Introduction
Alkylating agents comprise a large class of
chemotherapeutic drugs used to treat several types of cancers.
Alkylating agents cause cell death by forming cross-links between
adjacent strands of DNA via alkylation at the
O6-position of guanine. O6-Methylguanine-DNA
methyltransferase (MGMT) is a DNA repair protein that prevents
cross-link formation by transferring the alkyl group to an internal
cysteine residue, restoring guanine in the DNA and inactivating
itself in the process. Various human tumor cell lines and
xenografts have been used to demonstrate the association between
the activity of MGMT and the ability to withstand methylating
agents and alkylating nitrosoureas (1).
Cyclophosphamide (CPM) has been used against a broad
spectrum of malignancies. CPM is unique in its lack of alkylating
activity, requiring in vivo metabolic activation to produce
active alkylating compounds (2). In
an in vivo mouse xenograft study, lung tumor xenografts with
high MGMT activity were revealed to be less sensitive to the
growth-inhibitory effects of CPM than those with low MGMT activity
(3). However, another study of 23
varying xenograft tumors showed no correlation between CPM
anti-tumor and MGMT tumor activity (4). In clinical studies, MGMT negativity
was associated with significantly increased overall survival (OS)
among patients with diffuse large B-cell lymphoma following
treatment with CPM and other drugs (5,6).
However, in the patients with breast cancer that was treated with
neoadjuvant chemotherapy, including CPM, no correlation was
observed between MGMT expression and the response to CPM (7). Conversely, a recent study demonstrated
the predictive value of MGMT protein expression in breast tumor
biopsies obtained prior to CPM-containing neoadjuvant chemotherapy
(8).
MGMT is ubiquitously expressed in normal human
tissues. Levels of MGMT are known to vary considerably between
individuals and organ types, and MGMT activity is usually higher in
malignant tissues compared with normal tissues (9). In breast tumors, MGMT expression can
be up to 4-fold higher compared with normal breast tissues
(10,11). Certain clinical studies have
indicated that MGMT expression correlates with the prognosis of
breast cancer, whereas other clinical studies have failed to
elucidate any association between MGMT expression and OS in
patients with breast cancer (7,12–14).
The longstanding belief has been that breast tumors are
heterogeneous with respect to MGMT expression, however, these
contradictory results could be due to the majority of previous
studies being evaluated in heterogeneous groups of patients with
breast cancer (15).
Gene expression profiling studies on breast tumors
have identified 4 main intrinsic molecular subtypes of breast
cancer. These are the luminal A, luminal B, human epidermal growth
factor receptor-2 (HER2)-enriched and basal-like subtypes (16,17).
These subtypes exhibit significant differences in terms of
incidence, risk factors, prognosis and response to treatment
(18). The prognosis of basal-like
cancers tends to be poor. As their response to chemotherapy is
poorly understood, optimal chemotherapy regimens and reliable
prognostic and predictive factors for these cancers are widely
sought after. A recent study indicated that the MGMT promoter
methylation status predicts tumor response to alkylating drugs in
patients with triple-negative (TN) breast cancer (19). In the present study,
immunohistochemical analyses of breast tumor subtypes and MGMT
protein expression were conducted using formalin-fixed,
paraffin-embedded specimens obtained from patients with breast
cancer. The correlation between MGMT expression and prognosis in
the subtypes of breast cancer, managed according to common
therapeutic protocols, was then investigated. The association
between MGMT expression and the clinical outcome was examined to
explore the possibility of MGMT expression as a predictive marker
in patients with breast cancer treated with CPM-containing
chemotherapy.
Materials and methods
Patients
Between November 2006 and December 2010, 1,049
patients with breast cancer underwent surgery at Kinki University
Hospital (Osaka-Sayama, Osaka, Japan). In total, 635 patients with
invasive breast carcinomas, whose resected materials were suitable
for further immunohistochemical examinations, were selected
(Table I). The ages of the patients
ranged between 22 and 89 years (median, 58 years). All patients
provided written informed consent for collection of their tissue
material and clinical data for research purposes, and the study
protocol was approved by the institutional review board (Kinki
University Hospital, Osaka-Sayama, Osaka, Japan). None of the
patients had distant metastasis or underwent pre-operative therapy.
Adjuvant therapy was individually based on indicators of treatment
response (hormone and HER2 status) and risk indicators. The
patients who underwent breast-conserving surgery received
post-operative radiotherapy to the residual breast tissue (50 Gy in
25 fractions).
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Total patients
(n=635) |
|---|
|
|
|---|
| Variables | No. | % |
|---|
| Menopausal
status |
| Pre | 202 | 32 |
| Post | 433 | 68 |
| TNM stage |
| I | 254 | 40 |
| II | 326 | 51 |
| III | 55 | 9 |
| Node status |
| Negative | 400 | 63 |
| Positive | 235 | 37 |
| Estrogen
receptor |
| Negative | 122 | 19 |
| Positive | 513 | 81 |
| Progesterone
receptor |
| Negative | 162 | 26 |
| Positive | 473 | 74 |
| HER2 |
| Negative | 493 | 78 |
| Positive | 142 | 22 |
Immunohistochemical analysis of breast
cancer subtype
Representative portions of formalin-fixed,
paraffin-embedded tumor-containing sections were prepared for
hematoxylin and eosin staining to confirm invasive carcinoma, and
then serial 4-μm thick sections were generated for
immunohistochemical analysis. The Allred scoring system was used to
measure estrogen receptor (ER) and progesterone receptor (PgR)
expression. HER2 analysis was based on the American Society of
Clinical Oncology/College of American Pathologists guidelines
(20). Immunostaining of
cytokeratin (CK) 5/6 and EGFR (HER1) was performed as described
previously, and positivity for CK 5/6 and EGFR was evaluated by two
investigators who were blinded to the clinical outcomes (21). CK 5/6 was scored as positive when
≥1% of invasive tumor cells exhibited strong cytoplasmic and/or
membranous staining. Positivity for EGFR was defined as the
detection of ≥10% of cells in the invasive tumors exhibiting strong
membrane staining (22).
Immunohistochemical staining of MGMT
The immunohistochemical procedures were as
previously described (23).
Briefly, paraffin sections were deparaffinized and antigen
retrieval was performed by microwaving the samples. Endogenous
peroxidase activities were blocked with 3% hydrogen peroxidase in
methanol. Following the blocking of the non-specific binding with
10% normal goat serum, the sections were incubated with a 1:20
dilution of anti-MGMT mouse monoclonal antibody (clone MT3.1;
Chemicon, Bioscience Research Reagents, Temecula, CA, USA) for 60
min at room temperature. Staining was achieved using the Envision
kit according to the manufacturer’s instructions (Dako,
Carpinteria, CA, USA). To assess MGMT immunostaining, each slide
was individually reviewed and scored by two investigators. At least
1,000 tumor cell nuclei were evaluated in each specimen, in fields
exhibiting the highest density of immunopositive cells. Samples
were considered positive when immunoreactivity was detected in
>10% of cell nuclei.
Statistical analysis
Statistical analysis was performed using JMP
software, version 8 (SAS Institute, Inc., Cary, NC, USA).
Correlations between tumor characteristics and MGMT protein
expression were determined using the χ2 test. The
probabilities of OS and disease-free survival (DFS) were calculated
according to the Kaplan-Meier method and were compared using the
log-rank test. The OS time was measured from the date of definitive
surgery to the date of the last follow-up or mortality from any
cause. DFS events included local, regional or distant breast cancer
recurrences, second cancer (in the contralateral breast and
non-breast cancers) and all mortalities from the time of surgery.
All tests were two-sided and P<0.05 was considered to indicate a
statistically significant difference.
Results
Immunohistochemical subtypes
In total, the 635 cases of invasive carcinoma were
classified into 5 clinical subtypes using immunohistochemical
markers as follows: Luminal A (ER+ and/or
PgR+ and HER2−), luminal B (ER+
and/or PgR+ and HER2+),
HER2+/ER− (ER−, PgR−
and HER+), basal-like (ER−, PgR−,
HER2−, CK 5/6+ and/or HER1+) and
unclassified (negative for all 5 markers) (24). Of the 635 primary tumors analyzed in
the present study, 425 (67%) were luminal A, 95 (15%) were luminal
B, 47 (7%) were HER2+/ER−, 48 (7%) were
basal-like and 20 (3%) were unclassified. Clinicopathological
features were not significantly correlated with immunohistochemical
subtypes.
Immunohistochemical analysis of MGMT
protein expression
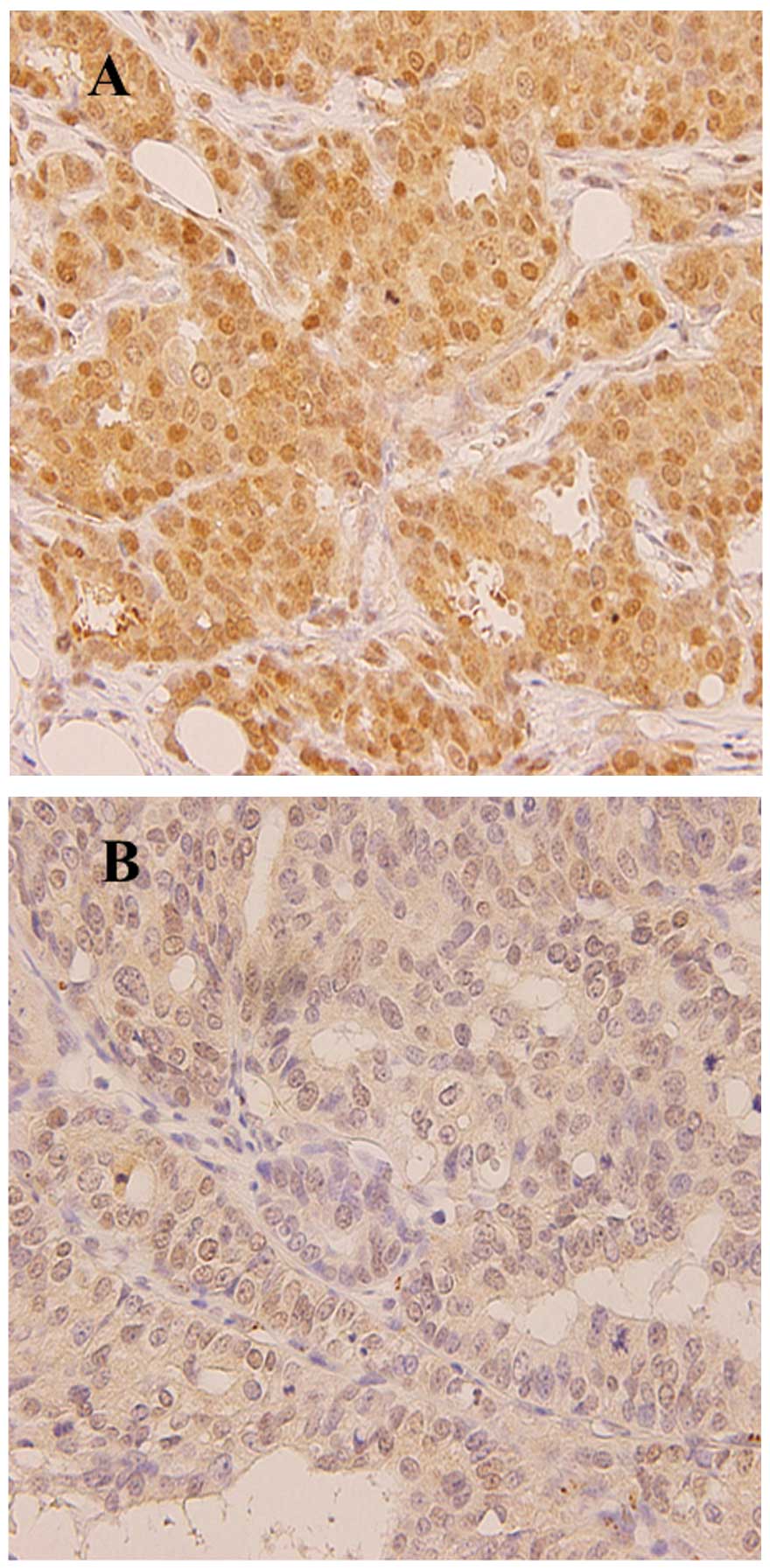
Immunohistochemistry revealed intense nuclear
staining and weak cytoplasmic staining for MGMT in the tumor cells
(Fig. 1). Tumors were defined as
MGMT-positive when >10% of cells exhibited nuclear staining.
MGMT positivity was identified in 398 (63%) of 635 patients with
breast cancer. The characteristics of the 635 patients according to
the MGMT immunoreactivity are presented in Table II. The frequency of MGMT protein
expression was significantly higher in the tumors with no lymph
node metastasis compared with the tumors positive for lymph node
metastasis. The MGMT status was significantly correlated with the
hormone receptor status. A significant inverse correlation between
the MGMT status and the HER2 and HER1 status was observed (Table II). MGMT positivity was identified
in 68% of luminal A and 67% of luminal B tumors, whereas MGMT
negativity was significantly more common in
HER2+/ER− tumors. In total, 22 (46%)
basal-like tumors were MGMT-positive. MGMT expression was not
significantly correlated with breast cancer subtype.
| Table IIAssociation between MGMT status and
clinicopathological variables. |
Table II
Association between MGMT status and
clinicopathological variables.
| MGMT, n (%) | |
|---|
|
| |
|---|
| Variables | Positive | Negative | P-value |
|---|
| TNM stage |
| I | 172 (68) | 82 (32) | 0.09 |
| II | 195 (60) | 131 (40) | |
| III | 31 (56) | 24 (44) | |
| Node status |
| Negative | 264 (66) | 136 (34) | 0.02 |
| Positive | 134 (57) | 101 (43) | |
| Estrogen
receptor |
| Negative | 49 (40) | 73 (60) | 0.001 |
| Positive | 349 (68) | 164 (32) | |
| Progesterone
receptor |
| Negative | 76 (47) | 86 (53) | 0.001 |
| Positive | 322 (68) | 151 (32) | |
| HER2 |
| Negative | 320 (65) | 173 (35) | 0.03 |
| Positive | 78 (55) | 64 (45) | |
| CK 5/6 |
| Negative | 372 (63) | 222 (37) | 0.87 |
| Positive | 27 (66) | 14 (34) | |
| HER1 |
| Negative | 371 (65) | 203 (35) | 0.01 |
| Positive | 28 (46) | 33 (54) | |
| Subtype |
| Luminal A | 291 (68) | 134 (32) | 0.001 |
| Luminal B | 64 (67) | 31 (33) | |
|
HER2+/ER− | 14 (30) | 33 (70) | |
| Basal-like | 22 (46) | 26 (54) | |
| Unclassified | 7 (35) | 13 (65) | |
Clinical significance of MGMT protein
expression
The patients in the study received systemic
therapies based on indicators of treatment response (tumor hormone
and HER2 status of the tumor) and risk. Following surgery, 2% of
patients received no adjuvant therapy, 60% received endocrine
therapy, 17% received chemotherapy and 21% received endocrine
therapy and chemotherapy. The median follow-up time after surgery
was 4.6 years (range, 0.9–7.8 years). OS and DFS rates differed
significantly according to the breast cancer subtype, and were
significantly worse for patients with basal-like tumors than for
those with luminal A tumors.
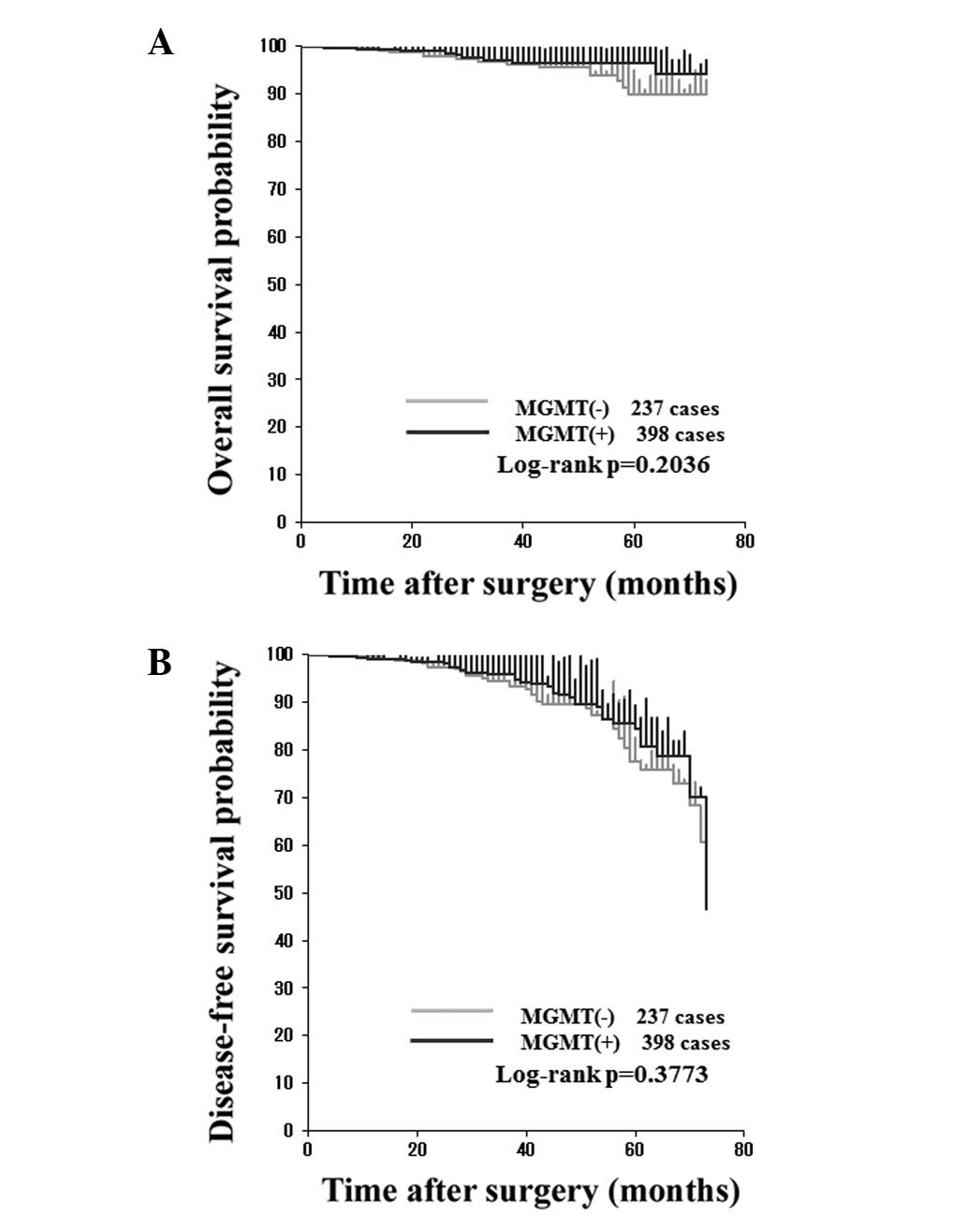
The prognostic significance of MGMT protein
expression was analyzed. OS and DFS rates did not significantly
differ between the patients with MGMT-positive tumors and those
with MGMT-negative tumors (Fig. 2).
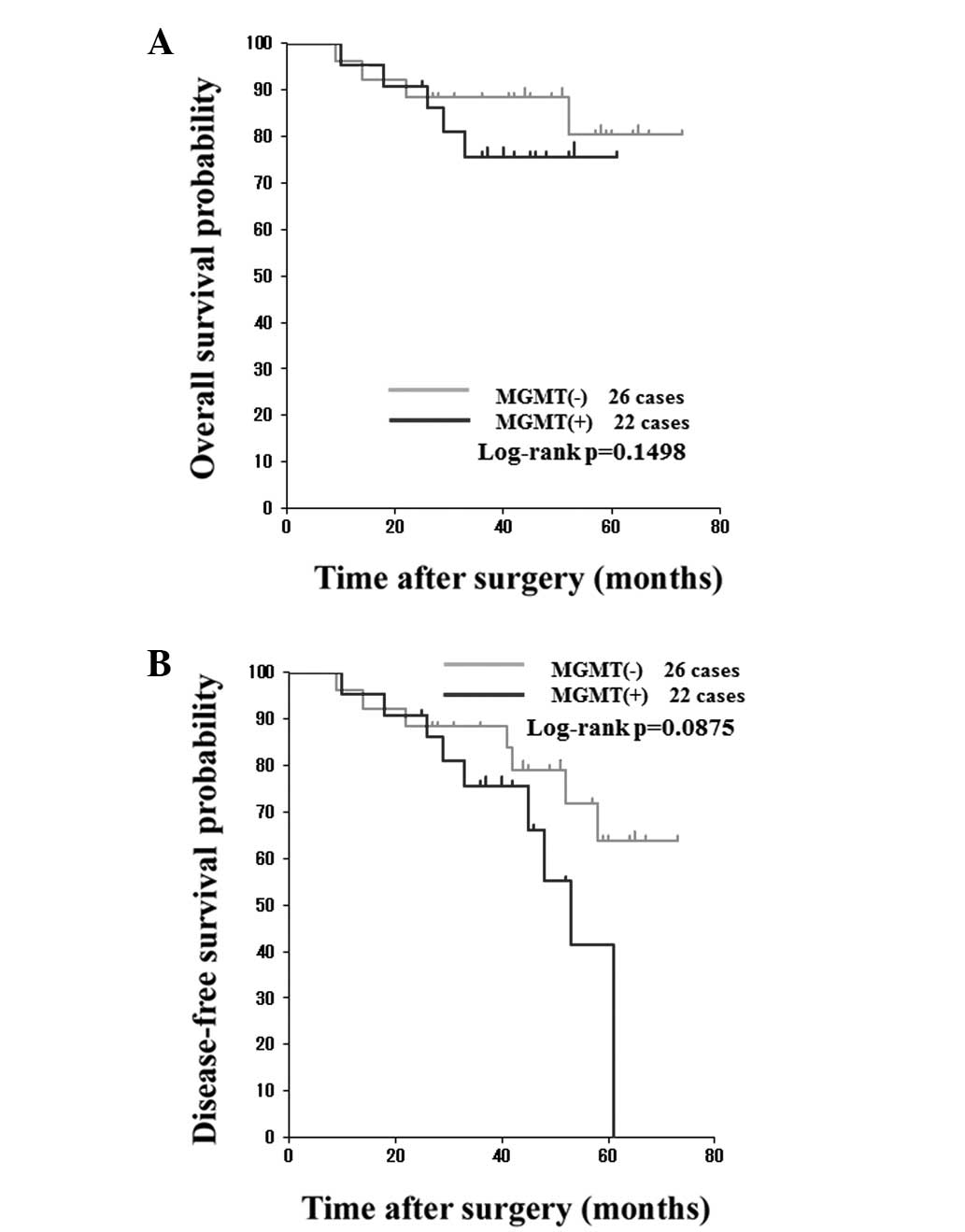
In comparing the clinical outcomes of the patients with
MGMT-positive tumors with those of the patients with MGMT-negative
tumors according to immunohistochemical subtypes, no statistically
significant difference in OS and DFS rates was found according to
MGMT expression for luminal A, luminal B or
HER2+/ER− tumors. However, Kaplan-Meier
estimates revealed that the patients with MGMT-negative basal-like
tumors tended to have better DFS, but not OS, compared with those
with MGMT-positive tumors (Fig.
3).
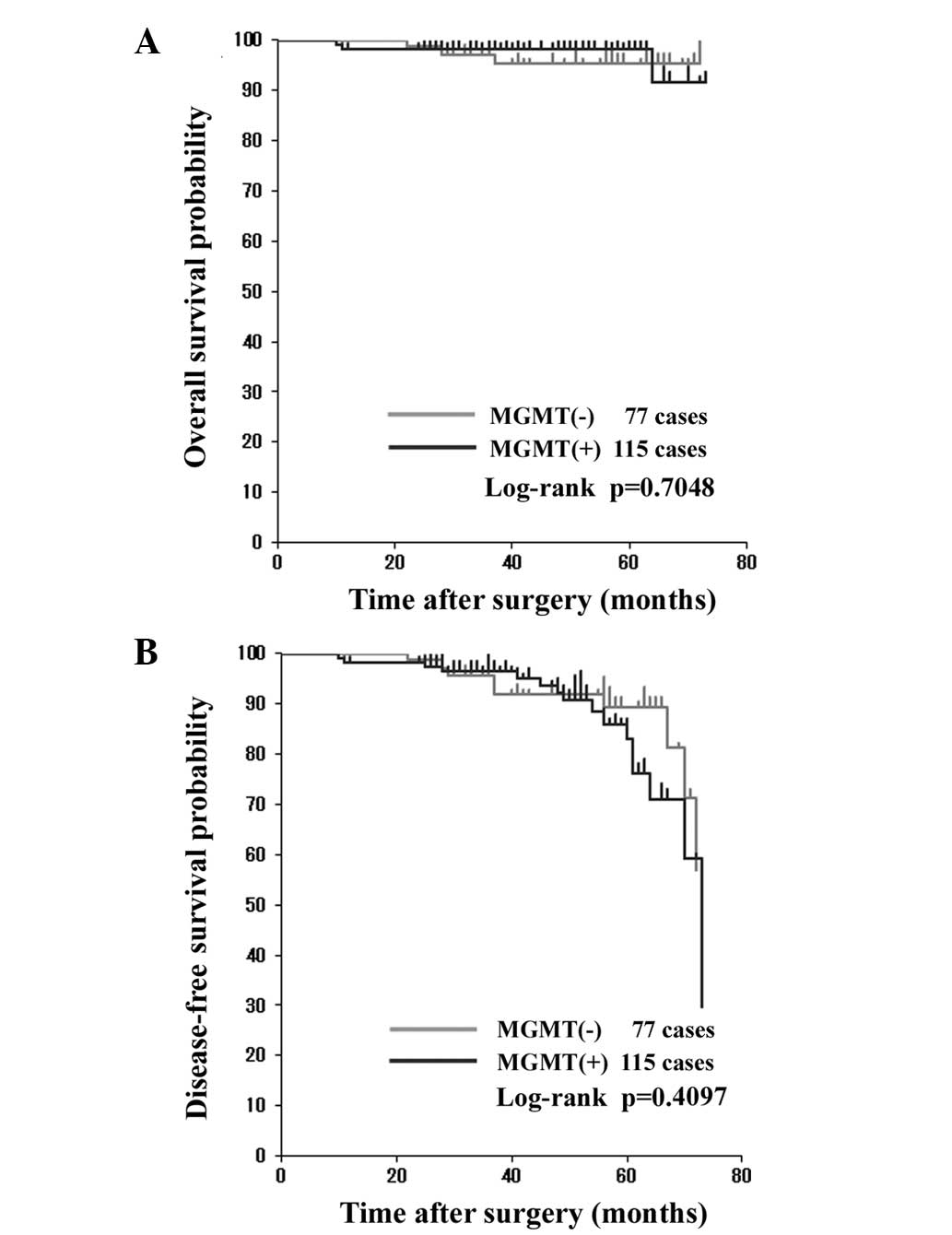
The potential of MGMT protein expression as a
predictive marker for the efficacy of alkylating agents was
investigated. CPM-containing chemotherapy was administered to 112
(26%), 38 (40%), 22 (47%) 15 (31%) and 5 (25%) patients with
luminal A, luminal B, HER2+/ER−, basal-like
and unclassified tumors, respectively. Of the 192 patients who
received CPM-containing chemotherapy, 115 exhibited MGMT-positive
tumors. Kaplan-Meier estimates of OS and DFS rates for the patients
who received CPM revealed no significant differences according to
MGMT expression (Fig. 4). The
clinical outcomes of patients with luminal A, luminal B or
HER2+/ER− tumors treated with CPM-containing
regimens were analyzed. OS and DFS rates in the patients with
luminal A, luminal B or HER2+/ER− tumors did
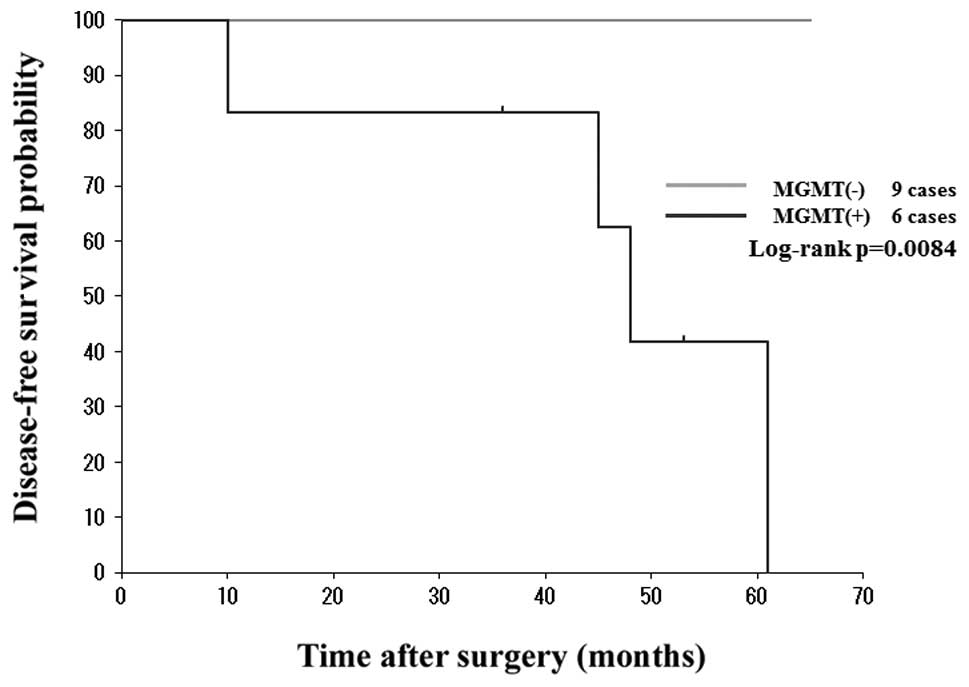
not differ significantly according to the MGMT status. Among the
basal-like tumors from the 15 patients who received CPM-containing
regimens as adjuvant chemotherapy, 6 were MGMT-positive and 9 were
MGMT-negative. When analyzing the clinical outcomes of these
patients, no recurrence was observed in those with MGMT-negative
tumors, however, 4 of the 6 patients with MGMT-positive tumors had
breast cancer recurrences. Patients with MGMT-negative tumors had a
significantly improved DFS rate compared with the patients with
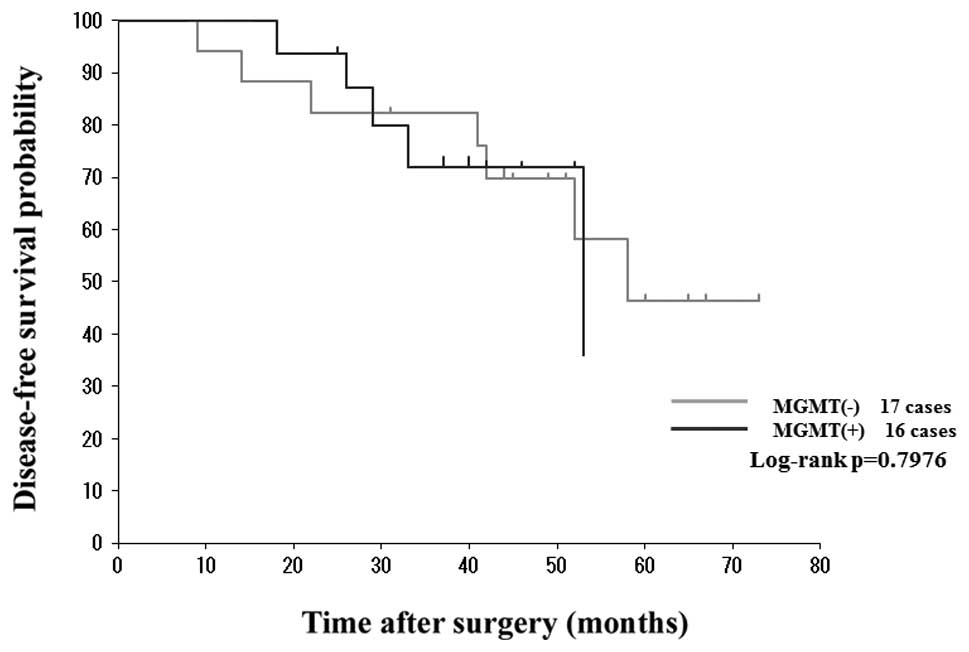
MGMT-positive tumors (Fig. 5). By
contrast, Kaplan-Meier estimates of DFS in the 33 patients with
basal-like tumors who were not administered CPM as an adjuvant
therapy revealed no statistical differences according to MGMT
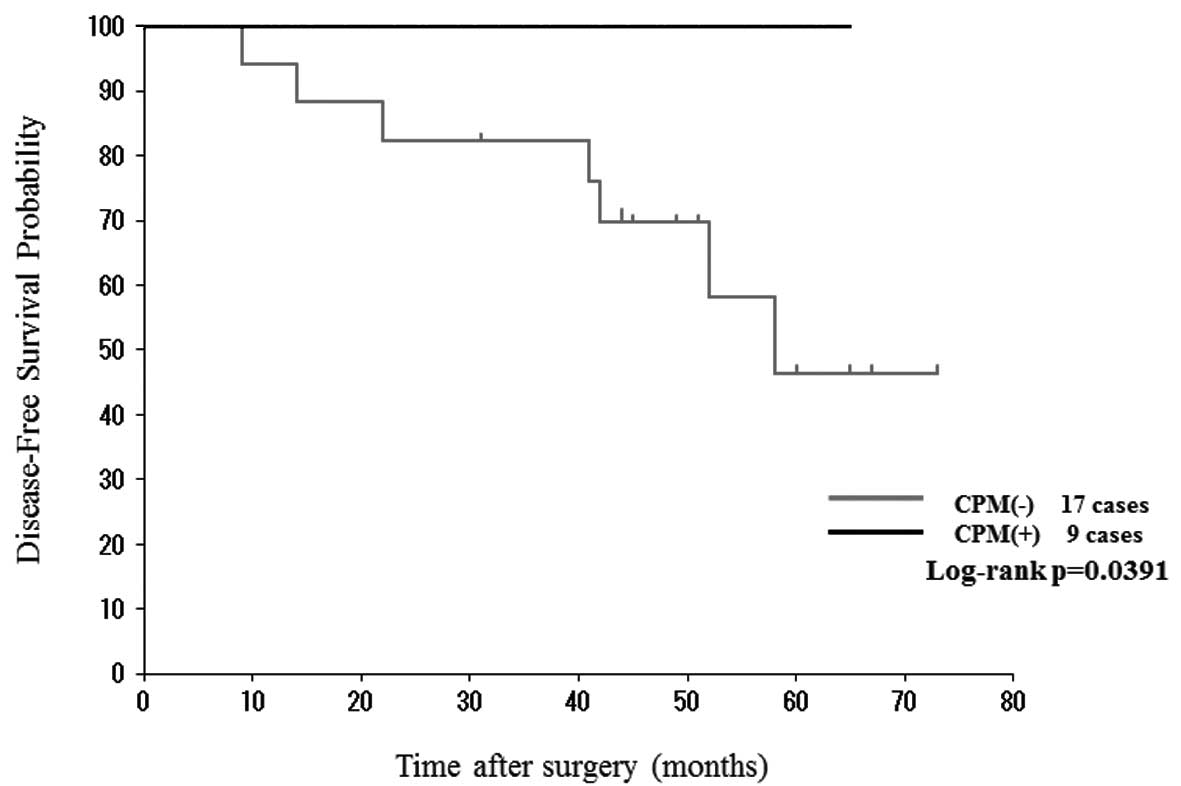
expression (Fig. 6). Of the 48
patients with basal-like tumors, 26 had MGMT-negative tumors. Among
these 26 patients, 9 received CPM-containing adjuvant chemotherapy.
Compared with the patients treated with CPM-containing
chemotherapy, the patients who did not receive CPM-containing
chemotherapy had a significantly poor prognosis (Fig. 7).
Discussion
Numerous methods have been used to analyze MGMT
status in a wide-spectrum of human tumors. In the present study,
MGMT status was assessed in patients with breast cancer by
analyzing MGMT protein expression using an immunohistochemical
method, which can be easily performed without specific equipment,
even on archived formalin-fixed, paraffin-embedded specimens,
together with other immunohistochemical studies for tumor
diagnosis. MGMT protein expression was studied in a large series of
cases from a single institution using an immunohistochemical
method. In total, 63% of the 635 patients with breast cancer
harbored MGMT-positive tumors. To the best of our knowledge, using
various anti-MGMT antibodies and applying diverse criteria for MGMT
immunopositivity, immunohistochemical studies concerning MGMT
protein expression in breast cancer have demonstrated that 54–81%
of breast cancers are MGMT-positive (8,12–14,25,26).
To clarify the clinical relevance of MGMT expression
in patients with breast cancer, the association between
clinicopathological factors and MGMT status in breast cancers was
investigated first. Breast cancers with no lymph node metastasis
were more likely to be MGMT-positive than those with positive lymph
nodes. MGMT status showed a strong correlation with ER and PgR
status and a significant, inverse correlation with HER2 status. The
patients with ER-positive disease received endocrine therapy, and
anti-HER2 therapy was indicated in the patients with HER2-positive
disease. However, MGMT expression was not correlated with OS or DFS
among the patients with breast cancer in the present study.
Next, MGMT protein expression as a possible
prognostic factor in breast cancer subtypes was examined using the
Kaplan-Meier method. Although Neto et al did not analyze
clinical outcome of patients with breast cancer, the study
indicated that MGMT expression was correlated with factors for a
poor prognosis, including the molecular phenotype of breast cancers
(14). The present study found no
significant association between MGMT status and the clinical
outcome of patients with luminal A, luminal B,
HER2+/ER− and basal-like subtypes. It was
therefore concluded that MGMT protein expression generally has no
prognostic value for breast cancers.
In the present study, basal-like cancer was defined
as ER−, PgR−, HER2−, CK
5/6+ and/or EGFR+ tumors using
immunohistochemical surrogate markers (24). Patients with basal-like breast
cancers do not benefit from molecular-targeted treatments,
including endocrine therapy or trastuzumab. A previous in
vivo study demonstrated that chemosensitivity in human cells
lacking BRCA1, and to a certain extent other TN cells, may be
sensitive to drugs that cause double-strand breaks in DNA,
including alkylating agents (27).
Although basal-like breast cancer is not identical to TN tumors,
previous retrospective studies have indicated that classical CPM,
methotrexate and fluorouracil chemotherapy may be beneficial for
breast cancer patients with TN phenotypes (28–30).
In the present study, approximately one-third of the patients with
basal-like breast cancer received CPM-containing adjuvant
chemotherapy. Among the patients with basal-like breast cancer
treated with a CPM-containing regimen, those with MGMT-negative
tumors had a better DFS rate compared with those with MGMT-positive
tumors. Furthermore, among the patients with basal-like breast
cancer with an MGMT-negative phenotype, those who received
CPM-containing chemotherapy exhibited an improved DFS rate compared
with those who received chemotherapy without CPM. However, the
clinical outcomes of patients with other subtypes of breast cancer
were independent of the MGMT status, irrespective of the treatment
with CPM-containing chemotherapy. Taken together, the results of
the present study indicate that MGMT protein expression could be a
useful prognostic and predictive marker of patients with basal-like
breast cancer who are treated with CPM-containing chemotherapy.
The majority of chemotherapeutic regimens that have
been used to treat all stages of breast cancer have used CPM as an
integral component. In the liver, CPM undergoes metabolic
activation to form phosphoramide mustard and acrolein (2). Phosphoramide mustard is believed to
produce interstrand cross-links between the N7-position of guanines
on opposite DNA strands, which are considered to be the major
cytotoxic lesions. Previous studies have indicated that acrolein,
and not phosphoramide mustard, is the mutagenic/toxic metabolite of
CPM, with MGMT being involved in its repair (31). The association between MGMT
expression and the resistance to CPM has been debated (32). It is clear that drug resistance in
cancer is a multifactorial process. High intracellular aldehyde
dehydrogenase activity is reported to be an important determinant
of CPM sensitivity (33). The
decreased expression or mutation of p53 has also been associated
with chemoresistance (34). Other
postulated mechanisms of resistance include the increased
expression of the glutathione S-transferase group of enzymes,
resulting in an increased deactivation of potentially damaging
metabolites of CPM and a depletion of cellular glutathione
(32). These various mechanisms
possibly operate simultaneously, and the precise contribution of
each is thus difficult to define.
Finally, the present study demonstrated that the
MGMT expression level and improvement in clinical outcomes are
significantly correlated among patients with basal-like breast
cancers who receive CPM-containing adjuvant chemotherapy. At
present, the exact reasons why MGMT protein expression affects
CPM-containing chemotherapy in these patients are not known. As
Lehmann et al (35) reported
two different subtypes of basal-like breast cancer using gene
expression analysis, our future studies will focus on elucidating
the role of MGMT in the anti-tumor effect and toxicity of CPM, and
identifying a subset of basal-like breast cancer that exhibits
sensitivity to CPM.
Acknowledgements
The authors would like to express their gratitude to
Professor Tetsuya Mitsudomi at the Department of Surgery, Faculty
of Medicine, Kinki University (Japan), for providing valuable
advice and encouragement. The authors also wish to thank Fusako
Kamata for supplying technical assistance.
References
|
1
|
Pegg A: Multifaceted roles of
alkyltransferase and related proteins in DNA repair, DNA damage,
resistance to chemotherapy, and research tools. Chem Res Toxicol.
24:618–639. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Colvin M and Hilton J: Pharmacology of
cyclophosphamide and metabolites. Cancer Treat Rep. 65(Suppl 3):
89–95. 1981.
|
|
3
|
Mattern J, Eichhorn U, Kaina B and Volm M:
O6-methylguanine-DNA methyltransferase activity and sensitivity to
cyclophosphamide and cisplatin in human lung tumor xenografts. Int
J Cancer. 77:919–922. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
D’Incalci M, Bonfanti M, Pifferi A, et al:
The antitumour activity of alkylating agents is not correlated with
the levels of glutathione, glutathione transferase and
O6-alkylguanine-DNA-alkyltransferase of human tumour xenografts.
EORTC SPG and PAMM Groups. Eur J Cancer. 34:1749–1755. 1998.
|
|
5
|
Ohno T, Hiraga J, Ohashi H, et al: Loss of
O6-methylguanine-DNA-methyltransferase protein expression is a
favorable prognostic marker in diffuse large B-cell lymphoma. Int J
Hematol. 83:341–347. 2006. View Article : Google Scholar
|
|
6
|
Hansen RJ, Ludeman SM, Paikoff SJ, et al:
Role of MGMT in protecting against cyclophosphamide-induced
toxicity in cells and animals. DNA repair (Amst). 6:1145–1154.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cayre A, Penault-Llorca F, De Latour M, et
al: O(6)-methyguanine-DNA methyl transferase gene expression and
prognosis in breast carcinoma. Int J Oncol. 21:1125–1131.
2002.PubMed/NCBI
|
|
8
|
Nakai K, Mitomi H, Alkam Y, et al:
Predictive value of MGMT, hMLH1, hMSH2 and BRCA1 protein expression
for pathological complete response to neoadjuvant chemotherapy in
basal-like breast cancer patients. Cancer Chemother Pharmacol.
69:923–930. 2012. View Article : Google Scholar
|
|
9
|
Esteller M, Hamilton SR, Burger PC, et al:
Inactivation of the DNA repair gene O6-methylguanine-DNA
methyltransferase by promoter hypermethylation is a common event in
primary human neoplasia. Cancer Res. 59:793–797. 1999.PubMed/NCBI
|
|
10
|
Wani G and D’Ambrosio SM: Expression of
the O6-alkylguanine-DNA alkyltransferase gene is elevated in human
breast tumor cells. Anticancer Res. 17:4311–4315. 1997.PubMed/NCBI
|
|
11
|
Citron M, Schoenhaus M, Rothenberg H, et
al: O6-methylguanine-DNA methyltransferase in normal and malignant
tissue of the breast. Cancer Invest. 12:605–610. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Osanai T, Takagi Y, Toriya Y, et al:
Inverse correlation between the expression of O6-methylguanine-DNA
methyl transferase (MGMT) and p53 in breast cancer. Jpn J Clin
Oncol. 35:121–125. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Matsukura S, Miyazaki K, Yakushiji H, et
al: Expression and prognostic significance of O6-methylguanine-DNA
methyltransferase in hepatocellular, gastric, and breast cancers.
Ann Surg Oncol. 8:807–816. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Neto JC, Ikoma MM, Carvalho KC, et al:
MGMT and PTEN as potential prognostic markers in breast cancer. Exp
Mol Pathol. 92:20–26. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Clemons MJ, Bibby MC, El Teraifi H, et al:
Heterogeneity of O6-alkylguanine-DNA-alkyltransferase expression in
human breast tumours. Br J Cancer. 86:1797–1802. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Perou CM, Sørlie T, Eisen MB, et al:
Molecular portraits of human breast tumours. Nature. 406:747–752.
2000. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sørlie T, Perou CM, Tibshirani R, et al:
Gene expression patterns of breast carcinomas distinguish tumor
subclasses with clinical implications. Proc Natl Acad Sci USA.
98:10869–10874. 2001.PubMed/NCBI
|
|
18
|
Prat A, Ellis MJ and Perou CM: Practical
implications of gene-expression-based assays for breast
oncologists. Nat Rev Clin Oncol. 9:48–57. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fumagalli C, Pruneri G, Possanzini P, et
al: Methylation of O6-methylguanine-DNA methyltransferase (MGMT)
promoter gene in triple-negative breast cancer patients. Breast
Cancer Res Treat. 134:131–137. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wolff AC, Hammond ME, Schwartz JN, et al:
American Society of Clinical Oncology/College of American
Pathologists guideline recommendations for human epidermal growth
factor receptor 2 testing in breast cancer. J Clin Oncol.
25:118–1145. 2007. View Article : Google Scholar
|
|
21
|
Livasy CA, Karaca G, Nanda R, et al:
Phenotypic evaluation of the basal-like subtype of invasive breast
carcinoma. Modern Pathol. 19:264–271. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim MJ, Ro JY, Ahn SH, et al:
Clinicopathologic significance of the basal-like subtype of breast
cancer: a comparison with hormone receptor and
Her2/neu-overexpressing phenotypes. Hum Pathol. 37:1217–1226. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Nakasu S, Fukami T, Baba K and Matsuda M:
Immunohistochemical study for O6-methylguanine-DNA
methyltransferase in the non-neoplastic and neoplastic components
of glioma. J Neurooncol. 70:333–340. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Carey LA, Perou CM, Livasy CA, et al:
Race, Breast Cancer subtypes, and survival in the Carolina Breast
Cancer Study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Munot K, Bell SM, Lane S, et al: Pattern
of expression of genes linked to epigenetic silencing in human
breast cancer. Hum Pathol. 37:989–999. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sharma G, Mirza S, Parshad R, et al:
Clinical significance of promoter hypermethylation of DNA repair
genes in tumor and serum DNA in invasive ductal breast carcinoma
patients. Life Sci. 87:83–91. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
O’Malley FP, Chia S, Tu D, et al:
Topoisomerase II alpha and responsiveness of breast cancer to
adjuvant chemotherapy. J Natl Cancer Inst. 101:644–650. 2009.
|
|
28
|
Colleoni M, Cole BF, Viale G, et al:
Classical cyclophosphamide, methotrexate, and fluorouracil
chemotherapy is more effective in triple-negative, node-negative
breast cancer: results from two randomized trials of adjuvant
chemoendocrine therapy for node-negative breast cancer. J Clin
Oncol. 28:2966–2973. 2010. View Article : Google Scholar
|
|
29
|
Falo C, Moreno A, Varela M, et al:
HER-2/neu ststus and response to CMF: retrospective study in a
series of operable breast cancer treated with primary CMF
chemotherapy. J Cancer Res Clin Oncol. 133:423–429. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Munzone E, Curigliano G, Burstein HJ, et
al: CMF revisited in the 21st century. Ann Oncol. 23:305–311. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cai Y, Wu MH, Ludeman SM, et al: Role of
O6-alkylguanine-DNA alkyltransferase in protecting against
cyclophosphamide-induced toxicity and mutagenicity. Cancer Res.
59:3059–3063. 1999.PubMed/NCBI
|
|
32
|
Gamcsik MP, Dolan ME, Andersson BS and
Murray D: Mechanisms of resistance to the toxicity of
cyclophosphamide. Curr Pharm Des. 5:587–605. 1999.PubMed/NCBI
|
|
33
|
Hilton J: Role of aldehyde dehydrogenase
in cyclophosphamide-resistance L1210 leukemia. Cancer Res.
44:5156–5160. 1984.PubMed/NCBI
|
|
34
|
Kirsch DG and Kastan MB: Tumor-suppressor
p53: implication for tumor development and prognosis. J Clin Oncol.
16:3158–3168. 1998.PubMed/NCBI
|
|
35
|
Lehmann BD, Bauer JA, Chen X, et al:
Identification of human triple-negative breast cancer subtypes and
preclinical models for selection of targeted therapies. J Clin
Invest. 121:2750–2767. 2011. View
Article : Google Scholar : PubMed/NCBI
|