Introduction
Adenoid cystic carcinoma (ACC) of the larynx is an
extremely rare disease that arises from the laryngeal glandular
elements (1). Approximately two
thirds of laryngeal ACCs arise in the subglottis. Compared with
subglottic and glottic ACCs, supraglottic ACC is less common
(2). The clinical characteristics
of supraglottic ACC can be confused with those of laryngeal
amyloidosis, which is a rare benign tumor. Amyloidosis refers to a
variety of conditions wherein normally soluble proteins become
insoluble and are deposited in the extracellular space. Amyloidosis
with larynx-only localization is rare. The objective of this study
is to show that the duration and progression of laryngeal ACCs may
be quite variable, occasionally appearing as benign as amyloidosis,
and the predilection for unnoticeable spreading may account for the
locally advanced tumors and would also account for the high
incidence of positive or even ‘negative’ margins on surgical
specimens. Written informed consent was obtained from the
patient.
Case report
A 44-year-old woman with a six-month history of
progressive hoarseness and an abnormal sensation in the throat was
referred to the Nanjing Drum Tower Hospital (Nanjing, China). The
patient had no history of smoking, coughing, dyspnea or dysphagia;
however, it is worth noting that the patient was exposed to iron
ore and coal dust for several years in the work place. In addition,
the patient had a history of over five years of second-hand smoke
inhalation.
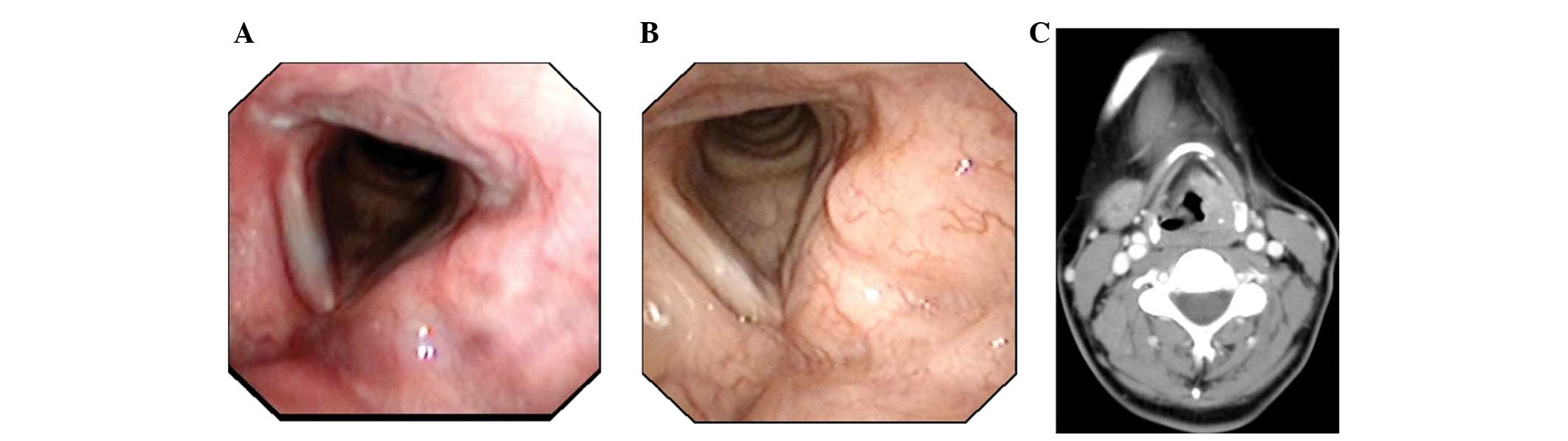
Fiberoptic laryngoscopy revealed swelling of the
left ventricular fold and laryngeal ventricle that extended
backwards to the left aryepiglottic fold. The bilateral vocal cords
appeared normal and there was no vocal cord paralysis (Fig. 1A). The patient subsequently refused
any further examinations. The laryngeal abnormal sensation
gradually progressed, and after 18 months the patient underwent a
second laryngoscopy, which revealed similar findings to the first
without obvious progression (Fig.
1B). Computed tomography (CT) revealed a mass involving the
left ventricular fold and anterior commissure. The left pyriform
sinus was not distinguished (Fig.
1C). Neither physical examination or neck CT detected any
tumescent lymph nodes in the neck, and the chest X-ray was
normal.
The preoperative diagnosis that was deemed most
likely was that of a laryngeal neoplasm with laryngeal amyloidosis.
The subsequent frozen section biopsy of the lesion taken during
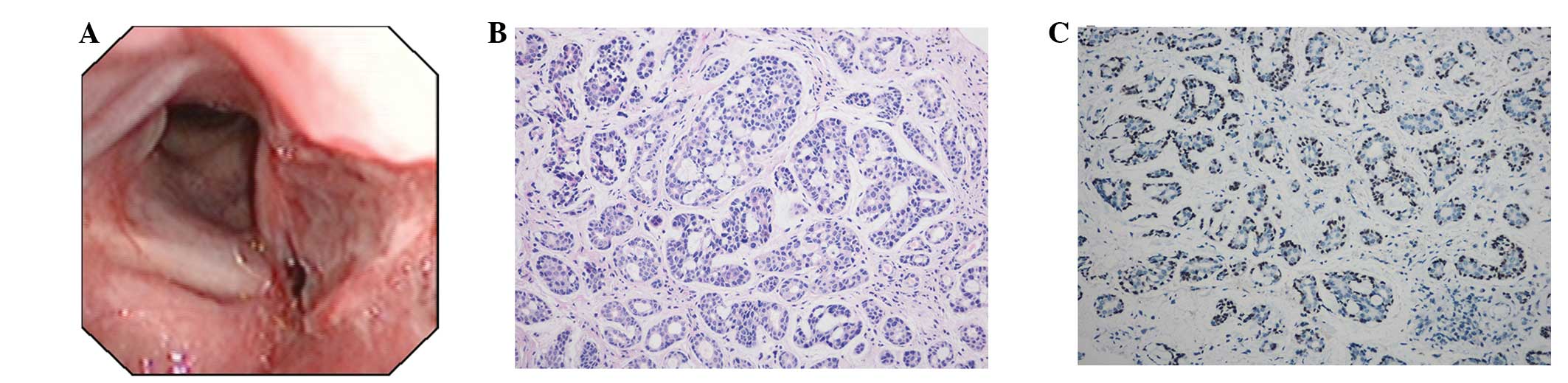
laryngofissure revealed the nature of the neoplasm. As the patient
refused to undergo an expanded total laryngectomy, which is
indicated for a locally advanced laryngeal tumor (3), local resection of the left ventricular
fold, laryngeal ventricle and aryepiglottic fold was performed only
(Fig. 2A). The margin of the
biopsied tissue surrounding the lesion was negative. Although there
was no sign of lymphatic spreading, perineural invasion existed,
therefore, it was suggested that radiotherapy be performed at one
month post-surgery (4). However,
one month later and prior to this radiotherapy, regional recurrence
of the tumor was identified. With informed consent from the
patient, a total laryngectomy without neck dissection was
performed, as no lymph nodes were found to be involved (5). The tumor invaded the left side of the
throat up to the root of the epiglottis, down from just beneath the
true vocal cords into the subglottis ~1 cm and crossed to the right
supraglottic area. The post-operative pathological findings
confirmed the diagnosis of ACC and the histopathological pattern
was a mixed cribriform and tubular subtype (Grade I; Fig. 2B) (6). Immunocytochemistry revealed positive
staining for p63 (Fig. 2C),
carcinoembryonic antigen, cytokeratin 5/6 and 8/18, epithelial
membrane antigen, S100 and cytokeratin smooth muscle actin.
Although adjuvant radiotherapy is known to provide superior disease
control, p63 staining was positive (7,8). The
patient rejected radiotherapy as it would not cure the disease, but
selected traditional Chinese medicine as an adjuvant therapy.
During the 42-month follow-up period, there was no evidence of
regional relapse or distant metastases.
Discussion
ACC of the head and neck typically arises in the
major and minor salivary glands (9). As accessory salivary glands are
exiguous in the larynx, laryngeal ACC is a rare disease, accounting
for <1% of all malignant tumors in this area (10). When ACC occurs in the supraglottis,
it often involves the false cords, the aryepiglottic folds and the
caudal aspect of the epiglottis. In the glottis, ACCs are located
in the floor of the laryngeal ventricle and subglottic surface of
the anterior commissure (11). As
ACCs spread in an unnoticeable submucosal and perineural fashion,
early diagnosis is difficult, therefore, when a patient is referred
to hospital, the disease is often at the advanced stage. In the
present study, the laryngeal ACC was at stage II (T2N0M0) prior to
biopsy, but at the revision surgery the tumor was at stage IV.
Grade I ACC is commonly associated with early
recurrence and an earlier risk of distant metastases (12). In the present case, the
extraordinary short time of recurrence may result from the
misleading ‘negative’ margins, and it is possible that unrecognized
invasion of specimens existed in this case. Furthermore, it may be
due to the lack of adjuvant radiotherapy, although this has not yet
been confirmed by randomized clinical studies. In addition,
staining was positive for p63, whose alteration was an independent
prognostic marker and associated with radiotherapy resistance.
Laryngeal ACC may be easily misdiagnosed as
laryngeal amyloidosis, whose manifestation is similar (7). Laryngeal amyloidosis is one of the
rare benign tumors of the larynx, accounting for <1% of all
benign tumors of this region. Laryngeal amyloidosis is
characterized by the presence of extracellular fibrillar proteins
in the laryngeal tissues and may be localized without systematic
manifestations. The accumulation of amyloid deposits affects the
normal structure and function of laryngeal tissues (13).
In the present case, the patient was misdiagnosed
with laryngeal amyloidosis due to the following: i) The medical
history of the patient revealed a female non-smoker with a two-year
slow progression of symptoms; ii) the symptoms included hoarseness
and an uncomfortable laryngeal sensation, but not dyspnea,
dysphagia or stridor; and iii) the diagnostic tests revealed normal
chest X-ray results and submucosal masses involving the left
ventricular fold, aryepiglottic fold and pyriform sinus without
vocal cord fixation or paralysis upon fiberoptic laryngoscopy and
CT. Therefore, no clear malignancy was indicated.
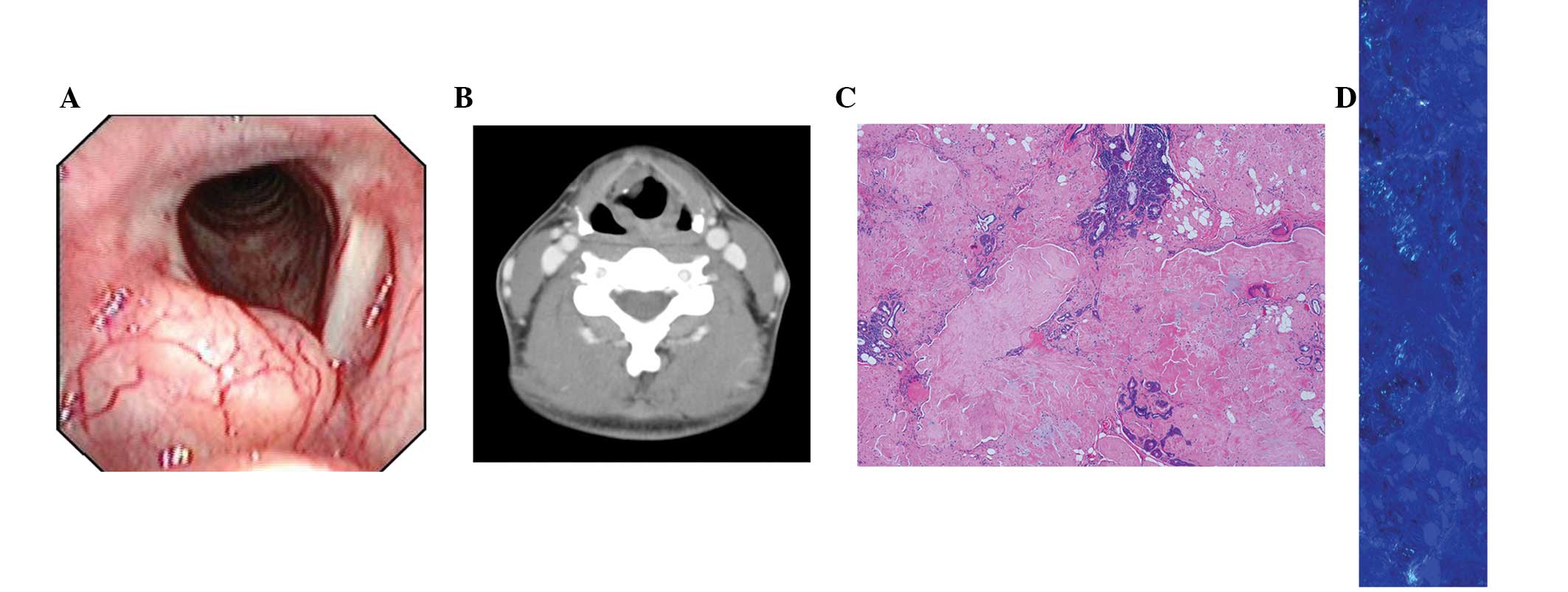
In comparison, one month prior to the present case,
a 33-year-old female attended an appointment at the Nanjing Drum
Tower Hospital and was diagnosed with laryngeal amyloidosis. The
patient presented with an abnormal sensation in the throat. The
findings of the laryngoscopy and CT scan are shown in Fig. 3A and B and are similar to those of
laryngeal ACC. By specific Congo red staining, amyloid appeared as
a diffuse subepithelial extracellular deposit of amorphous
eosinophilic material and as hyaline rings. Dense amyloid cracks in
tissue sections left cleft-like spaces (Fig. 3C). Under polarized light, amyloid
displayed typical apple-green birefringence (Fig. 3D).
Laryngeal ACC recurs quickly and requires sufficient
management during the first treatment modality. Thus, we suggest a
biopsy with specific immunocytochemical staining as the first
treatment strategy. With developing molecular biology, novel
therapeutic regimens may be identified from traditional Chinese
medicine.
Supraglottic ACC of the larynx is a rare entity and
is often disregarded. This diagnosis should be considered in
patients presenting with progressive hoarseness and an abnormal
sensation in the throat, even if there are no other presenting
symptoms and with/without a negative chest X-ray. Pre-operative
histopathological analysis is essential for an earlier differential
diagnosis of laryngeal amyloidosis. In our opinion, prospective
randomized multicenter studies are required to determine an optimal
treatment. Traditional Chinese medicine may be a post-operative
treatment regimen instead of radiotherapy; however, it requires
further investigation.
References
|
1
|
Tewfik TL, Novick WH and Schipper HM:
Adenoid cystic carcinoma of the larynx. J Otolaryngol. 12:151–154.
1983.PubMed/NCBI
|
|
2
|
Dexemble P, Huth J, Rebufy M and Chabrol
A: Carcinome adénoïde kystique du larynx. A propos de deux cas. Ann
Otolaryngol Chir Cervicofac. 120:244–248. 2003.(In French).
|
|
3
|
Ganly I, Patel SG, Coleman M, Ghossein R,
Carlson D and Shah JP: Laryngeal adenoid cystic carcinoma: A report
of two cases. Arch Otolaryngol Head Neck Surg. 132:767–770.
2006.
|
|
4
|
Stillwagon GB, Smith RR, Highstein C and
Lee DJ: Adenoid cystic carcinoma of the supraglottic larynx: report
of a case and review of the literature. Am J Otolaryngol.
6:309–314. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moukarbel RV, Goldstein DP, O’Sullivan B,
Gullane PJ, Brown DH, Wang L, et al: Adenoid cystic carcinoma of
the larynx: A 40-year experience. Head Neck. 30:919–924.
2008.PubMed/NCBI
|
|
6
|
Tincani AJ, Del Negro A, Araújo PP, Akashi
HK, Martins AS, Altemani AM, et al: Management of salivary gland
adenoid cystic carcinoma: institutional experience of a case
series. Sao Paulo Med J. 124:26–30. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Batsakis JG, Luna MA and el-Naggar AK:
Nonsquamous carcinoma of the larynx. Ann Otol Rhinol Laryngol.
101:1024–1026. 1992.PubMed/NCBI
|
|
8
|
Chen AM, Bucci MK, Weinberg V, Garcia J,
Quivey JM, Schechter NR, et al: Adenoid cystic carcinoma of the
head and neck treated by surgery with or without postoperative
radiation therapy: prognostic features of recurrence. Int J Radiat
Oncol Biol Phys. 66:152–159. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Olofsson J and van Nostrand AW: Adenoid
cystic carcinoma of the larynx: a report of four cases and a review
of the literature. Cancer. 40:1307–1313. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Alavi S, Namazie A, Calcaterra TC and
Blackwell KE: Glandular carcinoma of the larynx: the UCLA
experience. Ann Otol Rhinol Laryngol. 108:485–489. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nagel H, Hotze HJ, Laskawi R, Chilla R and
Droese M: Cytologic diagnosis of adenoid cystic carcinoma of
salivary glands. Diagn Cytopathol. 20:358–366. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bradley PJ: Adenoid cystic carcinoma of
the head and neck: A review. Curr Opin Otolaryngol Head Neck Surg.
12:127–132. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dedo H and Izdebski K: Laryngeal
amyloidosis in 10 patients. Laryngoscope. 114:1742–1746. 2004.
View Article : Google Scholar : PubMed/NCBI
|