Introduction
Carbohydrate antigen 19-9 (CA19-9) is a sialyl Lewis
A antigen and is widely used as a tumor marker for cancers of the
biliary, pancreatic and gastrointestinal tracts (1–3).
However, in benign diseases, such as pancreatitis, liver cirrhosis,
biliary diseases and diabetes mellitus, serum CA19-9 levels may
exhibit a marginal increase (4–7). The
current study presents a case of intralobar pulmonary
sequestration, which led to upper left abdominal bloating and
marked elevation of serum CA19-9 levels. The patient was previously
diagnosed with suspected gastrointestinal cancer. This study was
approved by the Ethics Committee of Tongji Hospital (Wuhan, China).
Witten informed consent was obtained from the patient.
Case report
A 48-year-old male was admitted to the Tongji
Hospital (Wuhan, China) presenting with upper left abdominal
bloating and marked elevation of serum CA19-9 levels. The bloating
was persistent with no improvement following corresponding
treatment for two months. The patient had an acute cough and pain
of the left chest one month prior to admission. The laboratory
examination results were normal with the exception of the marked
elevation of serum CA19-9 levels (790.6 U/ml). The patient was
administered with two weeks of antibiotic treatment and the
clinical symptoms evidently improved, however, the serum CA19-9
levels remained high (703.3 U/ml). The patient’s doctor suspected
hepato-biliary-pancreatic disease and the individual was referred
to the Tongji Hospital to determine the cause of the elevated serum
CA19-9 levels.
The patient was a non-smoker and had no family
history of pulmonary tuberculosis (TB) or bronchiectasis. However,
the patient had pneumonia in 2009, which was cured following
antibiotic treatment. The physical examination showed no
abnormalities and the laboratory examination revealed a marginal
increase in serum γ-guanosine triphosphate (80 IU/l) and serum
CA19-9 levels increased to 1,242.85 U/ml. To exclude the
possibility of an underlying abnormal malignant lesion,
esophagogastroduodenoscopy, endoscopic ultrasonography,
colonoscopy, abdominal ultrasonography and computed tomography (CT)
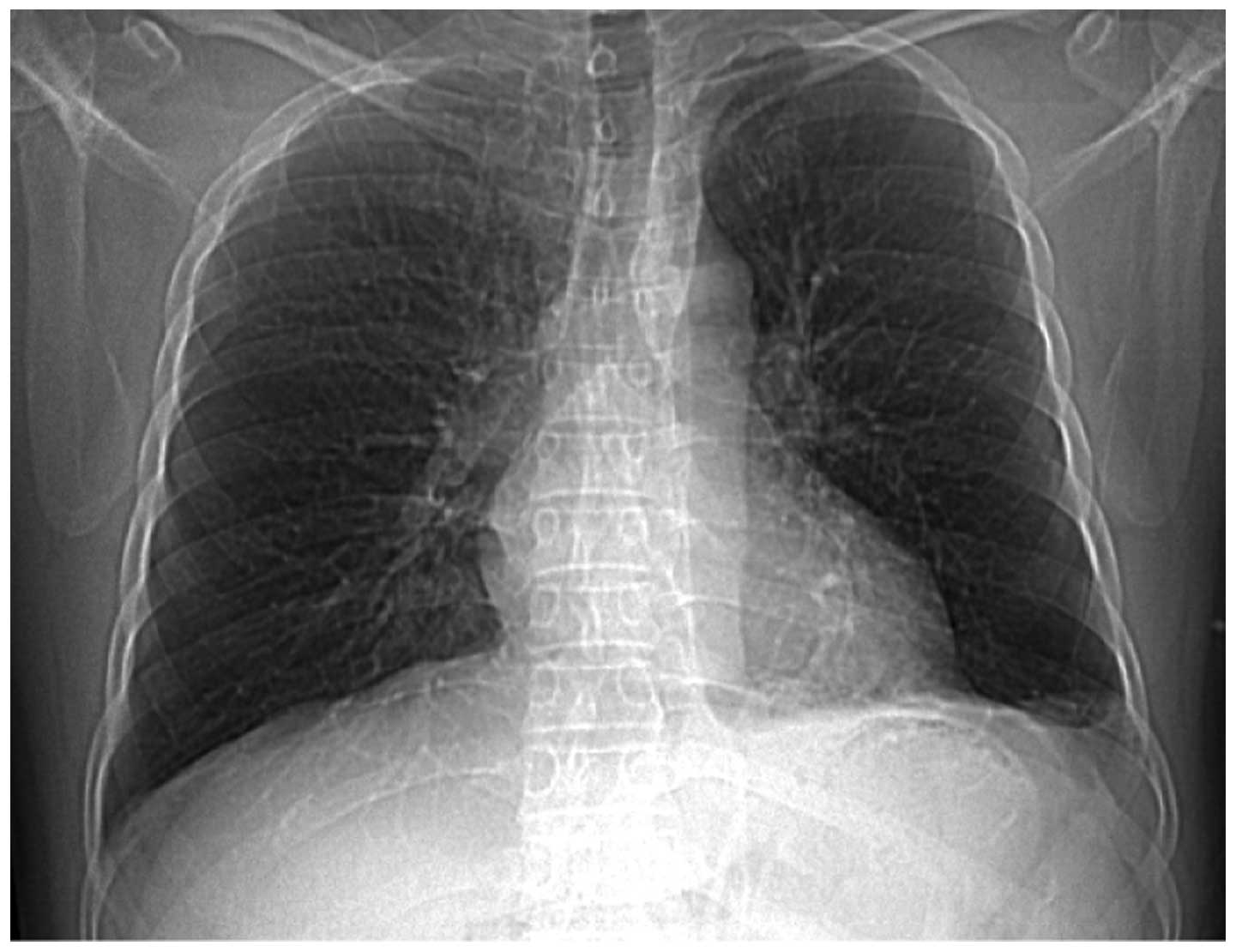
were performed with no specific abnormalities identified. A chest
X-ray that was performed on admission of the patient to hospital
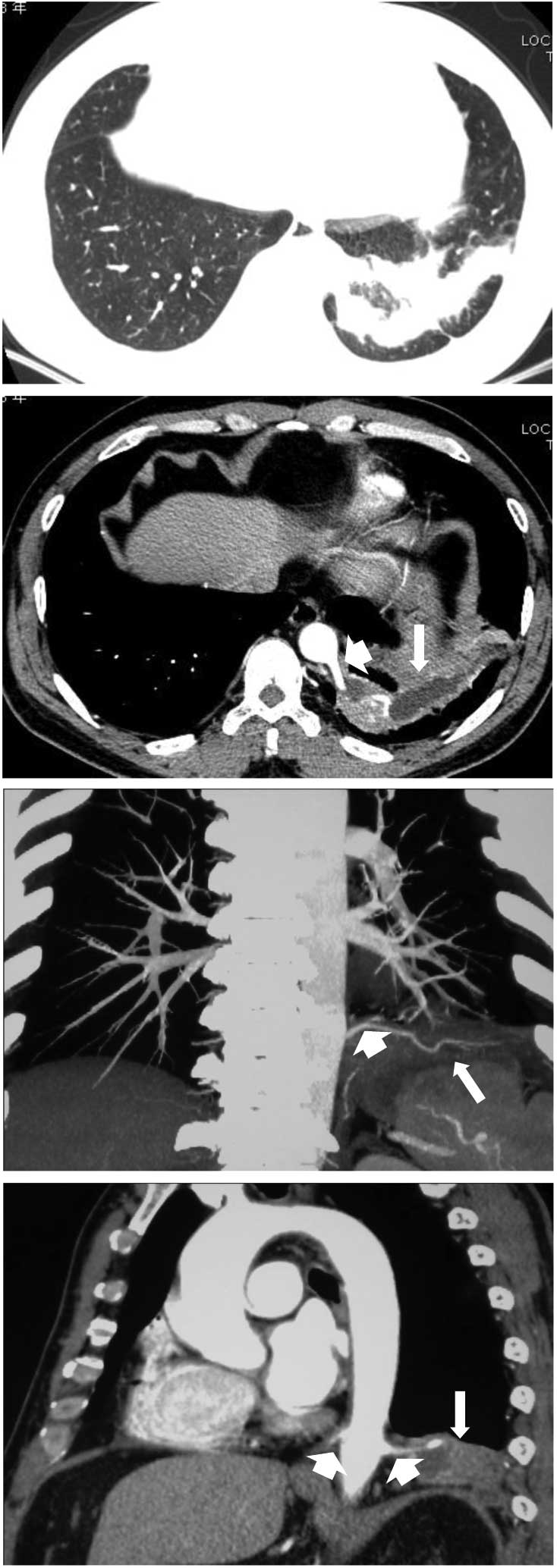
showed a dense shadow cord strip in the left lower region (Fig. 1). In addition, chest high-resolution
CT scanning and 3D image reconstruction further indicated anomalous
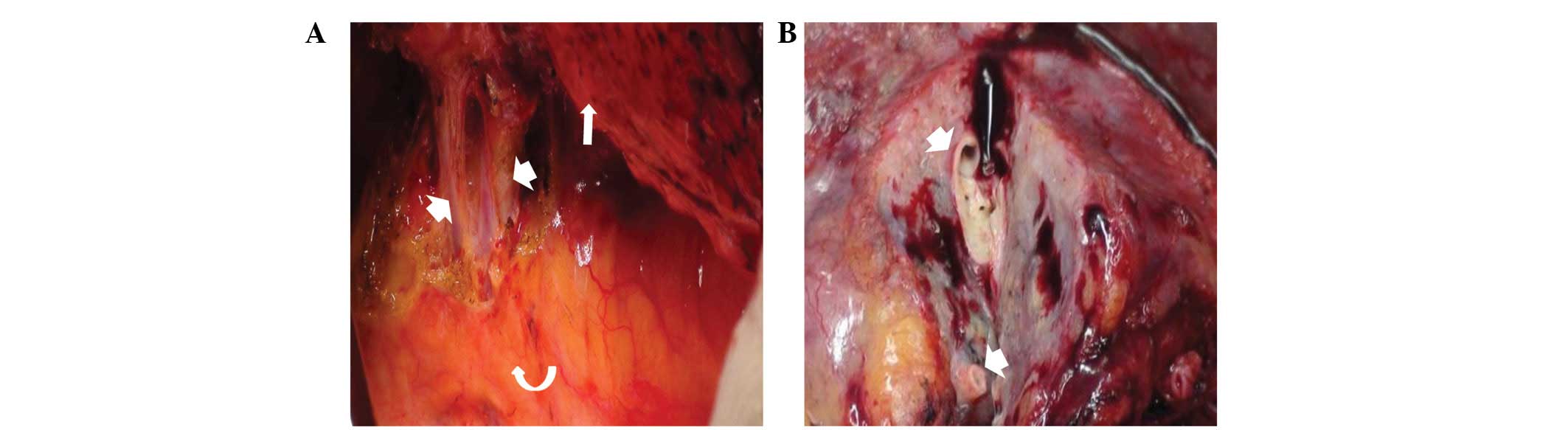
arteries arising from the descending thoracic aorta (Fig. 2). Pulmonary sequestration was
diagnosed, and surgery confirmed the presence of two aberrant
arteries arising from the thoracic aorta and entering the left
lower lobe basal segment. The sequestrated lung was consolidated
and tightly connected to the diaphragm (Fig. 3). A left lower lobectomy was
performed and the postoperative pathological observations were
consistent with intralobar pulmonary sequestration.
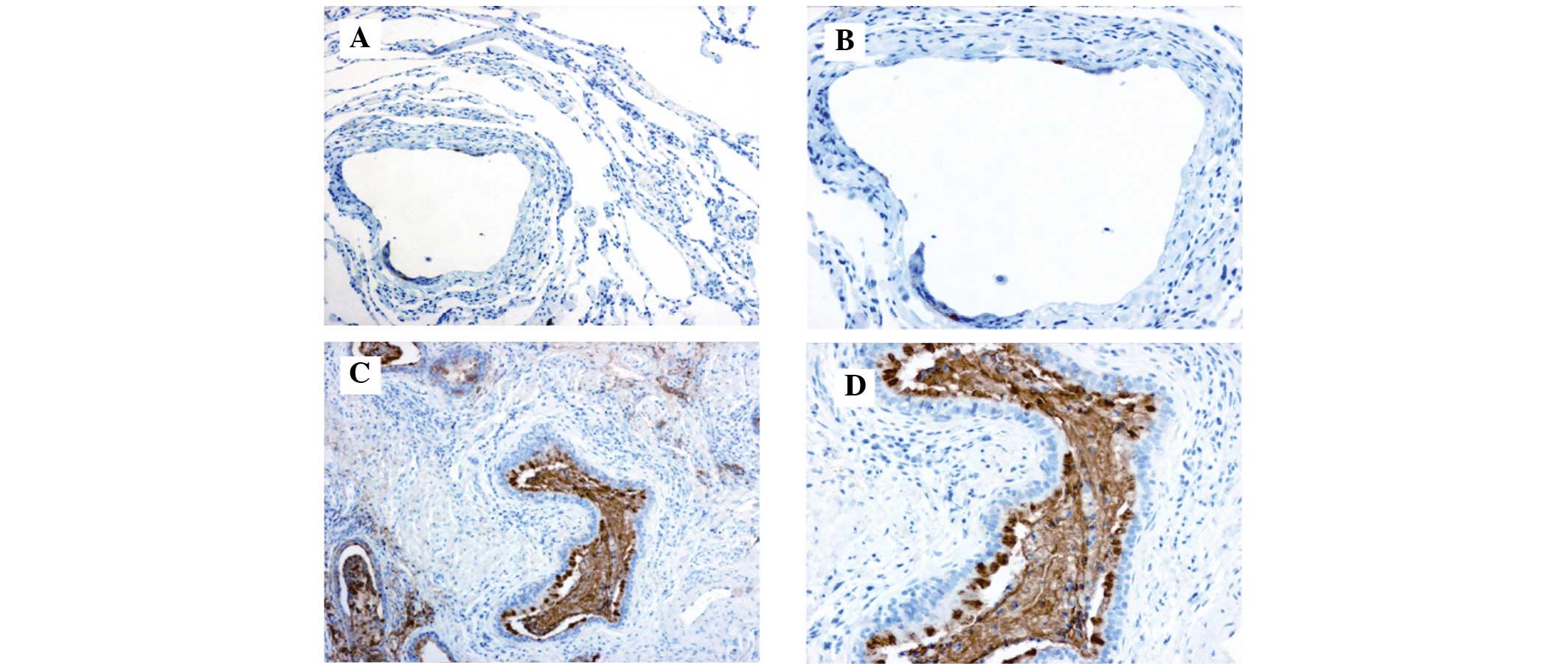
Immunohistochemistry staining using a monoclonal antibody against
human CA19-9 (Maixin Biotechnology, Fuzhou, China) demonstrated
marked positive staining for CA19-9 in the ciliated cylindrical
epithelia, alveoli and particularly in the mucus of the cysts
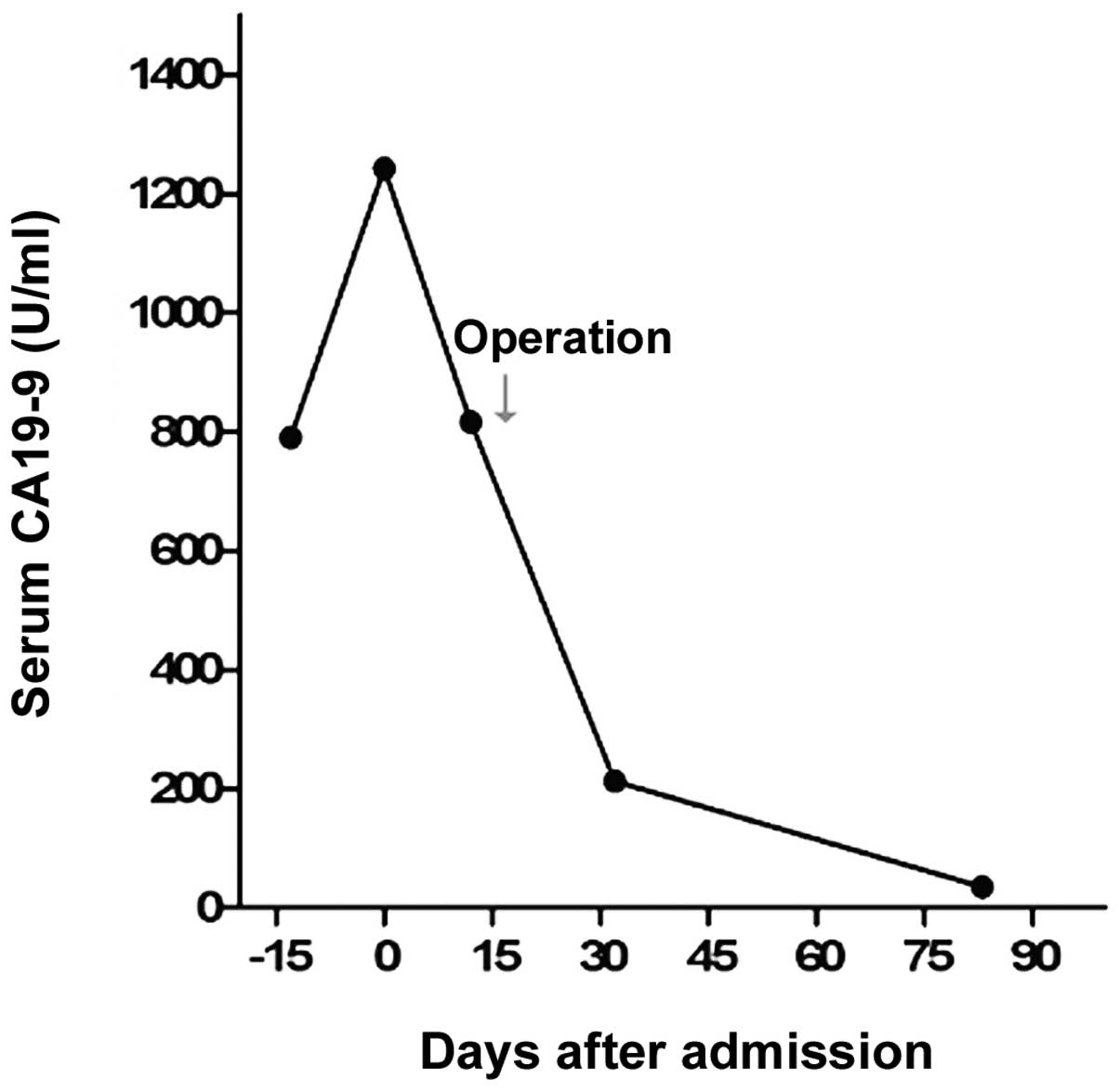
(Fig. 4). Following pulmonary
resection, the symptom of bloating improved and the serum CA19-9
levels rapidly decreased to within the normal range (34.5 U/ml;
Fig. 5).
Discussion
CA 19-9 is valuable as a serum marker for cancers of
the biliary, pancreatic and gastrointestinal tracts. However,
elevation of serum CA19-9 levels may also occur in the following
benign conditions: i) Increased CA19-9 production due to
inflammation or proliferation of non-cancerous tissues, such as
pancreatitis, pancreatic cysts, cholangitis, bronchial cysts,
bronchiectasis and ovarian cysts; ii) CA19-9 discharge pathway
obstruction caused by pancreatic or cholangial duct stenosis due to
gall stones and papillitis; and iii) malfunction in CA19-9
metabolism, such as chronic hepatitis, chronic glomerulonephritis
and diabetes mellitus (8). In the
current study, the patient presented with upper left abdominal
bloating and marked elevation of serum CA19-9 levels and was
diagnosed with intralobar pulmonary sequestration.
Immunohistochemistry demonstrated marked positive staining for
CA19-9 in the ciliated cylindrical epithelia, alveoli and
particularly in the mucus of the cysts. The serum CA19-9 levels
rapidly decreased to normal range following surgery. Furthermore,
in the present case, no malignant signs were identified in the
choledochal, pancreatic or gastrointestinal tracts. These results
indicated, in the present case, that CA19-9 was produced in the
sequestrated lung and released into the blood via an unknown
mechanism.
Pulmonary sequestration is a rare malformation
characterized by the presence of lung tissue with abnormal or
absent communication with the bronchi. Pulmonary sequestration is
classified into the following two types: Intralobar pulmonary
sequestration, in which the sequestered section of the lung lies
with the normal pulmonary visceral pleura; and extralobar pulmonary
sequestration, where the pulmonary tissue is surrounded by the
pleura of the lesion itself (9).
For the current study, 44 patients that were diagnosed with
pulmonary sequestration by surgery at the Tongji Hospital between
2003 and 2012 were reviewed (Table
I). There was an approximately equal distribution observed
between the genders, and five children and 39 adults were included.
The average age of the children that underwent surgery was five
years, ranging between two months and 10 years. Among the adult
population, the average age was 35 years, ranging between 13 and 59
years. The predominant clinical symptoms of pulmonary sequestration
were coughing (50%), fever (25%), hemoptysis (22.7%), expectoration
(18.2%), chest tightness (15.9%) and thoracic pain (11.4%).
Notably, nine patients were asymptomatic and the majority were
identified during a general check up. In total, 38 of the 44 cases
of sequestration were intralobar and the other six were extralobar.
Of the six patients with extralobar sequestrations, two patients
exhibited diaphragmatocele concurrently, however, intralobar
sequestrations were not found to be associated with other
diaphragmatic or cardiopulmonary anomalies. The sequestrated lung
predominantly appeared in the left (65.9%) and right (22.7%) lower
lobes; only two cases were identified in the right upper lobe and
three occurred in multiple lobes. Sequestrated lung is frequently
infected with various bacteria and occasionally it exhibits
secondary infection with uncommon pathogens, such as
Mycobacterium TB and fungus. Examination of the serum CA19-9
levels is seldom advised for suspected pulmonary sequestration
patients. Of the 44 patients, the serum CA19-9 levels were detected
by chance in three patients prior to surgery. One patient, out of
the three, was found to exhibit elevated serum CA19-9 levels (159.2
U/ml), which decreased to within the normal range following
surgery.
 | Table IAnalysis of 44 cases of pulmonary
sequestration surgical procedures at the Tongji Hospital between
2003 and 2012. |
Table I
Analysis of 44 cases of pulmonary
sequestration surgical procedures at the Tongji Hospital between
2003 and 2012.
| Clinical feature | n |
|---|
| Gender |
| Male | 24 |
| Female | 20 |
| Sequestration
type |
| Intralobar | 38 |
| Extralobar | 6 |
| Location |
| Single lobe | |
| Left lower lobe | 29 |
| Right lower
lobe | 10 |
| Right upper
lobe | 2 |
| Multiple lobes | 3 |
| Associated
diseases |
| Intralobar | 0 |
| Extralobar
(diaphragmatocele) | 2 |
| Serum CA19-9
level |
| Elevation | 1 |
| Normal | 2 |
| Not detected | 41 |
| Secondary
infection |
| Mycobacterium
tuberculosis | 1 |
| Fungal | 4 |
| Symptom |
| Cough | 22 |
| Fever | 11 |
| Hemoptysis | 10 |
| Expectoration | 8 |
| Chest tightness | 7 |
| Thoracic pain | 5 |
| Wheezing | 1 |
| Anhelation | 1 |
| Abdominal
distension | 1 |
| Asymptomatic | 9 |
To the best of our knowledge, the current study is
the first report regarding the digestive symptom as well as
elevated serum CA19-9 levels caused by pulmonary sequestration.
Although comparable cases have been previously reported in Japan
and Korea (10–15), the exact mechanism of the condition
remains a controversial subject. Previously, Yagyu et al
(16) inferred that CA19-9 may be
synthesized and secreted by normal bronchial epithelial cells, and
gradually accumulates in the sequestrated lung with no congestion
in the normal bronchial tree. In the current case,
immunohistochemistry demonstrated weak staining of CA19-9 in the
normal bronchial epithelia, however, marked staining was identified
in the sequestrated lung tissue, particularly in the mucus of the
cysts. In the present study, a cyst fluid culture was not performed
to exclude possible pathogens; however, the results were generally
consistent with the viewpoint of Ambiru et al (12) that CA19-9, which is concentrated in
the sequestrated lung, may transfer into the blood through the
injured mucosa of the cyst walls. Furthermore, we predict that the
diaphragm, stimulated by the consolidated lung, may lead to the
left upper abdominal bloating.
In conclusion, as patients that are diagnosed with
pulmonary sequestration may also show normal serum CA19-9 levels
(Table I), further basic studies
regarding the mechanism of CA19-9 increase in pulmonary
sequestration are required. Detecting the level of serum CA19-9 in
patients that are diagnosed with pulmonary sequestration may be
useful to investigate the correlation between, and mechanism of,
serum CA19-9 levels and pulmonary sequestration. In addition, to
avoid potential diagnostic pitfalls, it is important for digestive
physicians to be aware of the respiratory diseases that are
associated with elevated serum CA19-9 levels.
Acknowledgements
The present study was supported by the
Cardiothoracic Surgery Department and Department of Thoracic
Surgery at the Tongji Hospital (Wuhan, China).
References
|
1
|
Herlyn M, Sears HF, Steplewski Z and
Koprowski H: Monoclonal antibody detection of a circulating
tumor-associated antigen. I Presence of antigen in sera of patients
with colorectal, gastric, and pancreatic carcinoma. J Clin Immunol.
2:135–140. 1982. View Article : Google Scholar
|
|
2
|
Duffy MJ: CA 19-9 as a marker for
gastrointestinal cancers: a review. Ann Clin Biochem. 35:364–370.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
He CZ, Zhang KH, Li Q, Liu XH, Hong Y and
Lv NH: Combined use of AFP, CEA, CA125 and CA19-9 improves the
sensitivity for the diagnosis of gastric cancer. BMC Gastroenterol.
13:872013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Encabo G and Ruibal A: Seric CA 19.9
levels in patients with non tumoral pathologies. Our experience in
892 cases. Bull Cancer. 73:256–259. 1986.
|
|
5
|
Sawabu N, Takemori Y, Toya D, et al:
Factors affecting serum levels of CA 19-9 with special reference to
benign hepatobiliary and pancreatic diseases. Gastroenterol Jpn.
21:491–498. 1986.PubMed/NCBI
|
|
6
|
Leandro G, Zizzari S and Manghisi OG: Role
of hepatic dysfunction and bilirubin on CA 19-9 levels in cirrhotic
patients. Gastroenterology. 92:270–271. 1987.PubMed/NCBI
|
|
7
|
Nakamura N, Aoji O, Yoshikawa T, et al:
Elevated serum CA19-9 levels in poorly controlled diabetic
patients. Jpn J Med. 25:278–280. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ito S and Gejyo F: Elevation of serum
CA19-9 levels in benign diseases. Intern Med. 38:840–841. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mathew S and Erozan YS: Pulmonary
sequestration - a diagnostic pitfall: a case report. Diagn
Cytopathol. 16:353–357. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shiota Y, Kitade M, Furuya K and Ueda N: A
case of intralobar pulmonary sequestration with high serum CA19-9
levels. Acta Med Okayama. 42:297–300. 1988.PubMed/NCBI
|
|
11
|
Ahn YH, Song MJ and Park SH: Intralobar
pulmonary sequestration showing increased serum CA19-9. Tuberc
Respir Dis (Seoul). 72:507–510. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ambiru S, Nakamura S, Fukasawa M, Mishima
O, Kuwahara T and Takeshi A: Intralobar pulmonary sequestration
associated with marked elevation of serum carbohydrate antigen
19-9. Ann Thorac Surg. 88:2010–2011. 2009. View Article : Google Scholar
|
|
13
|
Ishii H, Mukae H, Ihiboshi H, et al:
Pulmonary sequestration associated with high levels of tumor
markers in serum. Nihon Kyobu Shikkan Gakkai Zasshi. 35:1029–1033.
1997.(In Japanese).
|
|
14
|
Kugai T and Kinjyo M: Extralobar
sequestration presenting increased serum CA19-9 and associated with
lung aspergillosis - an unusual case. Nihon Kyobu Geka Gakkai
Zasshi. 44:565–569. 1996.(In Japanese).
|
|
15
|
Nakamura H, Katsumi T, Nagata S, Saito M,
Konaka C and Kato H: A resected case of intralobar pulmonary
sequestration with increased serum tumor markers, CA19-9, CA125 and
NCC-ST-439. Nihon Kyobu Shikkan Gakkai Zasshi. 35:1425–1429.
1997.
|
|
16
|
Yagyu H, Adachi H, Furukawa K, et al:
Intralobar pulmonary sequestration presenting increased serum
CA19-9 and CA125. Intern Med. 41:875–878. 2002. View Article : Google Scholar : PubMed/NCBI
|