Introduction
Anaplastic thyroid carcinoma (ATC) is one of the
most aggressive endocrine tumors, with a high mortality rate. ATC
accounts for only 1–2% of all thyroid cancer and the mean age at
diagnosis is between 55 and 65 years (1–3). ATC
is a rare tumor that may metastasize to the skin in the context of
diffuse body metastases (4). By
contrast, cutaneous metastasis from differentiated thyroid
carcinoma is a rare manifestation of disseminated disease, while
the most common site of thyroid carcinoma skin metastases is the
scalp. Thoracic involvement is extremely rare. The metastatic
deposits usually present as flesh coloured nodules that are tender,
often itchy and which may ulcerate (3,4). Owing
to the relative rarity of this tumour, few treatment modalites are
available and the selection of treatment is largely made on
anecdotal evidence (2,4). ATC has a relatively negative prognosis
following diagnosis, with an average survival time of 4–12 months
(1,2).
The current study describes a case of anaplastic
thyroid cancer that presented with cervical lymph node metastasis
and exhibited diffuse skin metastases over a number of areas,
excluding the scalp, following treatment. The clinical,
radiological and pathological findings are presented. The patient
provided written informed consent.
Case report
A 57-year-old male presented to the Bağcılar
Training and Research Hospital (Istanbul, Turkey) due to difficulty
swallowing and swelling in the neck. The patient indicated a
previous diagnosis of goiter and had lost 3 kg of weight within the
previous 2 months. Laboratory assessments demonstrated normal
levels of free triiodothyronine, 2.38 pg/ml (ref, 2–4.4 pg/ml),
free thyroxine, 1.16 ng/dl (ref, 0.9–1.7), and thyroglobulin, 7.25
ng/ml (ref, 3–40 ng/ml), and a lower than normal level of
thyroid-stimulating hormone, 0.01 mU/l (ref, 0,35–5,5). The
sedimentation level was 11 mm for 30 min (ref, 0–5 h), 33 mm for 1
h (ref, 0–20) and was high overall. All other values were within
the normal ranges.
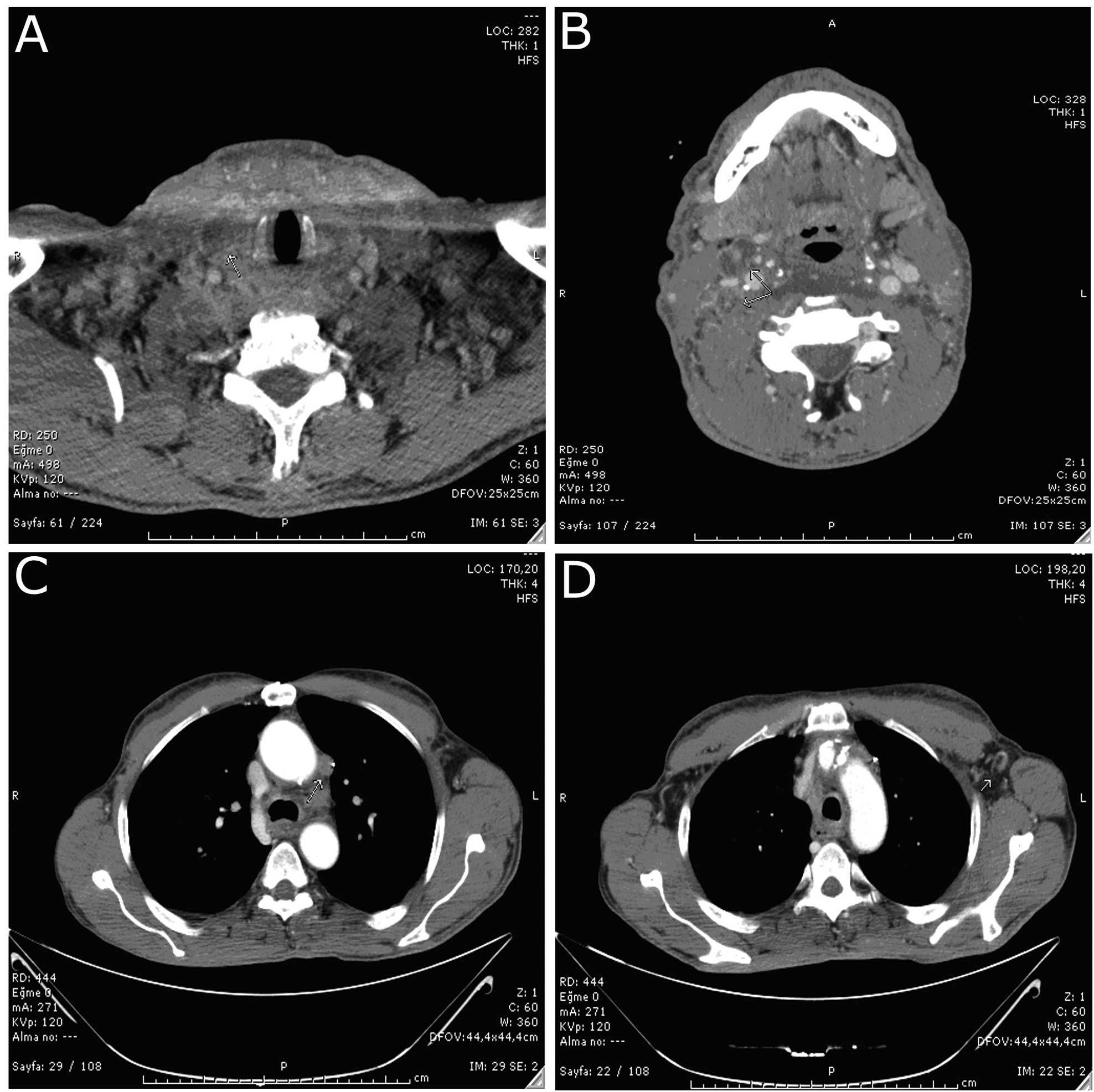
The neck computed tomography (CT) scan performed in
January 2012 exhibited a heterogeneous appearance, with an increase
in the size of the thyroid gland and marked parenchyma.
Lobular-contoured, centrally cystic-necrotic lymphadenopathies were
observed in the two jugular chains, with those in the right jugular
chain being more marked; the larger ones at a size of 2 cm and
others having a conglomerate appearance. Subcarinal, right
paratracheal, aortopulmonary, paraesophageal and left
tracheobranchial mediastinal lymphadenopathies were detected during
the thoracic CT, with the largest measuring 23 mm in diameter
(Fig. 1). Proximal esophageal
constriction was observed in association with extrinsic pressure
during the gastroscopy, which was applied due to the difficulty in
swallowing.
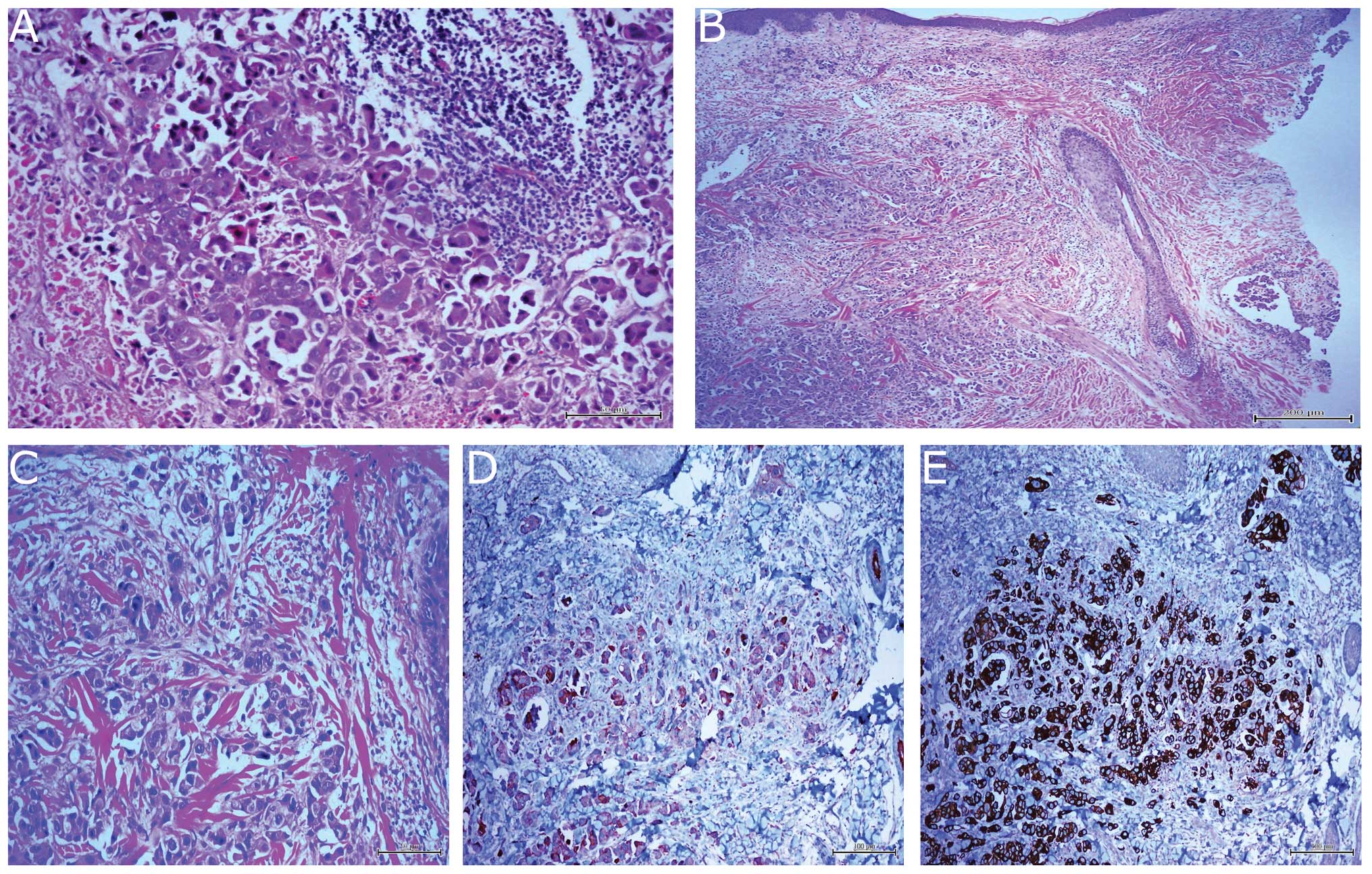
A fine-needle aspiration biopsy performed on a 20-mm
lymphadenopathy in the right jugular chain resulted in a sample
formed of large pleomorphic atypical epithelioid cells forming
flaccid clusters. The histopathological characteristics of the
Tru-Cut biopsy (Pro-Mag™ Ultra; PBN Medicals Denmark A/S, Stenløse,
Denmark) material, which was retrieved from the same mass, was a
match to the cytological aspirate (Fig.
2). The tumor cells showed positive immunoreactivity for
cytokeratin 7 (CK7) and galectin-3 in the immunohistochemical
staining, while exhibiting negative immunoreactivity for CK20,
thyroid transcription factor-1 (TTF-1) and human melanoma black-45.
In light of all these findings, the patient was diagnosed with a
metastatic anaplastic thyroid carcinoma.
Due to the extensive nature of the anaplastic
histology and lesions upon positron emission tomography (PET)/CT,
the patient was regarded to have advanced head-neck cancer, and
three cycles of doxorubicin (50 mg/m2) plus cisplatin
(40 mg/m2) for three weeks were subsequently
administered.
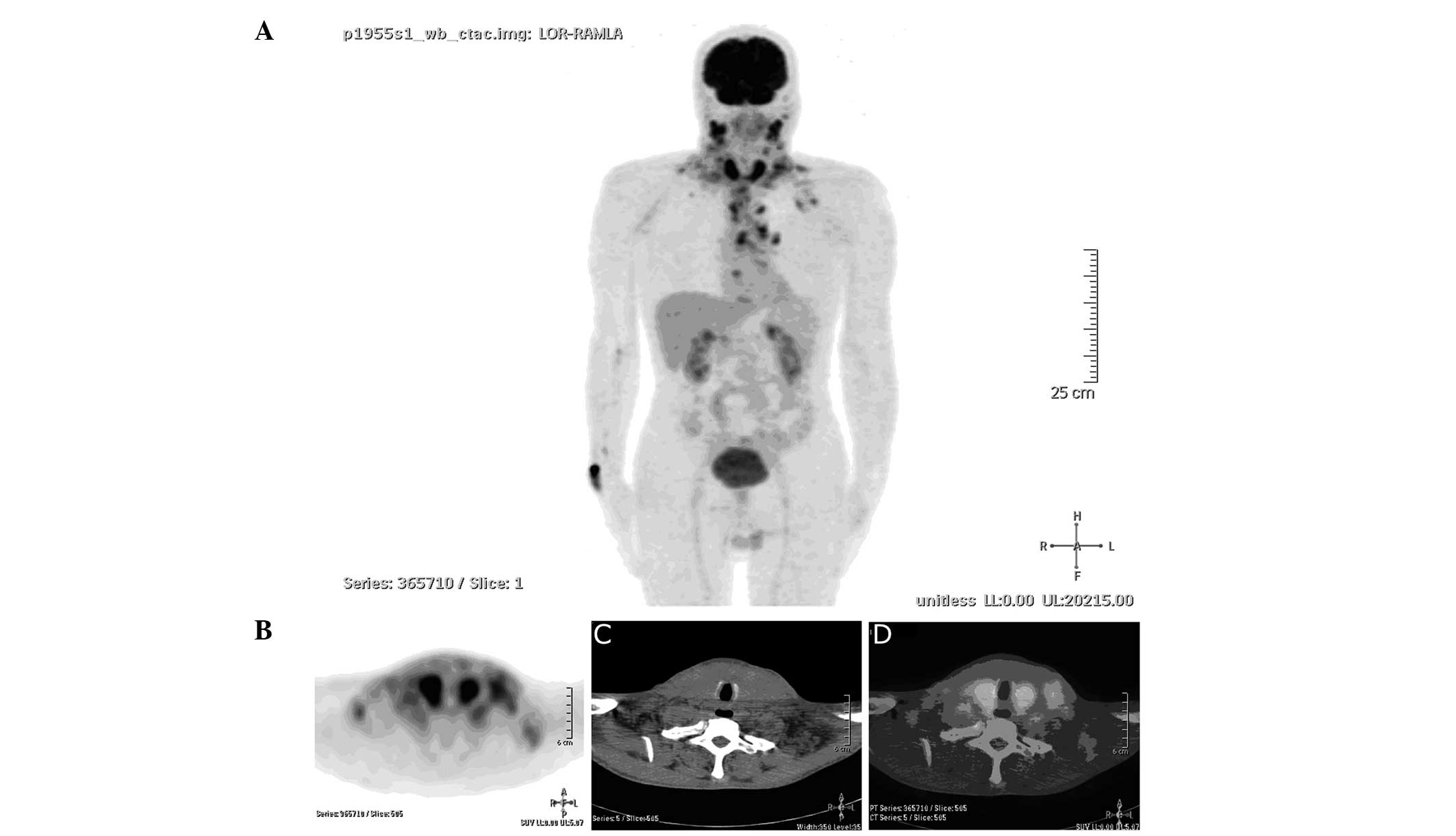
18F-fluorodeoxyglucose (FDG; 12.33 mCi)
was administered to the patient. PET/CT was subsequently performed
when the blood glucose level was 107 mg/dl following 8 h of fasting
for the assessment of the response to treatment after chemotherapy
and planning radiotherapy. Extremely intense FDG involvement was
observed in the two lobes of the thyroid, and a partial metabolic
response of metastatic character was observed in the hypermetabolic
lymphadenopathy in the neck, mediastinum and left axillary fossa
(Fig. 3).
Six cycles of chemotherapy (50 mg/m2
doxorubicin and 40 mg/m2 cisplatin for three weeks) were
administered upon the detection of anaplastic thyroid carcinoma
metastasis in the axillary lymphadenopathy material extracted in
April 2012. Palliative neck radiotherapy was applied up to a total
of 70 gy in 20 fractions.
Upon the completion of the treatment, diffuse,
painless, round to oval-shaped, purple to violet-colored skin
lesions that were fixed beneath the skin were noticed and began to
exhibit induration. The lesions appeared in the presternal and left
infraaxillary regions in the first month, then covered the left
front-lateral part of the thorax and extended to the left
infracostal border. The lesions were 3–4 cm in size and
occasionally formed plaques by merging (Fig. 4). Although the scalp is the most
common site of involvement (4), no
lesions were identified on the scalp of the current patient. The
histopathological and immunohistochemical findings of the skin
biopsy confirmed anaplastic thyroid carcinoma metastasis (Fig. 2). Consequently, the patient, who had
received 2 rounds of paclitaxel (2.5 mg/kg) plus carboplatin (360
mg/m2) therapy, succumbed to severe respiratory failure
1 month after the development of the metastatic skin lesions.
Discussion
Systemic metastases of thyroid cancers emerge during
the disease in 75% of patients and occur most frequently in the
lungs (80%), the bones (6–15%) and the brain (5–13%) (3). To date, ~50 cases have been reported
in association with primary thyroid cancer. A study by Dahl et
al (4) found that the most
frequent thyroid cancer to give rise to skin metastases was
papillary carcinoma, accounting for 41% of the cases, followed by
follicular carcinoma at 28%, and then anaplastic carcinoma and
medullary carcinoma each constituting 15% of the cases. By
contrast, Koller et al (5)
reported that follicular carcinoma has a greater preponderance for
cutaneous metastases than papillary carcinoma. Furthermore,
specific studies state that it is mostly papillary carcinomas that
result in metastasis (3,4). Anaplastic thyroid carcinoma is a rare
aggressive tumor that can lead to skin metastasis (6).
Skin metastases usually occur in the setting of
disseminated neoplastic disease, and the presence of cutaneous
metastases portends a poor prognosis. Skin metastasis typically
presents as slowly growing, solitary or multiple, erythematous,
flesh-colored, violaceous or blue-colored papules or nodules,
usually on the scalp, face or neck (5,6). Scalp
involvement was observed in 2/3 of patients in the study by Dahl
et al (4). Thoracic skin
involvement as observed in the present case is extremely rare.
Violaceous, multiple papillary-nodular eruptions appeared with
sudden onset and were diffused over the body, with different
localizations compared with previous studies. The most frequently
involved sites remained intact. However, the potential of skin
metastasis, considered upon the diagnosis of primary carcinoma, was
confirmed with histopathological assessment and immunohistochemical
staining. Although rarely observed at the onset of the disease,
skin metastases are generally observed in the advanced phases of
neoplasia and are indicators of a bad prognosis (5,6). In
the present case, the skin lesions appeared in the final phase in a
similar way to those in previous studies, and the patient succumbed
after a short 1-month period subsequent to their emergence
(4–6). This period was shorter compared with
the average survival period of 19 months (4), which has previously been indicated for
post-cutaneous metastasis in the literature. Thyroid cancers with
skin involvement may easily be confused with primary skin adnexial
tumors. TTF-1 is considered to be beneficial for distinguishing
carcinomas with pulmonary and thyroid immunohistochemistry from
other primary cancers, mesotheliomas and primary cutaneous Merkel
cell carcinomas (7).
The widest possible surgical approach may be applied
in resectable tumors; those with an absence of unilateral
extrathyroidal invasion at a diameter of <5 cm or those without
cervical lymph node involvement (8). Considering the radiological findings,
the patient of the present case had an advanced anaplastic
carcinoma and had no surgical options.
It has been reported that the combination of
doxorubicin and cisplatin is more effective compared with the
single use of doxorubicin in complete response (9). Skin lesions occurred pursuant to the
doxorubicin plus cisplatin therapy administered initially to the
present study patient, and paclitaxel therapy was initiated upon
the histopathological detection of ATC metastasis. Although this
was a promising option, as a response rate of 53% has been observed
previously (10), the patient did
not benefit from the treatment. Although the average survival rate
following cutaneous metastasis has been reported to be 19 months in
the literature (4), the present
patient succumbed to respiratory failure one month after the
occurrence of skin metastasis.
In conclusion, the present case was one of
anaplastic cancer, with skin metastasis emerging following
treatment and diffuse thoracic involvement, excluding the scalp, 10
months after the diagnosis. The present study demonstrated that the
possibility of metastatic thyroid cancer should be considered in
solid, multiple violaceous, blue-colored thoracic skin lesions, and
that metastatic thyroid carcinoma involving the skin can be
mistaken for primary skin tumors. Immunohistochemical stains should
be used in addition to the histopathological examination for the
differential diagnosis. External beam radiotherapy may be used as
an option for those patients who are not suitable for surgery or
full tumor removal.
References
|
1
|
Gilliland FD, Hunt WC, Morris DM and Key
CR: Prognostic factors for thyroid carcinoma. A population-based
study of 15,698 cases from the Surveillance, Epidemiology and End
Results (SEER) program 1973–1991. Cancer. 79:564–573.
1997.PubMed/NCBI
|
|
2
|
Are C and Shaha AR: Anaplastic thyroid
carcinoma: biology, pathogenesis, prognostic factors, and treatment
approaches. Ann Surg Oncol. 13:453–464. 2006. View Article : Google Scholar
|
|
3
|
Leonhardt JM and Heymann WR: Thyroid
disease and the skin. Dermatol Clin. 20:473–481. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dahl PR, Brodland DG, Goellner JR and Hay
ID: Thyroid carcinoma metastatic to the skin: a cutaneous
manifestation of a widely disseminated malignancy. J Am Acad
Dermatol. 36:531–537. 1997. View Article : Google Scholar
|
|
5
|
Koller EA, Tourtelot JB, Pak HS, Cobb MW,
Moad JC and Flynn EA: Papillary and follicular thyroid carcinoma
metastatic to the skin: a case report and review of the literature.
Thyroid. 8:1045–1050. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barr R and Dann F: Anaplastic thyroid
carcinoma metastatic to skin. J Cutan Pathol. 1:201–206. 1974.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lau SK, Luthringer DJ and Eisen RN:
Thyroid transcription factor-1: a review. Appl Immunohistochem Mol
Morphol. 10:97–102. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nel CJ, van Heerden JA, Goellner JR,
Gharib H, McConahey WM, Taylor WF and Grant CS: Anaplastic
carcinoma of the thyroid: a clinicopathologic study of 82 cases.
Mayo Clin Proc. 60:51–58. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shimaoka K, Schoenfeld DA, DeWys WD,
Creech RH and DeConti R: A randomized trial of doxorubicin versus
doxorubicin plus cisplatin in patients with advanced thyroid
carcinoma. Cancer. 56:2155–2160. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ain KB, Egorin MJ and DeSimone PA:
Treatment of anaplastic thyroid carcinoma with paclitaxel: phase 2
trial using ninety-six-hour infusion. Collaborative Anaplastic
Thyroid Cancer Health Intervention Trials (CATCHIT) Group. Thyroid.
10:587–594. 2000. View Article : Google Scholar : PubMed/NCBI
|