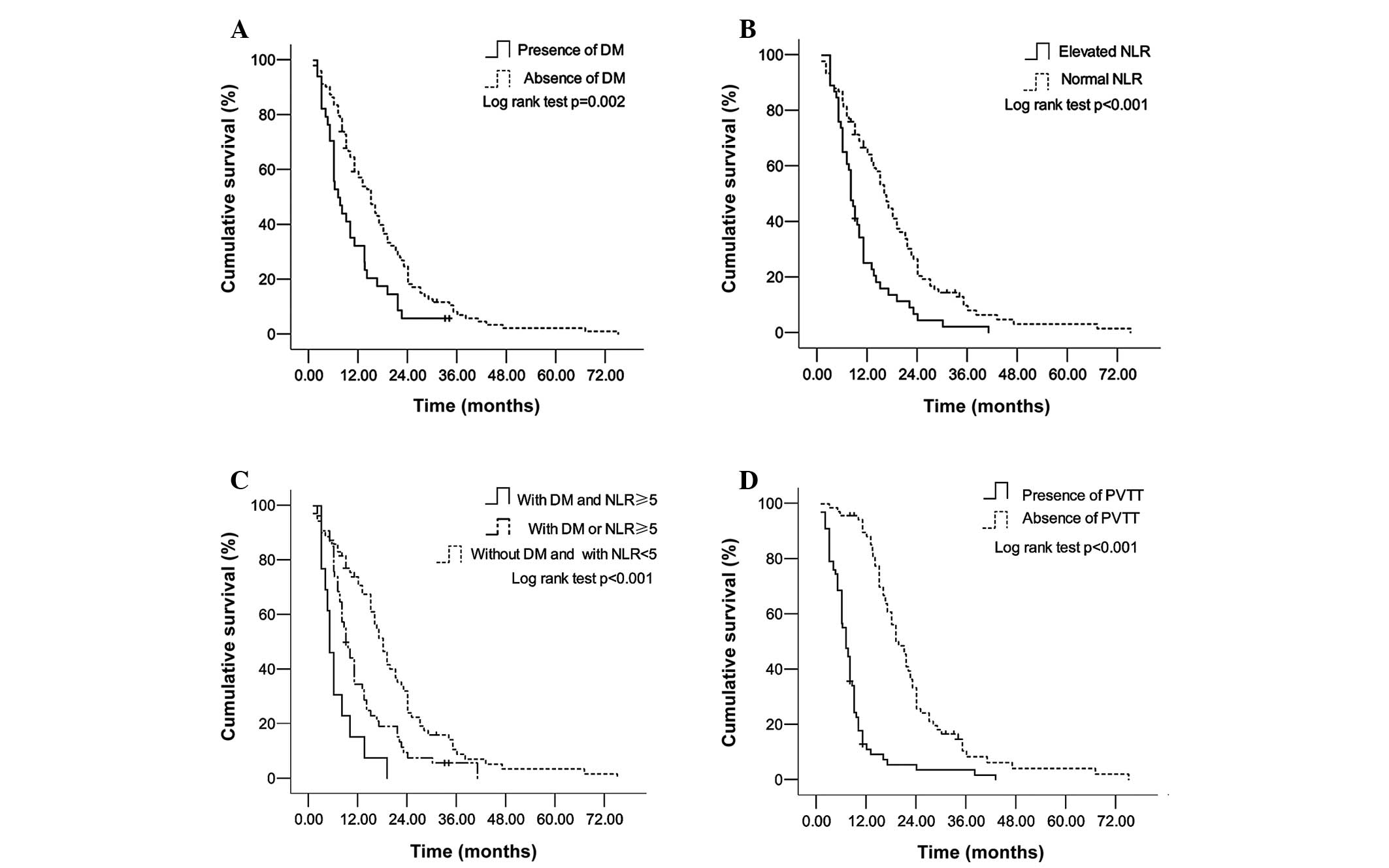
OS according to DM status, NLR level and
PVTT presence in non-viral HCC patients
The median follow-up period was 12 months (range,
2–76 months) for the non-viral HCC patients. Since pre-existing DM,
elevated baseline NLR and the presence of a PVTT independently
predicted the OS rate of non-viral HCC in the multivariate
analysis, the differences in survival rate between the presence and
absence of DM, elevated and normal NLR and the presence and absence
of a PVTT among the whole group were evaluated. As described in
Fig. 1A, the OS rate among patients
with pre-existing DM (1-year cumulative survival rate, 32.4%;
3-year cumulative survival rate, 0%; and 5-year cumulative survival
rate, 0%) was significantly lower than among patients without DM
(1-year survival rate, 57.3%; 3-year survival rate, 7.1%; and
5-year survival rate, 1.2%) (log-rank test, P=0.002). Similarly,
the survival rate in the elevated NLR group (1-year survival rate,
25.2%; 3-year survival rate, 2.3%; and 5-year survival rate, 0%)
was significantly lower when compared with the normal NLR group
(1-year survival rate, 64.3%; 3-year survival rate, 8.2%; and
5-year survival rate, 1.6%) (log-rank test, P<0.001; Fig. 1B). A specific Kaplan-Meier analysis
was performed (Fig. 1C) to detect
the effect of a combined use of pre-existing DM and NLR on patient
survival. There was a significant stepwise improvement in the OS
rate of patients with pre-existing DM and elevated NLR, with
pre-existing DM or elevated NLR and with an absence of DM and
normal NLR (log-rank test, P<0.001). This revealed the advantage
of the combined use of pre-existing DM and elevated NLR in
non-viral HCC patients. Finally, the survival time of patients with
the presence of a PVTT was examined (Fig. 1D), and it was shown that these
patients exhibited a significantly poorer survival rate (1-year
cumulative survival rate, 11.2%; 3-year cumulative survival rate,
1.9%; and 5-year cumulative survival rate, 0%) than patients
without a PVTT (1-year survival rate, 88.2%; 3-year survival rate,
8.5%; and 5-year survival rate, 2.1%) (log-rank test,
P<0.001).
Discussion
To investigate the impact of clinical factors on the
OS rate of patients with unresectable non-viral HCC who underwent
TACE, the factors that exhibited a potential impact on the
prognosis of non-viral HCC were compared. It was found that
pre-existing DM, an elevated baseline NLR and the presence of a
PVTT independently predicted a poor OS rate in non-viral HCC
patients. In addition, the combination of DM and NLR appeared to be
a stronger predictor for OS than DM or NLR alone. It was observed
that DM and NLR were significantly correlated with the indicators
of intrahepatic metastasis.
Several studies have confirmed that DM significantly
promotes the progression of non-viral HCC (11,21).
Therefore, in recent years, with the hypothesis in mind that DM may
be able to predict the survival of HCC, several early studies have
shown that DM is an independent factor for poorer survival in
patients undergoing surgical and non-surgical treatment (17,18,22).
Similar to the aforementioned studies, the present study also
observed that among non-viral HCC patients who had undergone TACE,
the patients with DM exhibited a poorer OS rate than those without
DM. However, another study reported that the survival difference
between patients with and without diabetes was not significant in a
Child-Pugh B group undergoing non-surgical treatment (18). It was assumed that the inconsistent
results may be caused by the difference in HCC etiology (major
viral causes vs. non-viral causes) and non-surgical treatment
strategy (TACE, percutaneous injection therapy vs. TACE) between
the two studies. In addition, a previous study also showed that
there was no significant difference in the five-year OS rate
between non-viral HCC patients with DM and without DM (23). A probable reason for this divergency
may be that more patients without DM were enrolled (75.4 vs. 41.7%)
and due to the fact that varying treatment strategies were adopted
(TACE vs. resection) in the present study. Therefore, further
studies are necessary to investigate the exact role of these
divergencies in the prognosis of non-viral HCC.
Although a previous study identified that the
mechanism underlying effect of DM on the prognosis of HCC could be
diabetes-related liver function failure (18), another study showed that DM-related
insulin resistance may be involved in the hepatocarcinogenesis of
non-viral HCC (24). DM has been
further confirmed to positively correlate with macrovascular
invasion among transplanted HCC patients (25). PVTT, which is a type of advanced
macrovascular invasion, also indicates a poorer prognosis for
patients with HCC (26). Elevated
GGT has also been found to be a significant risk factor for
microvascular invasion in patients with multinodular HCC (27). In the present study, it was found
that the patients with DM exhibited a significantly higher ratio
for the presence of PVTT and elevated GGT, and that DM correlated
positively with them. It was inferred that DM may affect the
prognosis of non-viral HCC by inducing macrovascular and
microvascular invasion, particularly by forming a tumor thrombus in
the portal vein.
In patients with cancer, systemic inflammation
measured by NLR plays crucial roles at various stages of HCC
tumorigenesis (14,15). A few studies have demonstrated that
the NLR could predict the OS rate in HCC patients undergoing
surgical and non-surgical treatment (19,28).
An elevated NLR can signify that relative neutrophilia is
correlated with more aggressive tumor behavior in uterine cancer
(29). Neutrophils also promote
tumor invasion by secreting neutrophil-derived hepatocyte growth
factor and by promoting the adhesion and motility of cancer cells
(30–32). As in the aforementioned studies, the
present study confirmed that an elevated baseline NLR predicted a
poorer OS rate in patients with non-viral HCC. Additionally, an
elevated NLR was correlated with tumor multiplicity and the
presence of a PVTT, which were indicators of the intrahepatic
metastasis of HCC. These data indicate that an elevated baseline
NLR may result in a poorer outcome of HCC through
neutrophil-promoted intrahepatic metastasis.
The carcinogenic effects of insulin resistance in
HCC may be the activation of insulin-like growth factor (IGF)-1 and
2 stimulated by compensatory hyperinsulinemia (33). IGF-1 may stimulate cancer
angiogenesis in part by upregulating vascular endothelial growth
factor (VEGF) expression (34),
whereas IGFs (IGF-1 and IGF-2) promote vasculogenesis in embryonic
stem cells through the upregulation of VEGF (35). All these studies indicate that VEGF
is extremely significant in the carcinogenesis of HCC. Besides
these findings, other data has indicated that VEGF released by
neutrophils also promotes angiogenesis in the progression of
cancer, including HCC (36). In the
present study, it was observed that a combination of DM and NLR
could predict a stepwise alteration in the OS rate of non-viral
HCC. Since DM and neutrophils are closely associated with VEGF, we
hypothesize that pre-existing DM together with an elevated NLR may
affect the survival rate of non-viral HCC through the VEGF
angiogenesis pathway, and a combined use of these two factors may
be a more valuable prognostic indicator for non-viral HCC patients
undergoing TACE.
The present study confirmed that the presence of a
PVTT predicted a poor survival rate in patients with HCC, as
published previously (26). While
the previous study (26)
demonstrated the predictive power of the presence of a PVTT in
virus-related HCC, the present study also observed that the
presence of a PVTT exhibited a prognostic power on non-viral HCC.
Although GGT level, tumor multiplicity and tumor diameter have been
identified as independent prognostic factors for HCC (37,38),
the multivariate analysis in the present study could not identify a
GGT level of >50 U/l, multiple tumors or a tumor diameter of ≥5
cm as independent factors. The reason for this may be that
pre-existing DM, an elevated baseline NLR and the presence of a
PVTT exhibited a stronger prognostic impact than GGT, tumor
multiplicity or tumor diameter on the progression of non-viral
HCC.
There are certain limitations to the present study.
First, the study was a retrospective observational study with a
lack of Child-Pugh score follow-up, which is an indicator of
hepatic functional reserve. Therefore, although several studies
have shown that NLR and DM affected the long-term survival of HCC
partly through their effect on hepatic functional reserve (18,38),
the effect of DM and NLR on the survival of non-viral HCC through
their impact on hepatic reserve cannot be confirmed. Furthermore,
due to the lack of recurrence of a follow-up, the association
between DM, NLR and liver cancer specific survival cannot be
verified. Finally, the present study was confined to a single
institution, and it is possible that the associations observed were
due to chance. Confirmatory prospective studies in larger cohorts,
including multiple institutions, are required.
In conclusion, despite these limitations, the
present study demonstrated that pre-existing DM and an elevated
baseline NLR are independent prognostic indicators of the OS rate
in non-viral HCC treated with TACE. The combination of DM and NLR
appears to be a stronger predictor for the OS rate than DM or NLR
alone. Pre-existing DM and an elevated baseline NLR may affect the
OS rate by promoting the malignant progression of HCC. Further
clinical studies are required to clarify a more specific biological
mechanism underpinning the role of DM and NLR in non-viral
hepatocarcinogenesis.
Abbreviations:
|
DM
|
diabetes mellitus
|
|
HCC
|
hepatocellular carcinoma
|
|
OS
|
overall survival
|
|
TACE
|
transarterial chemoembolization
|
|
HBV
|
hepatitis B virus
|
|
HCV
|
hepatitis C virus
|
|
NLR
|
neutrophil to lymphocyte ratio
|
|
PVTT
|
portal vein tumor thrombus
|
|
AFP
|
α-fetoprotein
|
|
GGT
|
γ-glutamyl transpeptidase
|
|
INR
|
international normalized ratio
|
|
VEGF
|
vascular endothelial growth factor
|
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2
|
Shi J, Zhu L, Liu S and Xie WF: A
meta-analysis of case-control studies on the combined effect of
hepatitis B and C virus infections in causing hepatocellular
carcinoma in China. Brit J Cancer. 92:607–612. 2005.
|
|
3
|
Chang MH, You SL, Chen CJ, et al; Taiwan
Hepatoma Study Group. Decreased incidence of hepatocellular
carcinoma in hepatitis B vaccinees: a 20-year follow-up study. J
Natl Cancer Inst. 101:1348–1355. 2009.
|
|
4
|
Papatheodoridis GV, Lampertico P,
Manolakopoulos S and Lok A: Incidence of hepatocellular carcinoma
in chronic hepatitis B patients receiving nucleos(t)ide therapy: a
systematic review. J Hepatol. 53:348–356. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shiratori Y, Ito Y, Yokosuka O, et al;
Tokyo-Chiba Hepatitis Research Group. Antiviral therapy for cirρtic
hepatitis C: association with reduced hepatocellular carcinoma
development and improved survival. Ann Intern Med. 142:105–114.
2005.
|
|
6
|
Hatanaka K, Kudo M, Fukunaga T, et al:
Clinical characteristics of NonBNonC- HCC: Comparison with HBV and
HCV related HCC. Intervirology. 50:24–31. 2007. View Article : Google Scholar
|
|
7
|
Llovet JM and Bruix J: Novel advancements
in the management of hepatocellular carcinoma in 2008. J Hepatol.
48(Suppl 1): S20–S37. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lencioni R, Chen XP, Dagher L and Venook
AP: Treatment of intermediate/advanced hepatocellular carcinoma in
the clinic: how can outcomes be improved? Oncologist. 15(Suppl 4):
S42–S52. 2010. View Article : Google Scholar
|
|
9
|
Llovet JM and Bruix J: Systematic review
of randomized trials for unresectable hepatocellular carcinoma:
Chemoembolization improves survival. Hepatology. 37:429–442. 2003.
View Article : Google Scholar
|
|
10
|
Nagaoki Y, Hyogo H, Aikata H, et al:
Recent trend of clinical features in patients with hepatocellular
carcinoma. Hepatol Res. 42:368–375. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Koh WP, Wang R, Jin A, Yu MC and Yuan JM:
Diabetes mellitus and risk of hepatocellular carcinoma: findings
from the Singapore Chinese Health Study. Brit J Cancer.
108:1182–1188. 2013. View Article : Google Scholar
|
|
12
|
Djiogue S, Nwabo Kamdje AH, Vecchio L, et
al: Insulin resistance and cancer: the role of insulin and IGFs.
Endocr Relat Cancer. 20:R1–R17. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mehta NN, McGillicuddy FC, Anderson PD, et
al: Experimental endotoxemia induces adipose inflammation and
insulin resistance in humans. Diabetes. 59:172–181. 2010.
View Article : Google Scholar
|
|
14
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899. 2010.
View Article : Google Scholar
|
|
15
|
Alison MR, Nicholson LJ and Lin WR:
Chronic inflammation and hepatocellular carcinoma. Recent Results
Cancer Res. 185:135–148. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ting CT, Chen RC, Chen CC, Liu MH, Chu D
and Kuo NW: Diabetes worsens the surgical outcomes in cirρtic
patients with hepatocellular carcinoma. Tohoku J Exp Med.
227:73–81. 2012.PubMed/NCBI
|
|
17
|
Huo TI, Hsu CY, Huang YH, et al: Diabetes
mellitus as an independent prognostic predictor and its association
with renal dysfunction in patients with hepatocellular carcinoma.
Liver Int. 30:198–207. 2010. View Article : Google Scholar
|
|
18
|
Huo TI, Wu JC, Lui WY, et al: Differential
mechanism and prognostic impact of diabetes mellitus on patients
with hepatocellular carcinoma undergoing surgical and nonsurgical
treatment. Am J Gastroenterol. 99:1479–1487. 2004. View Article : Google Scholar
|
|
19
|
Limaye AR, Clark V, Soldevila-Pico C, et
al: Neutrophil-lymphocyte ratio predicts overall and
recurrence-free survival after liver transplantation for
hepatocellular carcinoma. Hepatol Res. 43:757–764. 2012. View Article : Google Scholar
|
|
20
|
Bruix J and Sherman M; Practice Guidelines
Committee, American Association for the Study of Liver Diseases.
Management of hepatocellular carcinoma. Hepatology. 42:1208–1236.
2005. View Article : Google Scholar
|
|
21
|
Lagiou P, Kuper H, Stuver SO, Tzonou A,
Trichopoulos D and Adami HO: Role of diabetes mellitus in the
etiology of hepatocellular carcinoma. J Natl Cancer Inst.
92:1096–1099. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shau WY, Shao YY, Yeh YC, et al: Diabetes
mellitus is associated with increased mortality in patients
receiving curative therapy for hepatocellular carcinoma.
Oncologist. 17:856–862. 2012. View Article : Google Scholar
|
|
23
|
Kaibori M, Ishizaki M, Matsui K, Kitade H,
Matsui Y and Kwon AH: Evaluation of metabolic factors on the
prognosis of patients undergoing resection of hepatocellular
carcinoma. J Gastroenterol Hepatol. 26:536–543. 2011. View Article : Google Scholar
|
|
24
|
Kawamura Y, Ikeda K, Arase Y, et al:
Diabetes mellitus worsens the recurrence rate after potentially
curative therapy in patients with hepatocellular carcinoma
associated with nonviral hepatitis. J Gastroenterol Hepatol.
23:1739–1746. 2008. View Article : Google Scholar
|
|
25
|
Connolly GC, Safadjou S, Kashyap R, Chen
R, Orloff MS and Hezel AF: Diabetes mellitus impacts risk of
macrovascular invasion in patients undergoing transplantation for
hepatocellular carcinoma. BMC Gastroenterol. 13:92013. View Article : Google Scholar
|
|
26
|
Giannelli G, Pierri F, Trerotoli P, et al:
Occurrence of portal vein tumor thrombus in hepatocellular
carcinoma affects prognosis and survival: A retrospective clinical
study of 150 cases. Hepatol Res. 24:502002. View Article : Google Scholar
|
|
27
|
Zhao WC, Fan LF, Yang N, Zhang HB, Chen BD
and Yang GS: Preoperative predictors of microvascular invasion in
multinodular hepatocellular carcinoma. Eur J Surg Oncol.
39:858–864. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
McNally ME, Martinez A, Khabiri H, et al:
Inflammatory markers are associated with outcome in patients with
unresectable hepatocellular carcinoma undergoing transarterial
chemoembolization. Ann Surg Oncol. 20:923–928. 2013. View Article : Google Scholar
|
|
29
|
Tavares-Murta BM, Mendonça MA, Duarte NL,
et al: Systemic leukocyte alterations are associated with invasive
uterine cervical cancer. Int J Gynecol Cancer. 20:1154–1159. 2010.
View Article : Google Scholar
|
|
30
|
Imai Y, Kubota Y, Yamamoto S, et al:
Neutrophils enhance invasion activity of human cholangiocellular
carcinoma and hepatocellular carcinoma cells: an in vitro study. J
Gastroenterol Hepatol. 20:287–293. 2005. View Article : Google Scholar
|
|
31
|
McDonald B, Spicer J, Giannais B,
Fallavollita L, Brodt P and Ferri LE: Systemic inflammation
increases cancer cell adhesion to hepatic sinusoids by neutrophil
mediated mechanisms. Int J Cancer. 125:1298–1305. 2009. View Article : Google Scholar
|
|
32
|
Wu Y, Zhao Q, Peng C, Sun L, Li XF and
Kuang DM: Neutrophils promote motility of cancer cells via a
hyaluronan-mediated TLR4/PI3K activation loop. J Pathol.
225:438–447. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Siddique A and Kowdley KV: Insulin
resistance and other metabolic risk factors in the pathogenesis of
hepatocellular carcinoma. Clin Liver Dis. 15:281–296. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Oh JS, Kucab JE, Bushel PR, et al:
Insulin-like growth factor-1 inscribes a gene expression profile
for angiogenic factors and cancer progression in breast epithelial
cells. Neoplasia. 4:204–217. 2002. View Article : Google Scholar
|
|
35
|
Piecewicz SM, Pandey A, Roy B, Xiang SH,
Zetter BR and Sengupta S: Insulin-like growth factors promote
vasculogenesis in embryonic stem cells. PloS One. 7:e321912012.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Brandau S, Dumitru CA and Lang S: Protumor
and antitumor functions of neutrophil granulocytes. Semin
Immunopathol. 35:163–176. 2013. View Article : Google Scholar
|
|
37
|
Zhang JB, Chen Y, Zhang B, et al:
Prognostic significance of serum gamma-glutamyl transferase in
patients with intermediate hepatocellular carcinoma treated with
transcatheter arterial chemoembolization. Eur J Gastroenterol
Hepatol. 23:787–793. 2011. View Article : Google Scholar
|
|
38
|
Oh BS, Jang JW, Kwon JH, et al: Prognostic
value of C-reactive protein and neutrophil-to-lymphocyte ratio in
patients with hepatocellular carcinoma. BMC cancer. 13:782013.
View Article : Google Scholar : PubMed/NCBI
|