Introduction
Tuberculosis (TB) is a global threat to public
health. The World Health Organization reported that in 2011,
approximately two billion individuals were known to be infected
with Mycobacterium tuberculosis and 1.4 million deaths were
associated with TB (1). TB may be
categorized into pulmonary and extrapulmonary TB. Extrapulmonary TB
comprises 20% of all TB cases and occurs in a variety of organs
(2). TB of the thyroid gland is an
extremely rare disease.
Cancer is also a global threat and the second
leading cause of mortality following coronary artery disease, with
7.6 million deaths in 2008 (3).
Thyroid cancer is a common type of cancer. In the United States,
thyroid cancer comprises 1% of all cancers and accounts for 0.2% of
cancer mortality (4). Papillary
thyroid cancer (PTC) is the most common well-differentiated cancer
of the thyroid gland and accounts for 80–85% of well-differentiated
thyroid cancers (5).
The coexistence of malignant lesions and TB at the
same anatomical location in a patient is extremely rare, but has
been reported in various organs (6). However, only three cases in which
thyroid TB occurred concomitantly with thyroid cancer have been
reported (7–9). Among them, two cases of thyroid TB
were found post-operatively and one case of thyroid TB was
identified in the fine-needle aspiration cytology (FNAC). The
present study reports a case of coexisting TB and PTC diagnosed by
the histopathological examination of a resected thyroid specimen.
The patient provided written informed consent.
Case report
A 56-year-old female was admitted to the Department
of Breast and Thyroid Surgery (Shaoxing People’s Hospital,
Shaoxing, Zheijiang, China) in August 2012 due to the presence of
thyroid nodules on B-ultrasound. The patient first became aware of
these thyroid nodules during a regular health examination in 1997.
The nodules developed slowly and one of the nodules showed signs of
malignancy in the most recent B-mode ultrasound examination. The
patient had no history of pulmonary or extrapulmonary TB or any
known contact with any individuals with TB.
A clinical examination revealed a first to second
degree multinodular goiter, which was mobile, soft and not painful
on palpation. There was no palpable lymphadenopathy in the neck.
Thyroid function tests showed a hypothyroidism state: Increased
thyrotropic-stimulating hormone [TSH; 6.12 μIU/ml; normal range
(NR), 0.35–5.5 μIU/ml] and antithyroglobulin antibody levels (27.8
IU/ml; NR, ≤4.11 IU/ml); decreased free triiodothyronine (2.96
pmol/l; NR, 3.0–6.51 pmol/l) and triiodothyronine (0.9 nmol/l; NR,
0.92–2.79 nmol/l) concentrations; normal thyroxine and free
thyroxine, thyroglobulin and thyroid-binding globulin levels; and a
negative result for antithyroperoxidase antibody. Biochemical
analyses only showed elevated C-reactive protein levels (31.44
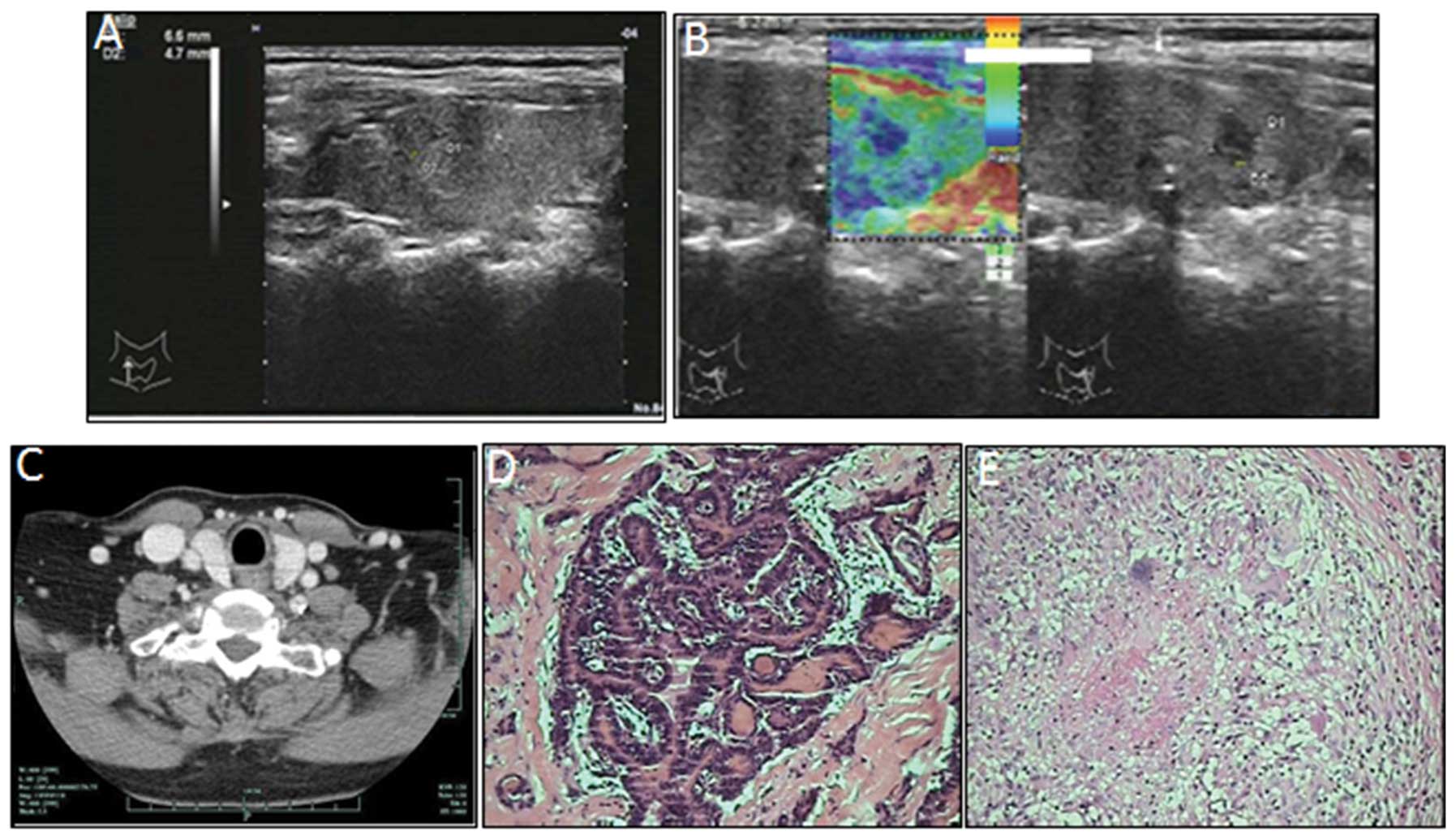
mg/l; NR, ≤8 mg/l). Thyroid B-mode ultrasonographyrevealed a number
of hypoechoic nodules in the bilateral lobe of the thyroid gland,
with sizes varying between 5 and 11 mm. However, one of these
nodules (7–8 mm in size) located near the top of the left thyroid
lobe was a heterogeneous hypoechoic lesion, and infiltrative
margins with microcalcifications were identified by ultrasonography
(Fig. 1). B-mode ultrasonography
showed a malignant nodule and cervical lymphadenectasis. Computed
tomography revealed that the cervical lymphonodule was enlarged on
the left side, at levels III and IV (Fig. 1). The chest X-ray was normal and
other extrapulmonary TBs were excluded.
A total thyroidectomy and selective neck dissection
(left side, levels III, IV and VI) were performed. The lobes were
opened and certain areas appeared to be colloid-rich and necrotic.
A hard, whitish lesion 6 mm in diameter, which was not clearly
separated from the normal tissue, was identified in the left lobe.
The extracted lymph nodes were soft, oval and 10 mm in diameter.
The intraoperative histological evaluation revealed thyroiditis and
PTC. The final diagnosis was established by definitive
histopathological examination. The histopathological examination of
the dissected cervical lymph nodes showed the presence of TB, but
no metastasis. Following surgery, a tuberculin skin test (PPD test)
showed strong positivity. The final diagnosis was of PTC with
thyroid TB (Fig. 1) and tuberculous
lymphadenitis. There were no post-operative complications. The
patient was treated with isoniazid, rifampicin and ethambutol for
six months, prior to a permanent substitution with L-thyroxin (100
μg per day). During the subsequent regular follow-up examinations
there were no signs of disease recurrence.
Discussion
Thyroid gland TB is a rare disease with a frequency
of 0.1–0.4% in histologically diagnosed thyroid specimens (10). In Asian countries, such as India and
Turkey, where the prevalence of TB is high, the incidence of
thyroid gland TB remains low (0.6–1.15%) (11,12).
Thyroid TB is difficult to diagnose in the clinic due to a lack of
specific signs and symptoms. Thyroid TB may present itself as an
isolated nodule, diffuse legion or multinodular goiter, and even as
an abscess or chronic skin sinus (10). Imaging techniques are not very
useful in forming a diagnosis (13). FNAC with acid-fast bacilli is
considered the best method for the diagnosis of TB pre-operatively
(14). However, the majority of
thyroid TB cases are diagnosed based solely on the post-operative
histopathological examination. In the present case, the
identification of TB in cervical lymphadenopathy and a strongly
positive PPD test supported the diagnosis of TB. The final
diagnosis was established by the definitive histopathological
examination of a resected specimen
In the present case, hypothyroidism was observed,
which is uncommon for thyroid TB or PTC. This observation may have
been associated with the long disease history (16 years) of the
thyroid TB, where fibrotic tissue may have replaced normal thyroid
follicles. A previous study suggested the use of antituberculous
agents combined with surgical removal of the affected area of the
thyroid gland or surgical drainage to treat thyroid TB (15). A total thyroidectomy was not
indicated due to consequent hypothyroidism. In the present case, a
total thyroidectomy was performed due to the coexistence of
PTC.
Generally, the appropriate microenvironment for
malignant development may be created by chronic inflammatory
conditions using numerous mechanisms (16). Mycobacterial infections establish
chronic and persistent inflammation. Previous studies have reported
that mycobacterial cell wall components are capable of inducing DNA
damage through the production of nitric oxide and reactive oxygen
species (17). This DNA damage has
been implicated in inflammation-related carcinogenesis (18). Mycobacterium tuberculosis has
also been found to induce antiapoptotic activity through the
upregulation of B-cell lymphoma 2 gene expression (19). Moreover, certain clinical and
experimental studies have observed elevated concentrations of
prostaglandins following mycobacterial infection (20). The combination of direct DNA damage,
apoptosis inhibition and chronic inflammation may result in a
microenvironment that is highly favorable for tumorigenesis
(17). In the present case, the
histopathological findings revealed typical inflammatory
characteristics of thyroid TB. Thus, the development of PTC may be
associated with TB infection. Furthermore, the high TSH levels
caused by disruption of the thyroid tissue promoted tumor cell
growth. In addition, the presence of TB lymphadenitis may result in
overstaging when using the tumor-node-metastasis system.
Pre-operative lymphatic puncture effectively prevents overstaging
and excessive surgery.
In conclusion, this study reported a rare case of
coexisting PTC and thyroid TB, and implicated the possible role of
mycobacterial infections in the tumorigenesis of PTC.
References
|
1
|
World Health Organization. 2012, Global
Tuberculosis Report 2012. http://www.who.int/tb/publications/global_report/gtbr12_main.pdf.
Accessed October 17, 2012
|
|
2
|
Akbulut S, Sogutcu N and Yagmur Y:
Coexistence of breast cancer and tuberculosis in axillary lymph
nodes: a case report and literature review. Breast Cancer Res
Treat. 130:1037–1042. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
World Health Organization. Global Health
Observatory: Cancer mortality and morbidity. http://www.who.int/gho/ncd/mortality_morbidity/cancer/en/index.html.
Accessed January 12, 2013
|
|
4
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J and
Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 59:225–249.
2009. View Article : Google Scholar
|
|
5
|
Sonkar AA, Rajamanickam S and Singh D:
Papillary thyroid carcinoma: debate at rest. Indian J Cancer.
47:206–216. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cömert FB, Cömert M, Külah C, Taşcilar O,
Numanoğlu G and Aydemir S: Colonic tuberculosis mimicking tumor
perforation: a case report and review of the literature. Dig Dis
Sci. 51:1039–1042. 2006.PubMed/NCBI
|
|
7
|
el Kohen A, Essakalli L, Amarti A,
Benchekroun L, Jazouli N and Kzadri M: Thyroid tuberculosis
associated with papillary microcarcinoma of the thyroid gland: a
case report. Rev Laryngol Otol Rhinol (Bord). 122:205–208. 2001.(In
French).
|
|
8
|
Hizawa K, Okamura K, Sato K, Kuroda T,
Yoshinari M, Ikenoue H and Fujishima M: Tuberculous thyroiditis and
miliary tuberculosis manifested postpartum in a patient with
thyroid carcinoma. Endocrinol Jpn. 37:571–576. 1990. View Article : Google Scholar
|
|
9
|
Suri VS, Sakhuja P, Malhotra V, Gondal R,
Singh S and Sidhu N: Co-existent tuberculosis and papillary
carcinoma thyroid. Trop Doct. 32:1182002.PubMed/NCBI
|
|
10
|
Bulbuloglu E, Ciralik H, Okur E, Ozdemir
G, Ezberci F and Cetinkaya A: Tuberculosis of the thyroid gland:
review of the literature. World J Surg. 30:149–155. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ghosh A, Saha S, Bhattacharya B and
Chattopadhay S: Primary tuberculosis of thyroid gland: a rare case
report. Am J Otolaryngol. 28:267–270. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Akbulut S, Sogutcu N, Arikanoglu Z, Bakir
S, Ulku A and Yagmur Y: Thyroid tuberculosis in southeastern
Turkey: is this the resurgence of a stubborn disease? World J Surg.
35:1847–1852. 2011. View Article : Google Scholar
|
|
13
|
Kang M, Ojili V, Khandelwal N and Bhansali
A: Tuberculous abscess of the thyroid gland: a report of two cases.
J Clin Ultrasound. 34:254–257. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Goel MM and Budhwar P: Fine needle
aspiration cytology and immunocytochemistry in tuberculous
thyroiditis: a case report. Acta Cytol. 52:602–606. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Majid U and Islam N: Thyroid tuberculosis:
a case series and a review of the literature. J Thyroid Res.
2011:3598642011. View Article : Google Scholar
|
|
16
|
Schottenfeld D and Beebe-Dimmer J: Chronic
inflammation: a common and important factor in the pathogenesis of
neoplasia. CA Cancer J Clin. 56:69–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Falagas ME, Kouranos VD, Athanassa Z and
Kopterides P: Tuberculosis and malignancy. QJM. 103:461–487. 2010.
View Article : Google Scholar
|
|
18
|
Kawanishi S, Hiraku Y, Pinlaor S and Ma N:
Oxidative and nitrative DNA damage in animals and patients with
inflammatory diseases in relation to inflammation-related
carcinogenesis. Biol Chem. 387:365–372. 2006. View Article : Google Scholar
|
|
19
|
Zhang J, Jiang R, Takayama H and Tanaka Y:
Survival of virulent Mycobacterium tuberculosis involves
preventing apoptosis induced by Bcl-2 upregulation and release
resulting from necrosis in J774 macrophages. Microbiol Immunol.
49:845–852. 2005.
|
|
20
|
Rangel Moreno J, Estrada García I, De La
Luz García Hernández M, Aguilar Leon D, Marquez R and Hernández
Pando R: The role of prostaglandin E2 in the immunopathogenesis of
experimental pulmonary tuberculosis. Immunology. 106:257–266.
2002.PubMed/NCBI
|