Introduction
Endometrial polyps are localized overgrowths of the
endometrium, with histological features composed of the irregular
proliferation of glands and stroma, containing thick-walled blood
vessels and lined by pseudostratified or flat epithelium (1).
The prevalence of polyps ranges between 7.8 and
34.9%, depending on the method used for diagnosis and the study
population (2). Prevalence has been
found to increase with age and is higher in postmenopausal patients
compared with premenopausal patients (3).
The malignancy rate associated with endometrial
polyps is low, and in a recent meta-analysis on the oncogenic
potential of polyps, it was observed that the malignancy rate of
endometrial polyps ranged between 0.8 and 8% in the different
studies analyzed (4). In our
previous study, a higher occurrence of premalignant and malignant
polyps was observed in postmenopausal females aged over 60 years
with vaginal bleeding (5). Other
studies have also shown an association between malignancy and
certain risk factors, including obesity, arterial hypertension,
diabetes mellitus and tamoxifen use (4,6).
Hormonal factors appear to be present in the
pathogenesis of endometrial polyps, and estrogen and progesterone
are known modulators of endometrial proliferation and
differentiation by means of steroid receptors. Furthermore, the
development of polyps may be associated with higher receptor
expression in the glandular epithelium, which subsequently leads to
focal hyperplasia of the endometrium (7). Few studies with a limited number of
tissue samples have assessed the expression of these receptors in
endometrial polyps (8–10). In the glandular epithelium of
endometrial polyps, the immunohistochemical expression of the
estrogen receptor (ER) and progesterone receptor (PR) is higher
than that in the adjacent endometrium. However, in the stromal
component of the endometrial polyps, only ER expression is higher
than in the adjacent endometrium. The same is not observed with PR
(8).
Despite a low prevalence of malignancy in
endometrial polyps, the role of ER and PR expression in the
mechanisms of carcinogenesis remains unknown. No data evaluating
these receptors in malignant polyps exists in the literature and
therefore, we hypothesized that there may be a difference in the
receptor expression between malignant and benign polyps.
The aim of the present study was to evaluate ER and
PR expression in the glandular epithelium and stroma of malignant
and benign polyps in postmenopausal patients.
Materials and methods
Patients
The present study was conducted at the Professor Dr.
José Aristodemo Pinotti Women’s Hospital (Center for Integral
Attention to Women’s Health) of the State University of Campinas
(UNICAMP; Campinas, Brazil). Approval was obtained from the
Research Ethics Committee of the UNICAMP School of Medicine
(769/2009), additionally the ethics committee waived the
requirement for patient consent. According to information stored in
the computerized database of this institution, 6,018 surgical
hysteroscopies were performed between January 1998 and December
2008 for the diagnosis and treatment of diverse uterine conditions.
Of the females examined, 1,050 underwent surgical treatment of
endometrial polyps and of these, 508 were postmenopausal. Females
with no histological confirmation of endometrial polyps and users
of hormonal therapy and tamoxifen were excluded. As a result, 390
postmenopausal females, aged between 39 and 86 years and diagnosed
with endometrial polyps determined by ultrasound or diagnostic
hysteroscopy were included in this study. Menopause was defined as
amenorrhea that had lasted for >12 months.
Clinical, histopathological and hysteroscopic data
were retrieved from patient medical records and the following
clinical characteristics were observed: Age, postmenopausal
bleeding, time since menopause, parity, presence of arterial
hypertension, obesity, diabetes mellitus and history of breast
cancer.
Diagnostic hysteroscopy was performed using a 2.8-mm
optical system (Karl Storz GmbH and Co., KG, Tuttlingen, Germany),
and for distension of the uterine cavity, a CO2 and
saline infusion was used. Surgical hysteroscopy was performed by a
gynecologist with the patient under spinal anesthesia, and a 10-mm
resectoscope with a loop electrode was used for the surgical
procedure (Karl Storz GmbH and Co., KG). Distension of the uterine
cavity was obtained by administration of the 1.5% glycine solution,
prior to the evaluation of the endocervical channel and endometrial
cavity. Resection of the endometrial polyps was performed by
electrocautery using the monopolar mode of energy.
Pathologists from the Department of Pathological
Anatomy of the UNICAMP Medical School analyzed the endometrial
samples obtained, using hematoxylin and eosin (H&E) staining.
Polyps were then classified as benign, non-atypical simple
hyperplasia, non-atypical complex hyperplasia, atypical simple
hyperplasia, atypical complex hyperplasia or malignant.
Construction of tissue microarray
(TMA)
Initially, a pathologist from the Department of
Pathological Anatomy of the UNICAMP School of Medicine studied the
slides representative of endometrial polyps stained with H&E.
The two regions that best represented the stroma and glandular
epithelium were then selected for the construction of the TMA
following a technique validated for the endometrium (11). Subsequently, the selected regions
were identified in archival paraffin blocks (donor blocks). These
marked donor blocks were sent to the Laboratory of
Immunohistochemistry of the Division of Pathologic Anatomy of the
A.C. Camargo Cancer Center (São Paulo, Brazil) for the construction
of the receptor blocks using the TMA technique. A TMA (Beecher
Instruments Inc., Silver Springs, MD, USA), available at the
Department of Pathologic Anatomy at the A.C. Camargo Cancer Center,
was used. Cylinder cores measuring 1.0 mm from the region of
interest, which were obtained by the previously described
equipment, were transferred to a new block with a two-dimensional
layout and 0.2 mm spacing between the cores, then determined and
recorded. From this new block, termed the recipient TMA block,
histological sections were obtained using a manual microtome and
transferred by adhesive tape to special adhesive-coated slides
(Instrumentics, Inc., Hackensack, NJ, USA). The adhesive tape was
then removed under exposure to ultraviolet light. Next, the
sections were stored, paraffin-embedded, vacuum-packed and frozen
at −20°C.
Immunohistochemistry
ER and PR expression was evaluated at the Laboratory
of Immunohistochemistry of the Department of Pathology of the
A.C.Camargo Cancer Center. The TMA sections were 5-μm thick and
deparaffinization was performed for 24 h at 60°C in an incubator.
Subsequently, the sections were rinsed in xylene at 60°C for 20 min
and at room temperature for 20 min, followed by rinsing with 100%
ethanol for 30 sec, 85% ethanol for 30 sec and 70% ethanol for 30
sec. The sections were then washed under distilled running
water.
A 10 mM citrate buffer solution (pH 6.0) was heated
to boiling point in a pressure cooker without sealing the lid
(Eterna®; Nigro Aluminium Ltd., São Paulo, Brazil). The
slides were then immersed and the lid was sealed with the safety
valve in open position. Following the release of the saturated
vapor, the safety valve was lowered until total pressurization was
reached. The timing was started once the pressure indicator valve
had reached the maximum point (~4 min). The pressure cooker
remained closed under running water until total depressurization.
The lid of the cooker containing the slides was then opened and the
slides were washed in distilled running water.
Endogenous peroxidase was blocked with 3% hydrogen
peroxide [H2O2 (10 vol)] with three changes
of 10 min each. The sections were then washed in distilled running
water and 10 mM phosphate-buffered saline [PBS (pH 7.4)] for 5
min.
Next, the slides were incubated with primary
antibody diluted in a predefined titer in PBS buffer containing 1%
bovine serum albumin (A9647; Sigma-Aldrich, St. Louis, MO, USA) and
0.1% sodium azide for 18 h in a humidity chamber at 4°C. The
procedure used primary monoclonal antibodies against ER (M7047;
clone 1D5; 1:250) and PR (M3569; clone PgR 636; 1:500)
(Dako®, Carpinteria, CA, USA).
The slides were washed with three changes of PBS
buffer for 3 min each and incubated for 30 min at 37°C with the
Advance™ horseradish peroxidase (HRP)-linked secondary antibody
(K4068; Dako). The slides were washed again with three changes of
PBS buffer for 3 min each and then incubated with the Advance HRP
enzyme for 30 min at 37°C. Following a final washing with three
changes of PBS buffer for 3 min each, the slides were incubated in
the following substrate solution: 100 mg
3,3′-diaminobenzidine-tetrahydrochloride (D-5637; Sigma-Aldrich), 1
ml dimethyl sulfoxide, 1 ml 6% H2O2 (20 vol)
and 100 ml PBS for 5 min at 37°C, protected from light. Next, the
slides were washed in distilled running water for 3 min and
counterstained with Harris’ hematoxylin for 1 min, followed by a
final thorough washing in distilled running water. The slides were
then immersed twice into ammoniacal water (0.5% ammonium hydroxide
solution) and washed in distilled running water. The sections were
dehydrated in the following solutions: 80% ethanol for 30 sec, 95%
ethanol for 30 sec, 100% ethanol twice for 30 sec each and xylene
four times for 30 sec each. The slides were then mounted on
Entellan neu (1.07961; Merck, Darmstadt, Germany) and on
microscopy, a final reaction product was observed as a golden brown
precipitate, varying according to the type of marker.
Immunohistochemical analysis
Hormonal receptors (ER and PR)
The TMA slides were read manually by only one
pathologist using conventional light microscopy (Zeiss AxioPhot
microscope, Carl Zeiss Microscopy, LLC, Thornwood, NY, USA). ER and
PR expression was evaluated in the stroma and glandular epithelium
of the polyp tissues using a semi-quantitative method of nuclear
reaction through analysis of the percentage of stained cells, the
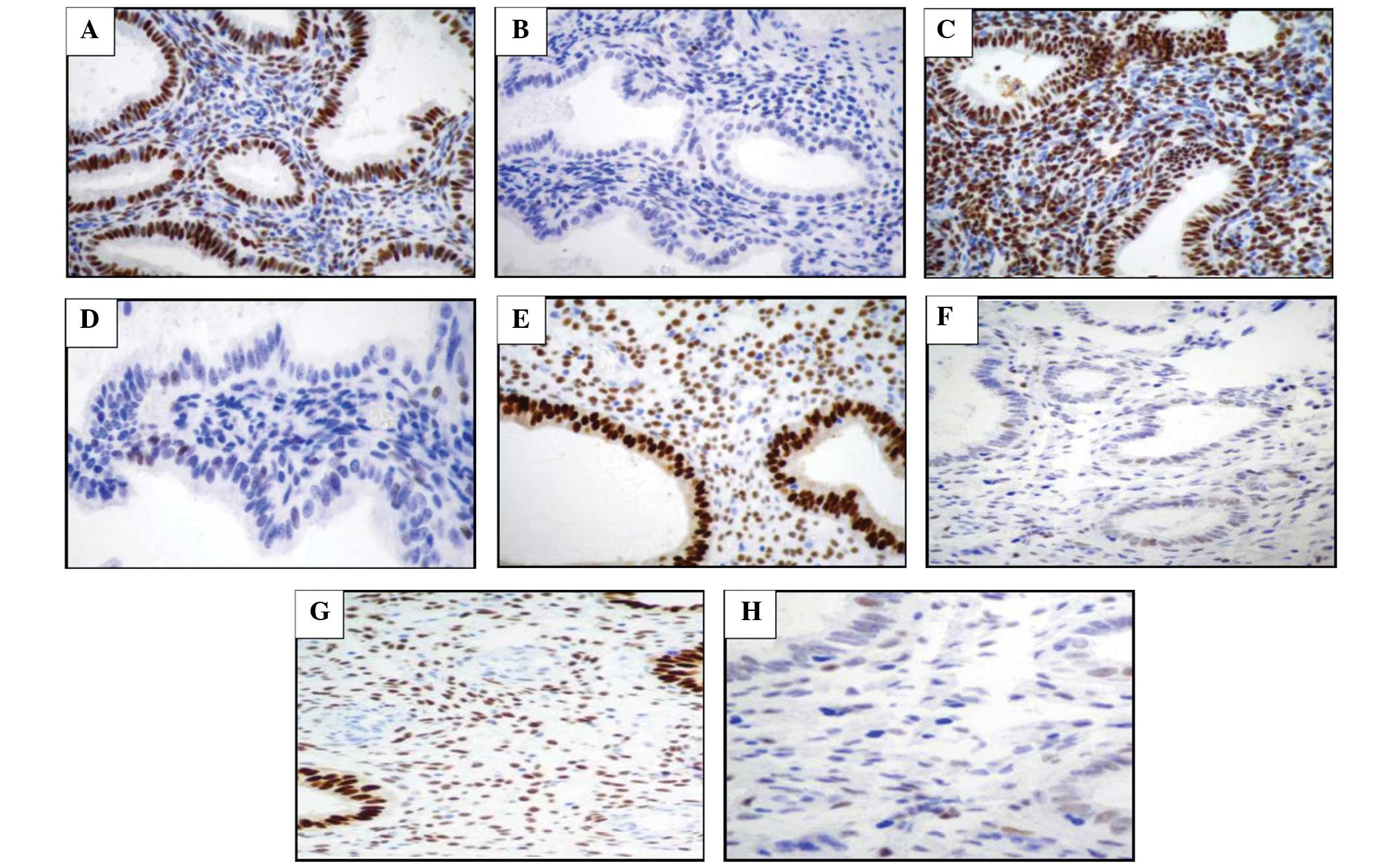
intensity of nuclear staining and the final score (12). The percentage of stained cells was
visually estimated and categorized as follows: Grade 0, no
staining; grade 1, <1% staining; grade 2, 1–10% staining; grade
3, 11–33% staining; grade 4, 34–66% staining; and grade 5, >66%
staining. With regard to the intensity of nuclear staining, the
staining was categorized as follows: Grade 0, negative; grade 1,
weak reaction; grade 2, moderate reaction; and grade 3, intense
reaction (12). The sum of
positivity and intensity resulted in a final score that ranged
between 0 and 8 (excluding value 1) (Fig. 1).
Statistical analysis
For statistical analysis, the polyps were grouped as
benign (including polyps of the endometrial mucosa and polyps with
non-atypical simple hyperplasia or non-atypical complex
hyperplasia) or premalignant/malignant (including polyps with
atypical simple hyperplasia or atypical complex hyperplasia and
carcinomatous polyps). Clinical characteristics between the groups
of benign and malignant polyps were compared using the
χ2, Fisher’s exact or Mann-Whitney non-parametric tests.
To compare the final scores of ER and PR expression in the
glandular epithelium and stroma of the polyps, a final score of ≤2
was considered a negative reaction and a final score of ≥3 was
considered a positive reaction. This comparison was made using
Fisher’s exact test and the χ2 test. A combination of
ER/PR expression in the glandular epithelium and stroma of the
endometrial polyps in comparison to the malignant and benign
lesions was calculated using Fisher’s exact test. The Statistical
Analysis System program, version 9.2 (SAS Institute Inc., Cary, NC,
USA) was used for these calculations. P<0.05 was considered to
indicate a statistically significant difference.
Results
Histological diagnosis
Table I shows the
histological diagnosis of resected lesions. In total, 362 benign
lesions were diagnosed (92.82%), including 313 endometrial
(80.26%), 41 non-atypical simple hyperplasia (10.5%) and eight
non-atypical complex hyperplasia (2.05%) polyps. The premalignant
lesions consisted of five polyps with atypical simple hyperplasia
(1.28%) and three polyps with atypical complex hyperplasia (0.76%).
In addition, 20 malignant polyps (5.11%) were diagnosed. Among the
malignant polyps, endometrioid adenocarcinoma was the histological
type of the majority. However, one case with less-differentiated
endometrial carcinoma and an additional case with serous
endometrial cancer were observed.
 | Table IHistological diagnosis of endometrial
polyps in postmenopausal patients. |
Table I
Histological diagnosis of endometrial
polyps in postmenopausal patients.
| Histological
diagnosis | n | % |
|---|
| Benign |
| Endometrial
polyp | 313 | 80.25 |
| Polyp without
atypical simple hyperplasia | 41 | 10.51 |
| Polyp without
atypical complex hyperplasia | 8 | 2.05 |
| Subtotal | 362 | 92.82 |
|
Premalignant/malignant |
| Polyp with atypical
simple hyperplasia | 5 | 1.28 |
| Polyp with atypical
complex hyperplasia | 3 | 0.76 |
| Polyp with
endometrioid adenocarcinoma | 18 | 4.61 |
| Polyp with
less-differentiated endometrial carcinoma | 1 | 0.25 |
| Polyp with serous
endometrial cancer | 1 | 0.25 |
| Subtotal | 28 | 7.17 |
| Total | 390 | 100 |
Clinical characteristics of
postmenopausal patients
The mean age of the females with benign polyps was
61.7±7.8 years (mean ± standard deviation) and 64.4±10.4 years for
those with malignant polyps. No significant difference was
identified in the mean age at menopause between the two groups
(48.9±7.5 vs. 50.4±4.8; P=0.236). Table II shows a comparison of the
clinical characteristics of the patients studied. No differences
associated with the presence of comorbid disorders, including
arterial hypertension, diabetes mellitus, breast cancer, obesity
and parity, were identified among the females with benign and
premalignant/malignant polyps. However, the presence of
postmenopausal bleeding was significantly greater in females with
premalignant/malignant polyps (P=0.0015; Table II).
| Table IIClinical characteristics of
postmenopausal patients with benign and malignant endometrial
polyps, and the prevalence of malignancy (n=390). |
Table II
Clinical characteristics of
postmenopausal patients with benign and malignant endometrial
polyps, and the prevalence of malignancy (n=390).
| Benign |
Premalignant/malignant | |
|---|
|
|
| |
|---|
| Characteristics | n | % | n | % | P-value |
|---|
| Age, years | | | | | 0.8549a |
| <40 | 1 | 100.0 | 0 | 0.0 | |
| 40–59 | 153 | 93.3 | 11 | 6.7 | |
| ≥60 | 207 | 92.4 | 17 | 7.6 | |
| Postmenopausal
bleeding | | | | | 0.0015b,c |
| Yes | 143 | 87.7 | 20 | 12.3 | |
| No | 210 | 96.3 | 8 | 3.7 | |
| Subarachnoid
hemorrhage | | | | | 0.1847b |
| Yes | 254 | 91.7 | 23 | 8.3 | |
| No | 107 | 95.5 | 5 | 4.5 | |
| Diabetes
mellitus | | | | | 0.2323b |
| Yes | 103 | 90.4 | 11 | 9.6 | |
| No | 257 | 93.8 | 17 | 6.2 | |
| Breast cancer | | | | | 0.6661a |
| Yes | 20 | 90.9 | 2 | 9.1 | |
| No | 341 | 92.9 | 26 | 7.1 | |
| Body mass
index | | | | | 0.0721b |
| <30 | 150 | 95.5 | 7 | 4.5 | |
| ≥30 | 204 | 90.7 | 21 | 9.3 | |
| Parity | | | | | 0.7098a |
| Nulliparous | 28 | 96.6 | 1 | 3.4 | |
| Multiparous | 331 | 92.5 | 27 | 7.5 | |
ER and PR expression
By comparing the final ER and PR score between the
benign and premalignant/malignant polyps, only the final score of
ER expression in the stroma of the endometrial polyps was observed
to be higher in the benign polyps compared with the premalignant
and malignant polyps, and showed a statistically significant
difference (Table III).
| Table IIIFinal ER/PR score in benign and
malignant polyps of postmenopausal patients (n=390). |
Table III
Final ER/PR score in benign and
malignant polyps of postmenopausal patients (n=390).
| Final score | Benign (n=362),
% |
Premalignant/malignant (n=28), % | P-value | OR (95% CI) |
|---|
| ER gland
(n=381) | | | 0.5721a | |
| Positive | 85.6 | 81.5 | | 1.0 |
| Negative | 14.4 | 18.5 | | 1.4
(0.49–3.73) |
| ER stroma
(n=384) | | | 0.0024a,b | |
| Positive | 82.9 | 59.3 | | 1.0 |
| Negative | 17.1 | 40.7 | | 3.3
(1.48–7.54)b |
| PR gland
(n=379) | | | 0.7089c | |
| Positive | 93.4 | 92.9 | | 1.0 |
| Negative | 6.6 | 7.1 | | 1.1
(0.24–4.91) |
| PR stroma
(n=381) | | | 0.1004c | |
| Positive | 89.8 | 77.8 | | 1.0 |
| Negatives | 10.2 | 22.2 | | 1.4
(0.56–3.30) |
In addition, by comparing the combined expression of
ER/PR, the risk of malignancy in the polyps was observed to be
significantly higher when the expression of the two receptors was
negative (ER−/PR−) in the stroma of the
endometrial polyps (odds ratio, 6.5; 95% confidence interval,
2.05–20.29). However, no significant difference was identified in
the glandular epithelium (Table
IV).
| Table IVComparison of the combined final
ER/PR score in benign and malignant polyps of postmenopausal
patients (n=390). |
Table IV
Comparison of the combined final
ER/PR score in benign and malignant polyps of postmenopausal
patients (n=390).
| Final ER/PR
score | Benign (n=362),
% |
Premalignant/malignant (n=28), % | P-valuea | OR (95% CI) |
|---|
| ER/PR gland
(n=372) | | | 0.2269 | |
|
ER+/PR+ | 96.3 | 90.9 | | 1.0 |
|
ER+/PR− | 3.7 | 9.1 | | 2.6
(0.54–12.58) |
|
ER−/PR+ | 76.6 | 100.0 | | 2.0
(0.70–5.64) |
|
ER−/PR− | 23.4 | 0.0 | | 0.6
(0.03–10.72) |
| ER/PR stroma
(n=375) | | | 0.0055b | |
|
ER+/PR+ | 93.1 | 93.3 | | 1.0 |
|
ER+/PR− | 6.9 | 6.7 | | 1.0
(0.12–7.74) |
|
ER−/PR+ | 74.1 | 54.5 | | 2.7
(0.98–7.41) |
|
ER−/PR− | 25.9 | 45.5 | | 6.5
(2.05–20.29) |
Discussion
The present study was conducted to evaluate ER and
PR expression in malignant and benign endometrial polyps of
postmenopausal patients. The results indicated that malignant
polyps exhibit a lower glandular and stromal ER expression than
benign polyps, however, PR expression was not found to correlate
with malignancy.
To the best of our knowledge, the present study
concerning ER and PR expression in postmenopausal patients is the
largest case study to have evaluated an association with
malignancy. The prevalence of malignancy in the sample studied was
7.1%, and postmenopausal bleeding was the only clinical parameter
found to correlate with the risk of malignancy in the endometrial
polyps. In our previous study, a prevalence of 4.1% (13) was identified. These prevalence rates
are consistent with those identified in other studies, which have
shown a prevalence of malignancy ranging between 0.8 and 8.0%
(14,15).
With regard to hormone receptor expression, the ER
and PR are specific nuclear receptors that belong to the steroid
receptor family. The activity of the ER is based on specific
regions of the gene and furthermore, the formation and
concentration of new receptors appear to be self-regulated and
dependent on hormonal factors (16). However, for progesterone, the tissue
expression of the PR has not been found to correlate with the
hormonal status found in postmenopausal patients, in which
progestational activity is not observed. In addition, the induction
of PR formation in the endometrium is mainly a consequence of
estrogen stimulation (17).
In the present study, the benign and
premalignant/malignant polyps were observed to exhibit a higher
expression of ER and PR in glandular cells than in stromal cells.
This higher glandular expression of the ER and PR has also been
observed in postmenopausal endometrial polyps when compared with
the atrophic endometrium (9) or
adjacent endometrium (7,8,18).
Other studies have also demonstrated that polyps in postmenopausal
females exhibit increased ER expression in the stroma and glandular
epithelium compared with polyps in premenopausal females (10,19).
However, PR expression is higher only in the glandular epithelium,
with no difference in expression identified in the stroma (19).
Few previous studies have investigated the
pathogenesis of endometrial polyps in detail, however, the present
study is the first to compare the ER and PR expression between
benign and malignant cases. The benign polyps were found to show
higher ER expression in the glandular epithelium and stroma.
However, no difference was identified with regard to PR when
compared with the premalignant/malignant polyps. This appears to
indicate that benign polyps in postmenopausal patients may respond
to an increased number of receptors, as a consequence of low
estrogen levels during the menopause. In addition, high expression
in the glandular epithelia indicates a higher sensitivity of these
structures to steroid hormones, which may be responsible for the
development of benign polyps in the presence of low serum estrogen
levels, while malignant polyps appear to be developed by a
different etiology.
In contrast to the high ER and PR expression
observed in benign endometrial polyps, one study has demonstrated
that the loss of steroid receptors is an early event in endometrial
carcinogenesis, and that endometrial carcinoma usually exhibits a
lower level of ER and PR than the normal endometrium or in
endometrial hyperplasia (20).
These observations indicate that the development of benign and
carcinomatous polyps may follow distinct pathways. By contrast, the
majority of studies show that estrogen promotes endometrial
carcinogenesis directly by stimulating the rapid proliferation of
epithelial cells. In addition, high ER expression is observed in
hyperplasia and carcinoma in populations of stromal and epithelial
cells (21–23).
According to the literature, ER and PR expression
may be lower in more advanced tumors and less-differentiated
tumors, which is a factor of worse prognosis (22,23).
In the present study, the presence of serous carcinoma and
less-differentiated carcinoma may have contributed to a decrease in
ER expression in the group of premalignant/malignant polyps. In
addition, when the expression of the two receptors (ER/PR) was
negative a malignancy risk that was six times higher was observed.
Other studies have also demonstrated that steroid receptor
expression is not an independent prognostic factor for endometrial
cancer, and uncertainty remains as to the usefulness of determining
receptor expression in patients with endometrial neoplasms
(24,25). No previous study has evaluated these
receptors in malignant polyps for the comparison of results.
However, it may be inferred from these differences that the
pathways of carcinogenesis in endometrial polyps may be different
from those observed in endometrial cancer or may be similar to
neoplasms of worse prognosis.
Discrepancies with regard to the results of the
present study and the various studies in the literature may in part
be explained by variations in methodology, particularly differences
in the antibody specificity and dilutions used. The lack of
consensus in the criteria defined for the positivity and
semi-quantitative nature of the method may have also contributed to
the different results between studies, according to the criteria
used. An additional possible limitation is the small number of
premalignant/malignant polyps analyzed in the present case study,
which may have interfered with the capacity of statistical tests to
identify significant differences between the groups. However, it is
important to highlight the fact that the number of
premalignant/malignant polyps may be high, in view of the low
prevalence of malignancy associated with polyps.
In conclusion, the observations of the present study
have shown that polyps in postmenopausal patients have high ER
expression in the stroma and glandular epithelium. However, this
expression is lower in premalignant/malignant polyps compared with
benign polyps. These results indicate that lower ER expression may
be one more risk factor for the malignancy potential of polyps in
postmenopausal females. Polypectomy has been routinely indicated to
stop bleeding and to exclude malignancy. No tool is currently
available to make predictions of the malignancy of these lesions,
and histological evaluation of the resected polyp continues to be
the only form of diagnosing malignant cases. The usefulness of
measuring receptors in polyps remains questionable. The real
etiology of polyps and their mechanisms of carcinogenesis appear to
occur by different mechanisms that are currently unclear, but
remain necessary for the adequate management of endometrial
polyps.
References
|
1
|
Kurman RL: Blaustein’s Pathology of the
Female Genital Tract. 5th edition. Springer; New York: pp. 448–450.
2002
|
|
2
|
Haimov-Kochman R, Deri-Hasid R, Hamani Y
and Voss E: The natural course of endometrial polyps: Could they
vanish when left untreated? Fert Steril. 92:8282009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dreisler E, Stampe SS, Ibsen PH and Lose
G: Prevalence of endometrial polyps and abnormal uterine bleeding
in a Danish population aged 20–74 years. Ultrasound Obstet Gynecol.
33:102–108. 2009.
|
|
4
|
Lee SC, Kaunitz AM, Ramos LS and Rhatigan
RM: The oncogenic potential of endometrial polyps. A Systematic
Review and Meta-Analysis. Obstet Gynecol. 116:1197–1205. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Antunes A Jr, Costa-Paiva L, Arthuso M,
Costa JV and Pinto-Neto AM: Endometrial polyps in pre- and
postmenopausal women: factors associated with malignancy.
Maturitas. 57:415–421. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Oguz S, Sargin A, KeleKei S, Aytan H,
Tapisiz OL and Mollamahmutoglu L: The role of hormone replacement
therapy in endometrial polyp formation. Maturitas. 50:231–236.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lopes RG, Baracat EC, de Albuquerque Neto
LC, et al: Analysis of estrogen- and progesterone-receptor
expression in endometrial polyps. J Minim Invasive Gynecol.
14:300–303. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Almeida ECS, Nogueira AA, Reis FJC,
Ramalho LNZ and Zucoloto S: Immunohistochemical expression of
estrogen and progesterone receptors in endometrial polyps and
adjacent endometrium in postmenopausal women. Maturitas.
49:229–233. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Inceboz US, Nese N, Uyar Y, Ozcakir HT,
Kurtul O, Baytur YB, et al: Hormone receptor expressions and
proliferation markers in postmenopausal endometrial polyps. Gynecol
Obstet Invest. 61:24–28. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gul A, Ugur M, Iskender C, Zulfikaroglu E
and Ozaksit G: Immunohistochemical expression of estrogen and
progesterone receptors in endometrial polyps and its relationship
to clinical parameters. Arch Gynecol Obstet. 281:479–483. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fons G, Hasibuan SM, van der Velden J and
ten Kate FJ: Validation of tissue microarray technology in
endometrioid cancer of the endometrium. J Clin Pathol. 60:500–503.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Harvey JM, Clark GM, Osbome CK and Allred
DC: Estrogen receptor status by immunohistochemistry is superior to
the ligand-binding assay for predicting response to adjuvant
endocrine therapy in breast cancer. J Clin Oncol. 17:1474–1481.
1999.
|
|
13
|
Costa-Paiva L, Godoy CE Jr, Antunes A Jr,
Caseiro JD, Arthuso M and Pinto-Neto AM: Risk of malignancy in
endometrial polyps in premenopausal and postmenopausal women
according to clinicopathologic characteristics. Menopause. 18:1–5.
2011. View Article : Google Scholar
|
|
14
|
Anastasiadis PG, Koutlaki NG, Skaphida PG,
Galazios GC, Tsikouras PN and Liberis VA: Endometrial polyps:
prevalence, detection, and malignant potential in women with
abnormal uterine bleeding. Eur J Gynaecol Oncol. 21:180–183.
2000.PubMed/NCBI
|
|
15
|
Martinez MA, Jou P, Nonell R, Cardona M,
Alonso I and Vanrell JA: Endometrial polyps: risk of malignancy and
clinical-anatomical correlation. Prog Obstet Ginecol. 47:506–510.
2004.
|
|
16
|
Speroff L: The estrogen receptor: changing
concepts. Clinical lessons from molecular biology. Reproductive
Medicine - A Millennium Review. Coutinho EM and Spinola P:
Parthenon Publishing Group; New York: pp. 155–161. 1999
|
|
17
|
Yen SSC: Human menstrual cycle.
Reproductive Endocrinology: Physiology, Pathophysiology, and
Clinical Management. Yen SSC, Jaffe RB and Barbieri RL: Saunders;
Philadelphia: pp. 193–227. 1999
|
|
18
|
Longcope C and Baker S: Androgen and
estrogen dynamics: relationships with age, weight and menopausal
status. J Clin Endocrinol Metabol. 76:601–604. 1993.PubMed/NCBI
|
|
19
|
McGurgan P, Taylor LJ, Duffy SR and
O’Donovan PJ: Are endometrial polyps from pre-menopausal women
similar to post-menopausal women? An immunohistochemical comparison
of endometrial polyps from pre- and post-menopausal women.
Maturitas. 54:277–284. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pickartz H, Beckmann R, Fleige B, Due W,
Gerdes J and Stein H: Steroid receptors and proliferative activity
in non-neoplastic and neoplastic endometria. Virchows Arch A:
Pathol Anat Histopathol. 417:163–171. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Giuffre G, Arena F, Scarfi R, Simone A,
Todaro P and Tuccari G: Lactoferrin immunoexpression in endometrial
carcinomas: relationships with sex steroid hormone receptors (ER
and PR), proliferation indices (Ki-67 and AgNOR) and survival.
Oncol Rep. 16:257–263. 2006.
|
|
22
|
Moshin SK, Weiss H, Havighurst T, Clark
GM, Beraldo M, Roanhle D, et al: Progesterone receptor by
immunohistochemistry and clinical outcome in breast cancer: a
validation study. Mod Pathol. 17:1545–1554. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ito K, Utsunomiya H, Yaegashi N and Sasano
H: Biological roles of estrogen and progesterone in human
endometrial carcinoma-new developments in potential endocrine
therapy for endometrial cancer. Endocr J. 54:667–679. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Iversen OE, Utaaker E and Skaarland E: DNA
ploidy steroid receptors as predictors of disease course in
patients with endometrial carcinoma. Acta Obstet Gynecol Scand.
67:531–537. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sivridis E, Giatromanolaki A, Koukourakis
M and Anastasiadis P: Endometrial carcinoma: association of steroid
hormone receptor expression with low angiogenesis and bcl-2
expression. Virchows Arch. 438:470–477. 2001. View Article : Google Scholar : PubMed/NCBI
|