Introduction
Thrombocytopenia is a common complication of liver
cirrhosis and is an intractable issue when performing invasive
procedures (1,2). When cirrhotic patients with severe
thrombocytopenia undergo elective invasive procedures for
hepatocellular carcinoma (HCC), ~60% of the patients require
treatment for thrombocytopenia, including platelet transfusions,
partial splenic embolization or splenectomy (2). However, platelet transfusions carry
the risk of anaphylactic shock, infection and transfusion-related
acute lung injuries. Partial splenic embolization may lead to
splenic abscesses. In addition, splenectomy may result in splenic
vein thrombosis and overwhelming post-splenectomy infections. Thus,
a non-invasive therapeutic strategy for thrombocytopenia is
required for cirrhotic patients with HCC.
Eltrombopag is an oral thrombopoietin (TPO)-receptor
(R) agonist that stimulates megakaryocytes and thus, increases
platelet counts in patients with idiopathic thrombocytopenic
purpura (3). Since decreased plasma
levels of TPO, in addition to hypersplenism, are major pathogenic
features of cirrhosis-related thrombocytopenia (1), eltrombopag appears to improve
thrombocytopenia in cirrhotic patients. Furthermore, eltrombopag
has previously been reported to increase platelet counts and thus,
enables subsequent interferon treatments and invasive procedures in
cirrhotic patients with severe thrombocytopenia (4–6).
TPO is known as a megakaryocyte growth and
development factor that leads to megakaryocyte proliferation. In
addition, TPO induces the proliferation of various cell types that
express the TPO-R. In the liver, the TPO-R occurs in hepatic
progenitor cells (7) and hepatic
sinusoidal endothelial cells (8).
In addition, TPO induces the proliferation of these two cell types
(7,8). Since hepatic sinusoidal endothelial
cells and hepatic progenitor cells are crucial in the development
and progression of HCC, the effect of eltrombopag on the
proliferation of HCC is significant.
The current report presents two cases of HCC with
cirrhosis-related thrombocytopenia. In these two cases, eltrombopag
treatment increased platelet counts without any concomitant changes
in the serum levels of tumor markers or HCC size. The HCCs were
subsequently treated by curative radiofrequency ablation (RFA)
without platelet transfusions or serious bleeding. Patient provided
writted informed consent.
Case report
Case 1
In 2008, a 65-year-old male patient was referred to
the Kurume University Hospital (Kurume, Japan) for the treatment of
hepatitis C virus (HCV)-related liver cirrhosis. The patient had a
history of esophageal varices rupture (that occurred in 1993) and
HCC, which was treated by transcatheter hepatic arterial
chemolipiodolization with embolization in 2007.
The patient was treated with ursodeoxycholic acid,
glycyrrhizin and nutritional therapy, including branched-chain
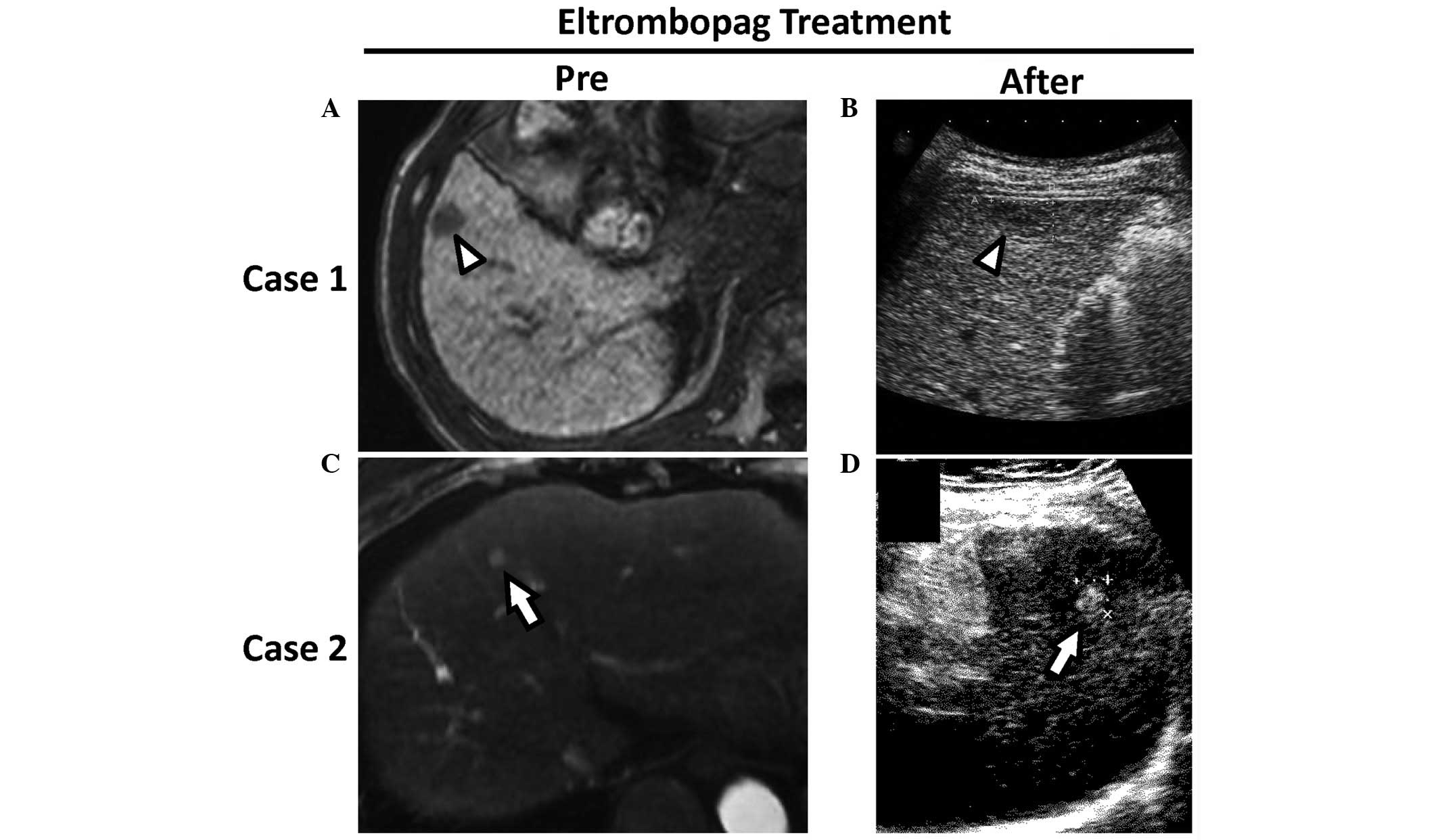
amino acid granules. However, in 2009, a regular abdominal
ultrasound revealed a hypoechoic lesion with a maximum diameter of
~15 mm in Couinaud segment 5 of the liver. The lesion showed
decreased contrast uptake in the hepatocyte phase as determined by
gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid
(EOB)-enhanced magnetic resonance imaging (MRI) scan (Fig. 1A). Additionally, an aspiration tumor
biopsy revealed that the lesion was a well-differentiated HCC. The
HCC was a single nodule and the patient’s Child-Pugh score was 7
points. Although RFA was selected as a therapeutic strategy for
HCC, the patient’s platelet count (4.8×104 /μl) revealed
severe thrombocytopenia.
The risks and benefits of participation in the phase
II study were explained to the patient (5); this study aimed to investigate the
efficacy and safety of eltrombopag in patients with
thrombocytopenia. Written informed consent was obtained and 25.0 mg
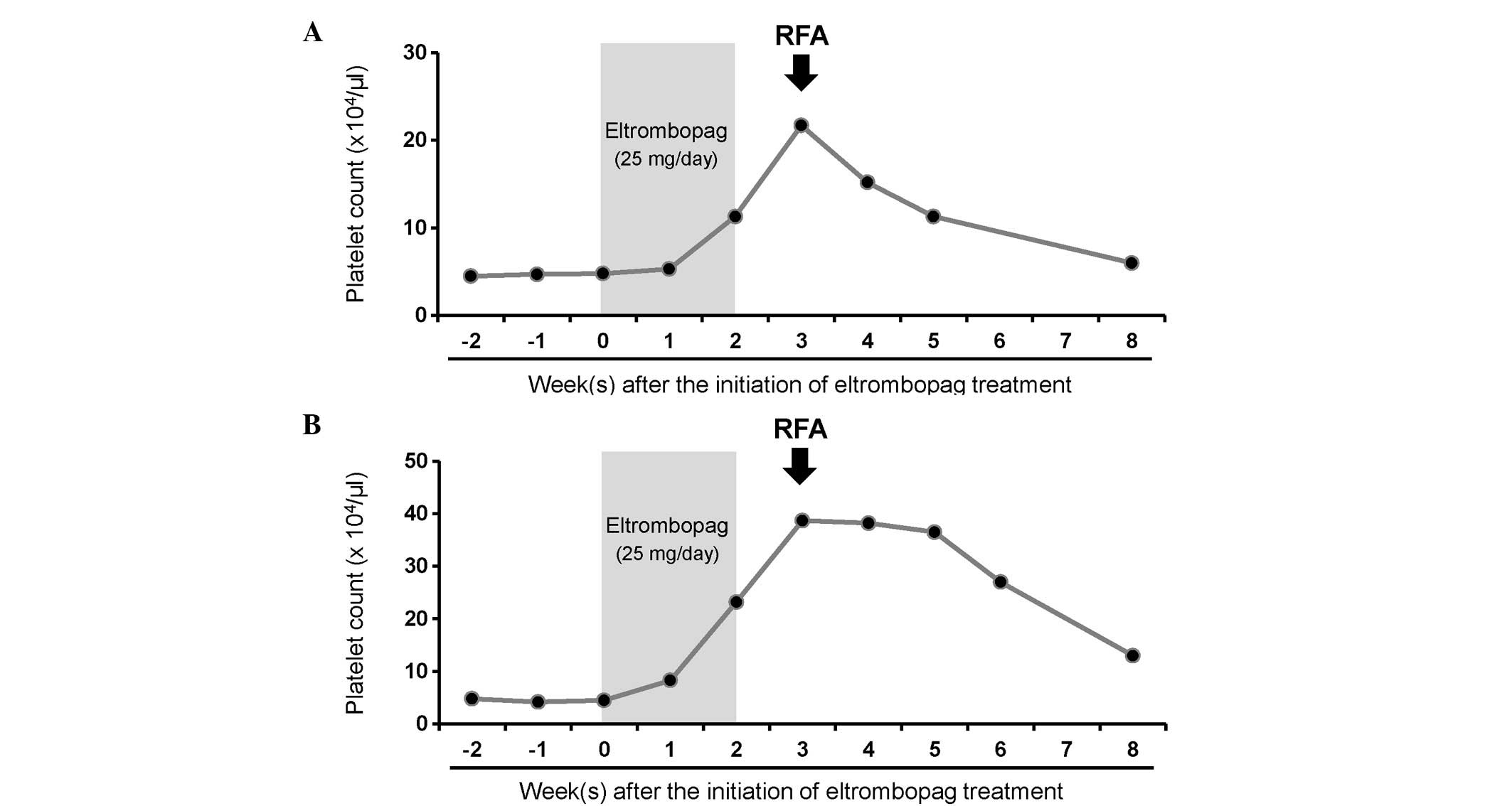
eltrombopag was subsequently administered to the patient. The
patient’s platelet count increased from 4.8 to 11.3×104
/μl during the administration of eltrombopag (Fig. 2A; gray area). Following the
termination of eltrombopag treatment, the platelet count continued
to increase to 21.7×104 /μl at three weeks since the
initiation of eltrombopag treatment. No significant changes were
observed in the serum levels of α-fetoprotein and des-γ-carboxy
prothrombin (Table I) or HCC size
(Fig. 1B). The HCC was curatively
treated by RFA without platelet transfusion or serious bleeding at
three weeks following initiation of the eltrombopag treatment.
 | Table IChanges in biochemical parameters
during the course of eltrombopag treatment. |
Table I
Changes in biochemical parameters
during the course of eltrombopag treatment.
| | Following eltrombopag
initiation |
|---|
| | Case 1 | Case 2 |
|---|
| |
|
|
|---|
| Biochemical
parameter | Reference value | Pre | Week 2 | Week 3 | Pre | Week 2 | Week 3 |
|---|
| Red blood cells,
×104/mm3 | 430–570 | 383 | 368 | 352 | 394 | 369 | 358 |
| Hemoglobin, g/dl | 14.0–18.0 | 12.5 | 11.7 | 11.5 | 13.1 | 12.3 | 12.1 |
| White blood cells,
/mm3 | 4000–9000 | 2200 | 2500 | 2600 | 3800 | 4200 | 5200 |
| Platelets,
×104/mm3 | 13–36 | 4.8 | 11.3 | 21.7 | 4.5 | 23.2 | 38.7 |
| Aspartate
transaminase, U/l | 13–33 | 102 | 67 | 60 | 46 | 35 | 36 |
| Alanine
aminotransferase, U/l | 8–42 | 96 | 64 | 49 | 35 | 24 | 22 |
| Lactate
dehydrogenase, U/l | 119–229 | 285 | 216 | 249 | 298 | 344 | 341 |
| Alkaline phosphatase,
U/l | 115–359 | 352 | 372 | 339 | 278 | 245 | 301 |
| γ-glutamyl
transpeptidase, U/l | 10–47 | 29 | 28 | 27 | 25 | 27 | 39 |
| Total protein,
g/dl | 6.70–8.30 | 8.09 | 7.74 | 7.59 | 7.71 | 7.17 | 7.34 |
| Albumin, g/dl | 4.00–5.00 | 2.83 | 2.69 | 2.59 | 3.23 | 2.91 | 2.87 |
| Total bilirubin,
mg/dl | 0.30–1.50 | 1.19 | 0.99 | 0.64 | 2.09 | 1.99 | 1.40 |
| Prothrombin activity,
% | 60–130 | 64 | 59 | 69 | 70 | 66 | 73 |
| Prothrombin activity,
INR | 0.87–1.25 | 1.32 | 1.40 | 1.27 | 1.25 | 1.29 | 1.22 |
| BUN, mg/dl | 8.0–22.0 | 22.6 | 21.5 | 25.4 | 15.0 | 15.3 | 20.2 |
| Creatinine,
mg/dl | 0.60–1.10 | 1.00 | 0.96 | 1.21 | 0.64 | 0.68 | 0.81 |
| Sodium, mEq/l | 138–146 | 137 | 136 | 136 | 139 | 138 | 134 |
| Child-Pugh score | | 7 | 7 | 7 | 8 | 8 | 7 |
| MELD score | | 10 | 10 | 11 | 12 | 12 | 10 |
| α-fetoprotein,
ng/ml | <8.7 | 23.0 | 21.8 | 26.2 | 27.8 | 30.5 | 23.9 |
| Des-γ-carboxy
prothrombin, mAU/ml | <40 | 16 | 14 | 20 | 45 | 35 | 30 |
Case 2
In 2005, a 61-year-old female patient was referred
to the Kurume University Hospital for the treatment of HCV-related
liver cirrhosis. The patient was treated with ursodeoxycholic acid
and glycyrrhizin. However, the hepatic fibrosis gradually
progressed. In 2009, a regular abdominal ultrasound revealed a
hyperechoic lesion with a maximum diameter of ~7 mm in Couinaud
segment 4 of the liver. An EOB-MRI scan revealed contrast
enhancement of the lesion during the early phase (Fig. 1C). The lesion was subsequently
diagnosed as a well-differentiated HCC via an aspiration tumor
biopsy. The HCC was a single nodule and the patient’s Child-Pugh
score was 8 points. RFA was selected as a therapeutic strategy for
the HCC, however, the patient’s platelet count decreased to
4.5×104 /μl.
The risks and benefits of participation in the phase
II study were explained as previously described (5). Written informed consent was obtained
and 25.0 mg eltrombopag was subsequently administered to the
patient. The platelet count increased from 4.5 to
23.2×104 /μl during eltrombopag treatment (Fig. 2B; gray area). Following the
termination of eltrombopag treatment, the platelet count increased
further to 38.7×104 /μl (three weeks since the
initiation of eltrombopag treatment). No significant changes were
observed in the serum levels of α-fetoprotein and des-γ-carboxy
prothrombin (Table I) or in the HCC
size (Fig. 1B). At three weeks
following the initiation of eltrombopag treatment, the HCC was
curatively treated by RFA without platelet transfusion or serious
bleeding.
Discussion
The effect of eltrombopag on the progression of
malignant neoplasms is an important issue. The current report
presents two cases of HCC with cirrhosis-related severe
thrombocytopenia. The administration of eltrombopag increased the
platelet count in these two cases without inducing significant
changes in the serum levels of tumor markers or HCC size. These
HCCs were successfully treated by RFA without platelet transfusions
or serious bleeding. The observations from these cases may indicate
that the short-term administration of eltrombopag does not affect
the progression of HCC and may be useful when administered prior to
invasive procedures in cirrhotic patients with
thrombocytopenia.
In the present study, eltrombopag treatment
significantly increased platelet count, which subsequently resulted
in successful RFA therapy and the avoidance of platelet
transfusions. These beneficial observations are consistent with
those of previous reports. Eltrombopag has previously been shown to
improve thrombocytopenia and permit interferon therapy in patients
with cirrhosis that is associated with HCV infection (6). More recently, eltrombopag has been
reported to reduce the requirement for platelet transfusions in
cirrhotic patients who have undergone elective invasive procedures
(4). The study included patients
with HCC, however, no monitoring of tumor markers or HCC size was
performed, which was conducted in the present study. Thus,
eltrombopag may replace platelet transfusions, partial splenic
embolization or splenectomy when elective invasive procedures are
performed on cirrhotic patients with thrombocytopenia.
In the current two cases, thrombosis did not develop
during or following eltrombopag treatment. However, certain
previous clinical trials have reported that invasive procedures
increase the risk for the development of thrombosis, even in
cirrhotic patients with thrombocytopenia (4,5). The
risk is proportional to the increasing platelet counts of
>200,000/mm3, which was avoided in the present study
by close monitoring of the patients. Although the reason for the
development of thrombosis remains unclear, von Willebrand factor
levels have been found to increase as an adaptive mechanism in
response to reduced platelet adhesion abilities in cirrhotic
patients (9). Additionally, an
increase was identified in the platelet formation of isoprostanes,
which promote platelet activation via the upregulation of
proaggregatory factors in cirrhotic patients (10,11).
Alternatively, impaired liver function may be involved in the
development of thrombosis, since the majority of eltrombopag is
eliminated in the liver (12).
Higher plasma concentrations of eltrombopag were observed in
patients with Child-Pugh class B when compared with patients with
Child-Pugh class A (5). Thus,
patients must be vigilant for signs of thrombosis, in particular
those with advanced liver cirrhosis, during eltrombopag
treatment.
Hepatic progenitor cells and hepatic sinusoidal
endothelial cells express TPO-R, in addition TPO induces the
proliferation of these two types of cells (7,8).
Furthermore, TPO-R is expressed in hepatoma cell lines, such as
Huh7, Hep3B and HepG2 (13,14); these observations indicate that
eltrombopag may accelerate the progression of HCC. Although
eltrombopag has been administered to treat tumor-bearing patients
(4,15), the effect of eltrombopag on tumor
progression has not previously been reported. In the present study,
it was demonstrated that short-term eltrombopag treatment did not
accelerate the progression of HCC. Although, from the results of
the two cases the possibility that long-term administration of
eltrombopag may accelerate tumor progression cannot be dismissed;
however, subsequent findings may support the hypothesis that
short-term administration of eltrombopag does not accelerate the
proliferation of HCC.
TPO-R expression has previously been found to be
lower in hepatoma cell lines compared with expression in primary
hepatocytes (14) and HCC tissues
do not express TPO-R (13). In
addition, TPO does not activate the extracellular signal-regulated
kinases 1/2 or the signal transducers and activators of
transcription 3 and 5 pathways, or affect the proliferation,
migration or invasion of Huh7 cells (14). Furthermore, TPO does not upregulate
Bax, Bcl-2 or cleaved caspase 3 and does not induce anti-apoptotic
effects in Huh7 cells (14).
Finally, in a previous xenograft experiment, no significant
differences were identified in the tumor volume, tumor appearance
and histological morphology of Huh7 cells that were treated with or
without TPO (14). Thus, the
short-term administration of eltrombopag may not accelerate tumor
progression.
In conclusion, the present study described two cases
of HCC with cirrhosis-related thrombocytopenia. Eltrombopag
treatment increased the platelet count in the two cases and
resulted in successful RFA treatments without platelet transfusions
or serious bleeding. Additionally, no changes were observed in the
serum levels of tumor markers or HCC size. Although eltrombopag is
not currently used for the treatment of thrombocytopenia in
patients with chronic liver disease undergoing invasive procedures,
the observations of the present study indicated that the short-term
administration of eltrombopag may not accelerate the progression of
HCC and may be beneficial for HCC treatment in cirrhotic patients
with thrombocytopenia.
Acknowledgements
The authors would like to thank Professor Nezam H.
Afdhal (Harvard Medical School, Boston, USA) for his helpful
comments.
References
|
1
|
Afdhal N, McHutchison J, Brown R, et al:
Thrombocytopenia associated with chronic liver disease. J Hepatol.
48:1000–1007. 2008. View Article : Google Scholar
|
|
2
|
Kawaguchi T, Kuromatsu R, Ide T, et al:
Thrombocytopenia, an important interfering factor of antiviral
therapy and hepatocellular carcinoma treatment for chronic liver
diseases. Kurume Med J. 56:9–15. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bussel JB, Cheng G, Saleh MN, et al:
Eltrombopag for the treatment of chronic idiopathic
thrombocytopenic purpura. N Engl J Med. 357:2237–2247. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Afdhal NH, Giannini EG, Tayyab G, et al;
ELEVATE Study Group. Eltrombopag before procedures in patients with
cirrhosis and thrombocytopenia. N Engl J Med. 367:716–724. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kawaguchi T, Komori A, Seike M, et al:
Efficacy and safety of eltrombopag in Japanese patients with
chronic liver disease and thrombocytopenia: a randomized,
open-label, phase II study. J Gastroenterol. 47:1342–1351. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McHutchison JG, Dusheiko G, Shiffman ML,
et al; TPL102357 Study Group. Eltrombopag for thrombocytopenia in
patients with cirrhosis associated with hepatitis C. N Engl J Med.
357:2227–2236. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schmelzer E, Deiwick A, Bruns H, Fiegel HC
and Bader A: Thrombopoietin is a growth factor for rat hepatic
progenitors. Eur J Gastroenterol Hepatol. 20:209–216. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cardier JE and Dempsey J: Thrombopoietin
and its receptor, c-mpl, are constitutively expressed by mouse
liver endothelial cells: evidence of thrombopoietin as a growth
factor for liver endothelial cells. Blood. 91:923–929. 1998.
|
|
9
|
Lisman T, Bongers TN, Adelmeijer J, et al:
Elevated levels of von Willebrand Factor in cirrhosis support
platelet adhesion despite reduced functional capacity. Hepatology.
44:53–61. 2006. View Article : Google Scholar
|
|
10
|
Basili S, Raparelli V, Riggio O, et al;
CALC Group. NADPH oxidase-mediated platelet isoprostane
over-production in cirrhotic patients: implication for platelet
activation. Liver Int. 31:1533–1540. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Violi F and Pignatelli P: Eltrombopag
before procedures in patients with cirrhosis and thrombocytopenia.
N Engl J Med. 367:20562012.PubMed/NCBI
|
|
12
|
Haselboeck J, Kaider A, Pabinger I and
Panzer S: Function of eltrombopag-induced platelets compared to
platelets from control patients with immune thrombocytopenia.
Thromb Haemost. 109:676–683. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Columbyova L, Loda M and Scadden DT:
Thrombopoietin receptor expression in human cancer cell lines and
primary tissues. Cancer Res. 55:3509–3512. 1995.PubMed/NCBI
|
|
14
|
Nozaki R, Murata S, Nowatari T, et al:
Effects of thrombopoietin on growth of hepatocellular carcinoma: Is
thrombopoietin therapy for liver disease safe or not? Hepatol Res.
43:610–620. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chawla SP, Staddon A, Hendifar A, Messam
CA, Patwardhan R and Kamel YM: Results of a phase I dose escalation
study of eltrombopag in patients with advanced soft tissue sarcoma
receiving doxorubicin and ifosfamide. BMC Cancer. 13:1212013.
View Article : Google Scholar : PubMed/NCBI
|