Introduction
Bronchogenic cysts are foregut-derived congenital
abnormalities that occur following the third week of embryonic life
(1). When attached to the primitive
foregut, the cyst is usually associated with the tracheobronchial
tree. However, in rare instances, the cyst may separate from the
normal airways, presumably by migration, and thus, may be found in
atypical locations, including the neck, intraspinal locations and
below the diaphragm (2).
Bronchogenic cysts presenting in the abdomen or retroperitoneum
have rarely been reported in the medical literature. Furthermore,
as bronchogenic cysts are usually asymptomatic, unless they become
secondarily infected or enlarge enough to compress adjacent organs,
the majority of reported cases are diagnosed incidentally (3,4). The
current study presents the case of a bronchogenic cyst in the
retroperitoneum of a 30-year-old female, which was successfully
managed by retroperitoneal laparoscopic surgery. In addition, the
clinical, radiographic, surgical and pathological observations are
summarized. Patient provided written informed consent.
Case report
A 30-year-old female was referred to the First
Hospital of Jilin University (Changchun, China) for the evaluation
of a left adrenal mass, which was identified incidentally during an
examination for a persistent fever, associated with coughing and
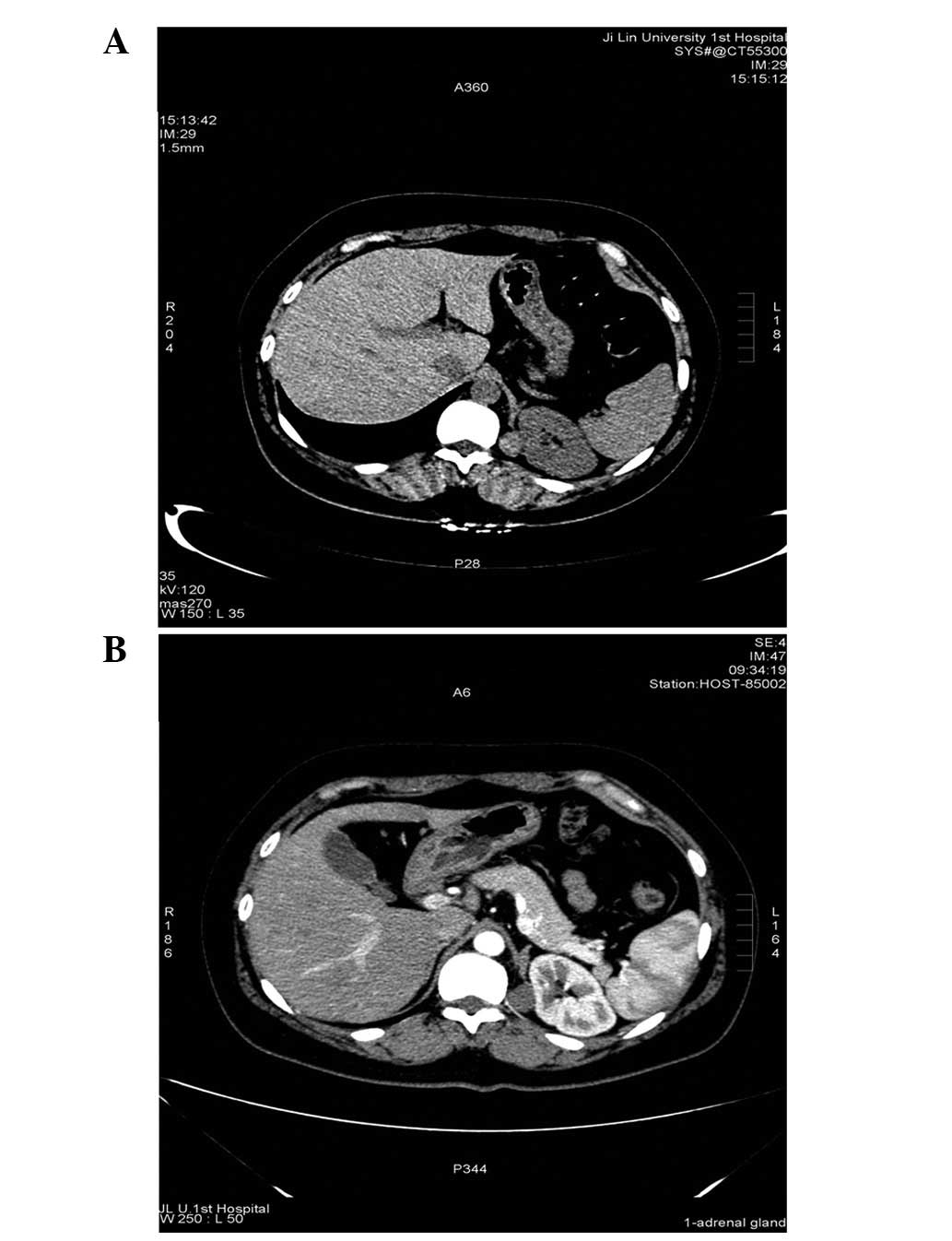
expectoration lasting for three days. A computed tomography (CT)
scan of the abdomen revealed a cystic mass measuring 32 Hounsfield
units, with a diameter of ~1.9 cm, located medially to the left
adrenal gland. However, the cystic mass was not clearly demarcated
from the upper pole of the left kidney (Fig. 1A). An enhanced CT scan revealed a
homogeneous, round, low-density mass with smooth outlines situated
in the retroperitoneum and slight enhancement (Fig. 1B).
The patient had no palpitations, diaphoresis,
weakness or hypertension. In addition, no other significant medical
history was noted. The patient’s endocrine evaluation results for
adrenal hypersecretion were negative, and the results of testing
for the renin ratio, aldosterone, plasma and urinary catecholamines
and metanephrines were all within the normal ranges. The patient
was admitted for surgical removal of the mass, and the laparoscopic
surgery revealed a 1.5×2.0×2.0-cm cystic structure with a complete
capsule, which was adherent to the upper pole of the left kidney.
The cyst was located deep within the retroperitoneum in the
immediate vicinity of the medial margin of the adrenal gland and
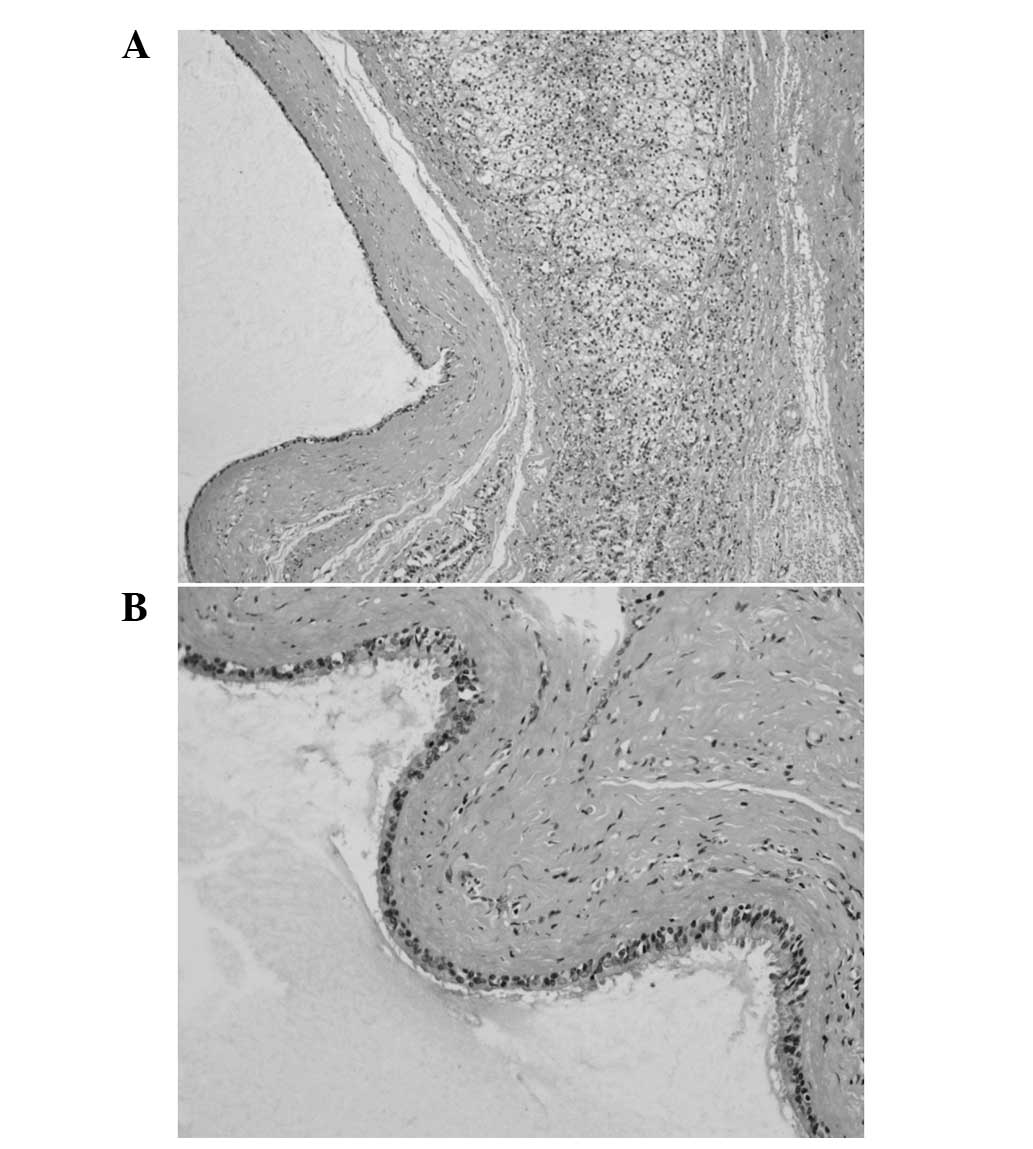
adjacent tissue. The pathological evaluation revealed a cystic mass
filled with a white seromucinous fluid. In addition, the
histopathological examination revealed that the cyst was partially
lined with ciliated pseudostratified epithelium, with the cyst wall
containing a small number of seromucous glands (Fig. 2).
The patient had an uneventful post-operative
recovery and was discharged on the fourth post-operative day. The
patient received no further treatment, however, regular follow-up
was performed due to the lesion being benign.
Discussion
When the tracheobronchial tree undergoes abnormal
budding and pinching off at approximately week five of gestation,
bronchogenic cysts develop (1). If
the connection with the tracheobronchial tree is lost, the foregut
and its derivatives that are usually in close proximity to the
trachea and bronchus may migrate to an atypical location (5). Retroperitoneally-located bronchogenic
cysts may occur as the pericardioperitoneal canal links the
thoracic and abdominal cavities (6).
Although bronchogenic cysts are rare, such cysts
must be considered in the diagnosis of a retroperitoneal mass.
However, the pre-operative diagnosis remains a clinical issue.
Retroperitoneal bronchogenic cysts may easily be misdiagnosed as
adrenal cortical or medullary tumors, or enteric, urothelial or
pancreatic cysts by their clinical and radiological presentation.
However, a histological diagnosis may differentially determine a
bronchogenic cyst from such lesions. Microscopically, bronchogenic
cysts are predominantly unilocular or oligolocular, lined by
pseudostratified ciliated columnar epithelium with bronchial
glands, mucoid material, cartilage and smooth muscle (7,8). In
the present study, the patient was diagnosed with a bronchogenic
cyst based on the presentation of the following histological
features: A ciliated pseudostratified epithelium and a small number
of seromucous glands.
The mainstay of treatment for retroperitoneal
bronchogenic cysts is surgical removal. Although the majority of
cysts are asymptomatic and exhibit benign behavior, excision is
recommended to establish a diagnosis, to alleviate any symptoms and
to prevent infection and the documented risk of malignant
transformation (9). According to
the literature, laparoscopic excision has been widely used to treat
retroperitoneal bronchogenic cysts (10,11).
Furthermore, as this approach uses small incisions, it has the
potential to decrease the duration of hospitalization and
therefore, reduce costs to the hospital and patient.
In conclusion, the current study presents a rare
case of a retroperitoneally localized bronchogenic cyst as an
unusual differential diagnosis of a retroperitoneal tumor. The
combination of clinical, biochemical and radiological features may
aid in the characterization of lesions, however, only a
histological analysis can currently provide a definite
diagnosis.
References
|
1
|
Buckley JA, Siegelman ES, Birnbaum BA and
Rosato EF: Bronchogenic cyst appearing as a retroperitoneal mass.
AJR Am J Roentgenol. 171:527–528. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
McAdams HP, Kirejczyk WM,
Rosado-de-Christenson ML and Matsumoto S: Bronchogenic cyst:
imaging features with clinical and histopathologic correlation.
Radiology. 217:441–446. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Murakami R, Machida M, Kobayashi Y, et al:
Retroperitoneal bronchogenic cyst: CT and MR imaging. Abdom
Imaging. 25:444–447. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Doggett RS, Carty SE and Clarke MR:
Retroperitoneal bronchogenic cyst masquerading clinically and
radiologically as a phaeochromocytoma. Virchows Arch. 431:73–76.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sumiyoshi K, Shimizu S, Enjoji M, et al:
Bronchogenic cyst in the abdomen. Virchows Arch A Pathol Anat
Histopathol. 408:93–98. 1985. View Article : Google Scholar
|
|
6
|
Reichelt O, Grieser T, Wunderlich H, et
al: Bronchogenic cyst. A rare differential diagnosis of
retroperitoneal tumors. Urol Int. 64:216–219. 2000.PubMed/NCBI
|
|
7
|
Martín R, Sanz E, de Vicente E, et al:
Differential diagnosis of asymptomatic retroperitoneal cystic
lesion: a new case of retroperitoneal bronchogenic cyst. Eur
Radiol. 12:949–950. 2002.PubMed/NCBI
|
|
8
|
Itoh H, Shitamura T, Kataoka H, et al:
Retroperitoneal bronchogenic cyst: report of a case and literature
review. Pathol Int. 49:152–155. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sullivan SM, Okada S, Kudo M and Ebihara
Y: A retroperitoneal bronchogenic cyst with malignant change.
Pathol Int. 49:338–341. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Díaz Nieto R, Naranjo Torres A, Gómez
Alvarez M, et al: Intraabdominal bronchogenic cyst. J Gastrointest
Surg. 14:756–758. 2010.
|
|
11
|
El Youssef R, Fleseriu M and Sheppard BC:
Adrenal and pancreatic presentation of subdiaphragmatic
retroperitoneal bronchogenic cysts. Arch Surg. 145:302–304.
2010.PubMed/NCBI
|