Introduction
Approximately 482,300 novel cases and 406,800
mortalities from esophageal cancer (EC) are reported annually
worldwide (1). EC is the sixth most
common cause of cancer mortality. The incidence of EC in China
accounts for 50% of cases worldwide, and the incidence of EC in
Henan province is >100/100,000 individuals. Although surgery,
radiotherapy, chemotherapy and biologically targeted therapies
continue to progress, the five-year survival rate for early EC
patients undergoing surgical treatment is ~30%. The reason for the
majority of failures is due to tumor recurrence (2–4). In
addition, the use of radiotherapy has been a focus of debate.
Therefore, the aim of the present study was to investigate the
pathological occurrence of squamous cell carcinoma by investigating
the pathological features of esophageal squamous cell carcinoma
using large sections. This may guide doctors to determine the
clinical target volume of radiotherapy, achieve a treatment for
cancer and reduce the radiation doses to the normal tissues in
order to improve a patient’s quality of life following
treatment.
Materials and methods
Clinical data
A total of 52 EC patients who underwent radical
resection in the Fourth Hospital of Hebei Medical University
(Shijiazhuang, China) between 2011 and 2012 were included in the
present study according to the following inclusion criteria:
Pre-operative lesion length on esophagography of >3 cm; complete
chest computed tomography (CT) scan, abdominal ultrasound and
conventional biochemical test records; and pathological
confirmation of squamous cell carcinoma. The 52 EC patients
consisted of 34 males (65.4%) and 18 females (34.6%), with a mean
age of 59 years (range, 26–73 years). The lesions were identified
in the upper thorax of six cases, the middle thorax of 40 cases and
the lower thorax of six cases. Esophageal imaging X-rays revealed a
mean lesion length of 5.8±1.4 cm (range, 3–10 cm). Three cases were
stage T2 and 49 cases were stage T3, 28 cases were stage N0 and 24
cases were stage N1, and 51 cases were stage M0 and one case was
stage M1. In addition, 29 cases were stage II, 22 cases were stage
III and one case was stage IV. TNM staging was determined according
to the Union for International Cancer Control (5). Patients provided written informed
consent. The study was approved by the ethics committee of The
Fourth Hospital of Hebei Medical University.
Detection methods and experimental
procedure
The lesions and esophagus-related indicators were
measured intraoperatively, and specimens were fixed for 24 h. The
tumor length, invasion depth and the distances between the upper
edge and the upper cutting edge of the tumor and between the lower
edge and the lower cutting edge were measured without tension
during surgery. The excised EC specimens were fixed with 10%
formalin solution for 24 h, and the length of the specimens and
invasion depths were measured. The types of tumor were identified
and recorded.
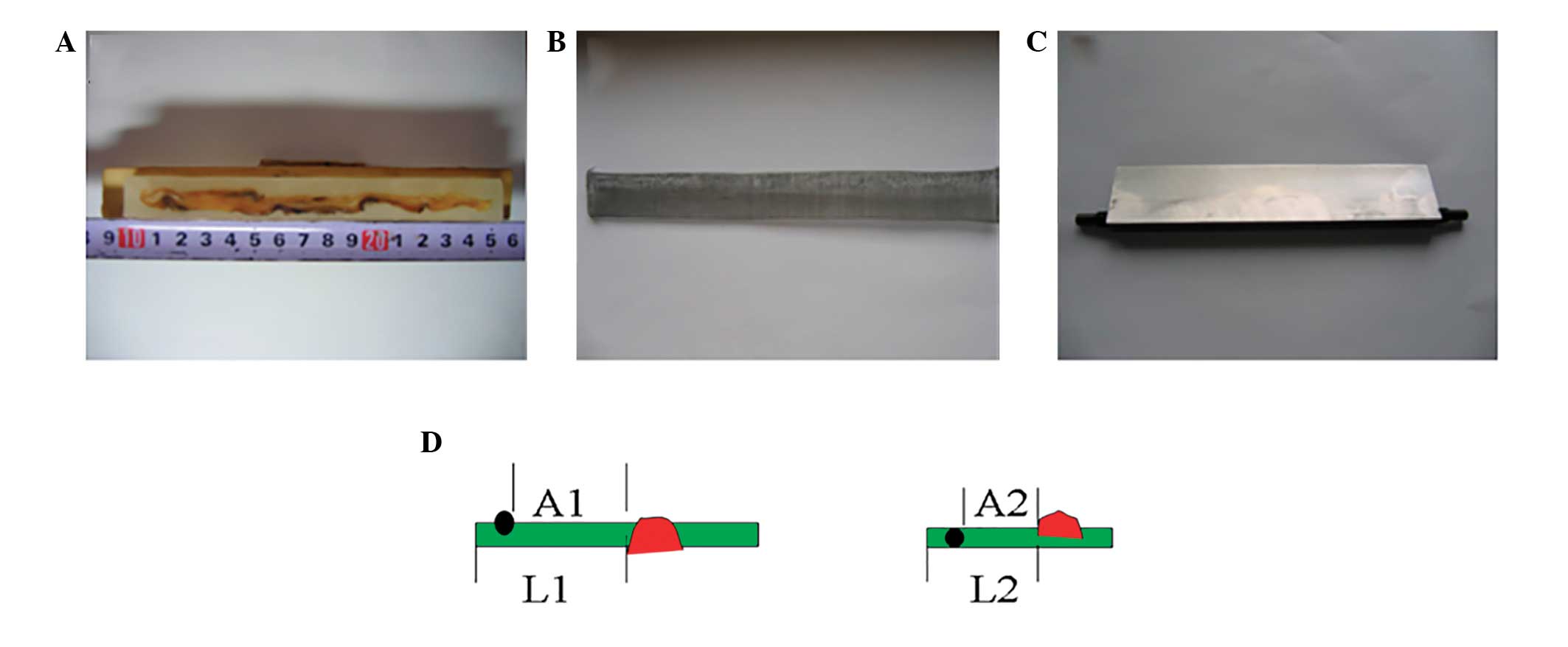
To produce the large sections for pathological
examination, 10% formaldehyde solution was used to fix specimens
for >24 h, and two 0.3-cm wide tissue blocks were obtained from
the fixed specimens. The tissue blocks contained the longest
longitudinal section and both sides of the excised esophagus. Gauze
(20 mesh) was used to produce the tissue boxes to avoid any
distortion in the process of section production.
Following dehydration, embedding, sectioning,
staining, dehydration transparency and cementing, the large
pathological sections were completed.
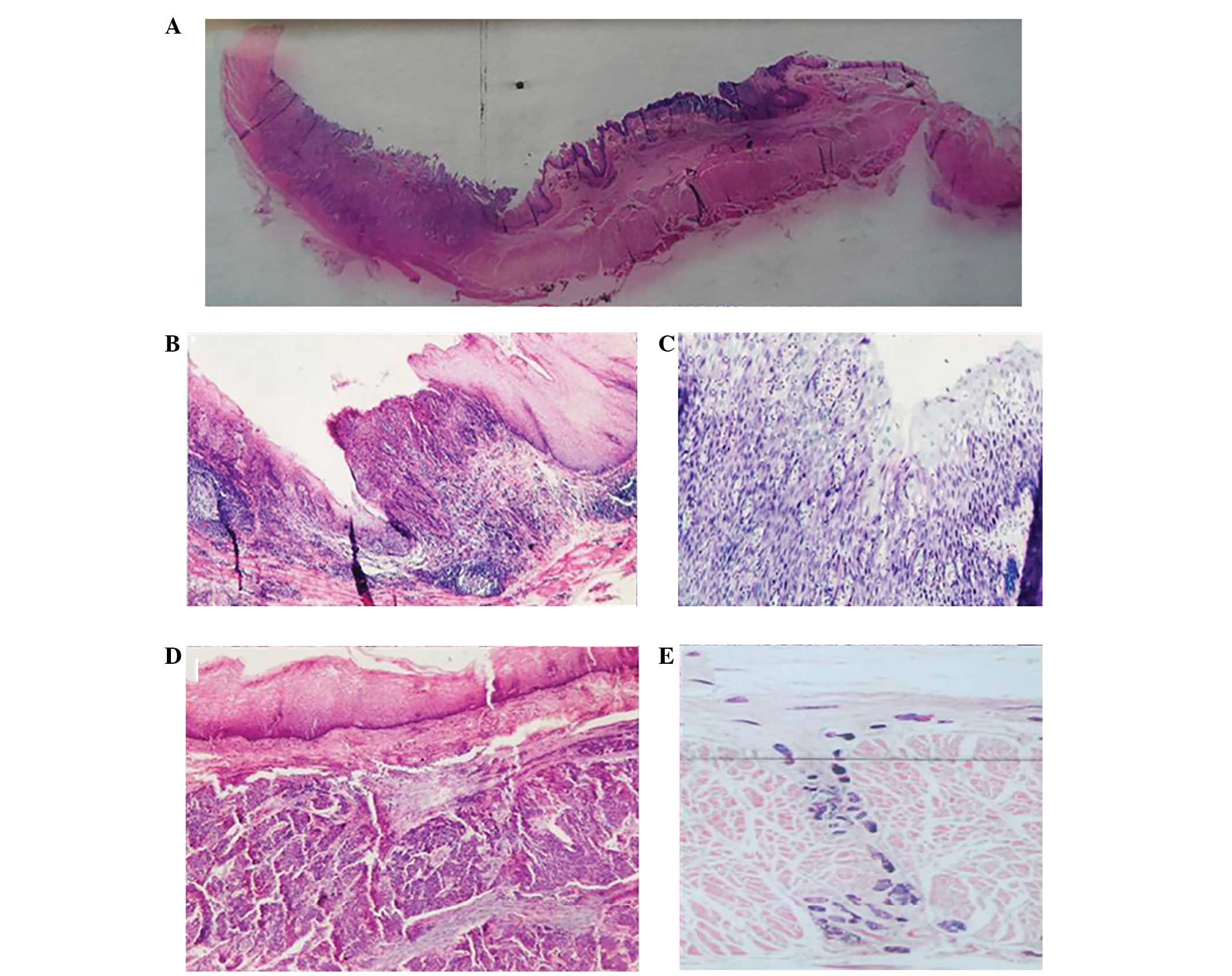
For the diagnosis and measurement of the associated
indicators, the sections were observed under a microscope to
identify the occurrence of multiple carcinogenic lesions (MLs),
severe dysplasia (SD), direct intramural infiltration (DI)
(Fig. 1), lymph node metastasis,
vascular invasion and lymphatic invasion.
The diagnostic criteria were as follows: ML, foci
separated from the main tumor exhibiting characteristics of
atypical hyperplasia carcinoma in situ or invasive
carcinoma; SD, undifferentiated atypical cells accounting for
>2/3 of the esophageal epithelial cell layer without breaking
through the underlying membrane; and DI, normal mucosal epithelial
lining of the esophagus with cancer submucosal infiltration or
myometrial invasion.
The actual length of the carcinomas were calculated
from the length determined microscopically, using the following
equation: L1/L2 = A1/A2 where L1 is the length of the normal
esophagus above the esophageal tumor and A1 is the distance between
ML and main tumor prior to surgery. L2 is the normal esophagus
above the esophageal tumor and A2 is the distance between ML and
main tumor following surgery. Using this equation the distance
between the ML and the main tumor in the patient prior to the
operation may be calculated. All other actual lengths were
calculated using the same method (Fig.
2).
Statistical analysis
Statistical analyses were conducted using SPSS
version 11.5 (SPSS, Inc., Chicago, IL, USA) and data are presented
as the mean ± standard deviation. The means of the two groups were
compared by t-test, and the means of multiple groups were compared
by analysis of variance and χ2 test. Correlations
between the pathological features were analyzed by the Pearson’s
correlation test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Comparison of lesion lengths
The comparison between lesion lengths determined by
esophagography, esophagoscopy and CT scan, and those measured
during surgery are shown in Table
I. The mean lesion length determined by esophagoscopy was
5.20±1.64 cm, which was significantly different (P=0.004) from the
mean lesion length observed during surgery (5.83±1.41 cm).
Esophageal stenosis, which inhibits esophagoscopy, may account for
this. The lesion lengths determined by CT scan were the largest.
This may be associated with the thickening of the esophageal lumen
due to esophageal edema around the EC.
 | Table IComparison between tumor lengths
measured during surgery and other methods. |
Table I
Comparison between tumor lengths
measured during surgery and other methods.
| Measuring method | Mean, cm | T-value | P-value |
|---|
| Surgery | 5.83±1.41 | | |
| Esophagography | 5.51±1.46 | 2.495 | 0.016 |
| Esophagoscopy | 5.20±1.64 | 3.056 | 0.004 |
| CT scan | 6.30±2.81 | 2.064 | 0.042 |
Vascular tumor emboli and lymphatic
invasion
Vascular tumor emboli were identified in six out of
52 patients, accounting for 11.5% of the total number of patients.
Statistical analysis was not performed, as only six cases were
identified. In addition, lymphatic invasion was observed in 36 out
of 52 patients, accounting for 69.2% of the total number of
patients.
Distribution and factors affecting
ML
A total of 28.8% of the patients (15 out of 52) were
found to exhibit ML, with seven cases identified at the proximal
end (upper) of the section, three cases at the distal end (lower)
and five cases at both ends. The mean proximal distance between the
ML and the main tumor, in addition to the length of the ML was
3.02±1.45 cm (largest length, 5.0 cm). In 95% of patients, a
distance of <5.0 cm was exhibited, while 90% of patients
exhibited a distance of <4.5 cm. The mean distal distance
between the ML and the main tumor, in addition to the length of the
ML was 2.60±2.44 cm (largest length, 7.5 cm). In 95% of patients, a
distance of <7.5 cm was exhibited, while 90% of patients
exhibited a distance <5.0 cm. No significant difference was
identified between the mean proximal and mean distal distances
(P=0.633; Table II).
| Table IIDistances between the subclinical
lesion and the main tumor in addition to the subclinical lesion
itself. |
Table II
Distances between the subclinical
lesion and the main tumor in addition to the subclinical lesion
itself.
| Subclinical
lesion | Maximum, cm | Mean, cma | 95% CI, cm | 90% CI, cm | T-value | P-value |
|---|
| ML |
| Proximal end | 5.0 | 3.02±1.45 | ≤5.0 | ≤4.5 | 0.486 | 0.633 |
| Distal end | 7.5 | 2.60±2.44 | ≤7.5 | ≤5.0 | | |
| SD |
| Proximal end | 5.0 | 2.45±1.30 | ≤4.5 | ≤3.8 | 1.232 | 0.229 |
| Distal end | 6.25 | 3.24±2.18 | ≤6.0 | ≤5.0 | | |
| DI |
| Proximal end | 6.4 | 2.80±1.52 | ≤5.0 | ≤4.7 | 2.012 | 0.049 |
| Distal end | 6.0 | 2.02±1.51 | ≤4.8 | ≤3.9 | | |
The lesion length and invasion depth were reduced in
the patients with ML compared with the patients without ML (P=0.039
and 0.028, respectively), however, no significant difference was
identified in the tumor volume between the two groups (Table III). Lymphatic invasion was
identified in 36 cases and of these, 14 were found to exhibit ML,
accounting for 38.9%, whereas only one patient was identified with
ML from the 16 patients without lymphatic invasion (6.3%). A
statistically significant difference was identified between the two
groups (P=0.036). However, no significant correlation was
identified between the ML, type of primary tumor, lesion position,
N stage and TNM stage (Table
IV).
| Table IIICorrelation between the subclinical
lesions and local tumor factors. |
Table III
Correlation between the subclinical
lesions and local tumor factors.
| Subclinical
lesion | Tumor length | Tumor invasion | Tumor volume |
|---|
|
|
|
|---|
| Mean, cma | T-value | P-value | Mean, cma | T-value | P-value | Mean,
cm3a | T-value | P-value |
|---|
| ML |
| Yes | 4.46±1.15 | 2.125 | 0.039 | 2.95±0.53 | 2.262 | 0.028 | 26.83±11.84 | 0.929 | 0.357 |
| No | 5.49±1.73 | | | 3.35±0.59 | | | 33.27±10.59 | | |
| SD |
| Yes | 5.64±1.10 | 0.984 | 0.331 | 3.54±1.14 | 0.807 | 0.423 | 29.02±14.24 | 0.900 | 0.373 |
| No | 6.04±1.71 | | | 3.79±1.14 | | | 32.94±17.20 | | |
| DI |
| Yes | 5.80±1.50 | 0.216 | 0.830 | 3.77±1.13 | 2.040 | 0.047 | 30.03±16.38 | 0.708 | 0.482 |
| No | 5.91±1.04 | | | 3.00±0.89 | | | 33.81±12.75 | | |
| Table IVFactors affecting the subclinical
lesions. |
Table IV
Factors affecting the subclinical
lesions.
| ML | SD | DI |
|---|
|
|
|
|
|---|
| Factors | No, n | Yes, n | χ2 | P-value | No, n | Yes, n | χ2 | P-value | No, n | Yes, n | χ2 | P-value |
|---|
| Lesion position | | | 1.21 | 0.539 | | | 0.09 | 0.947 | | | 0.62 | 0.780 |
| Upper esophagus | 5 | 1 | | | 3 | 3 | | | 1 | 4 | | |
| Middle
esophagus | 25 | 11 | | | 16 | 20 | | | 6 | 31 | | |
| Lower esophagus | 5 | 1 | | | 3 | 3 | | | 2 | 4 | | |
| Lymphatic
invasion | | | 4.15 | 0.038 | | | 0.18 | 0.675 | | | 4.12 | 0.043 |
| Yes | 20 | 12 | | | 15 | 18 | | | 5 | 30 | | |
| No | 15 | 1 | | | 7 | 8 | | | 5 | 8 | | |
| N stage | | | 3.42 | 0.057 | | | 0.43 | 0.691 | | | 1.82 | 0.183 |
| N0 | 21 | 4 | | | 11 | 19 | | | 4 | 21 | | |
| N1 | 14 | 9 | | | 11 | 7 | | | 5 | 16 | | |
| TNM stage | | | 2.09 | 0.135 | | | 0.14 | 0.718 | | | | |
| II | 21 | 5 | | | 13 | 14 | | | 7 | 19 | 3.73 | 0.050 |
| III + IV | 14 | 8 | | | 9 | 12 | | | 2 | 20 | | |
Distribution and factors affecting
SD
A total of 53.8% of patients (28 out of 52) were
found to exhibit SD, with 11 cases identified at the proximal end
of the section, 11 cases at the distal end and six cases at both
ends. The mean proximal distance between the SD and the main tumor,
in addition to the length of the SD was 2.45±1.30 cm. The mean
distal distance between the SD and the main tumor, in addition to
the length of the SD was 3.24±2.18 cm. No significant difference
was identified between the mean proximal and mean distal distances
(P=0.229; Table II). In addition,
no significant correlation was identified between the lesion
length, invasion depth and tumor volume and the SD (Table III), or between the SD and the
type of primary tumor, lymphatic invasion, lesion position, N stage
and TNM stage (Table IV).
Distribution and factors affecting
DI
A total of 78.8% of patients (41 out of 52) were
found to exhibit DI, with 12 cases identified at the proximal end
of the section, 10 cases at the distal end and 19 cases at both
ends. The mean proximal distance between the DI and the main tumor,
in addition to the length of the DI was 2.80±1.52 cm (largest
length, 6.4 cm). The mean distal distance between the DI and the
main tumor, in addition to the length of the DI was 2.02±1.51 cm
(largest length, 6.0 cm). The mean proximal distance was
significantly larger than the mean distal distance (P=0.049;
Table II). In addition, the
invasion depths were larger in patients with DI when compared with
that of patients without DI (P=0.047). No significant correlation
was identified between the lesion length, and tumor volume and the
DI (Table III). However, a
significant correlation was identified between lymphatic invasion
and TNM stage (P=0.044) and the DI (P=0.05). No significant
correlation was identified between the tumor volume and lesion
position and the N stage (Table
IV).
Discussion
Two hypotheses exist with regard to EC patients with
ML (6,7); one proposes that EC evolved from a
monoclonal cell, whereas the other hypothesizes that EC has a
polyclonal origin. The reported incidence of EC patients with ML is
0.8%–10.8% (8). In the current
study, the incidence of ML was 28.8%, which is markedly higher than
the reported incidence in the literature. This may be due to the
large sections used for pathological examination, which provide
more information with regard to the tumor. It was also revealed
that smaller tumors were found to correlate with a higher incidence
of ML. This indicated that under the effect of the same outside
carcinogenic factors, a fragment of normal esophageal tissue may
exhibit atypical hyperplasia in multiple sites. This atypical
hyperplasia may develop from mild to moderate hyperplasia, severe
hyperplasia, carcinoma in situ or invasive carcinoma. The
small foci of these different sites gradually grow and fuse into
visible tumors, which induce clinical symptoms, including
swallowing difficulty and hiccups. The incidence of ML is decreased
when these multicarcinoma in situ or microinvasive
carcinomas merge with each other. This may explain why certain
pathologists have identified >8 ML in early EC (9). In the current study, the proportion of
ML in patients with lymphatic invasion was identified to be larger
than that of patients without lymphatic invasion, indicating that
ML occurs simultaneously under the same pathogenic factors. An
additional possibility is that cancer cells have migrated along the
longitudinal lymphatics and settled at a certain point, and
proliferation started from there.
In the current study, the incidence of SD was 53.8%.
Epidemiological studies have shown that the incidence of EC
requires a continuous spectrum evolution, i.e., esophageal squamous
epithelium, mild atypical hyperplasia, moderate atypical
hyperplasia, SD, carcinoma in situ and invasive carcinoma
(10,11). Much focus has been applied to SD,
which exhibits undifferentiated atypical cells that account for
>2/3 of the esophageal epithelial cell layer, but do not break
through the underlying membrane. Carcinoma in situ refers to
cancerized epithelial layers, which do not break through the
basement membrane or infiltrate downward. Tao and Zong (12) analyzed EC specimens and found that
the p53-positive and SD rates in carcinoma in situ were 98
and 79%, respectively (P>0.05). Although the specimens of the
two groups exhibited different clinical stages, no differences in
SD or p53 protein expression in carcinoma in situ were
identified, indicating that SD has a carcinomic nature. Therefore,
the current study also observed the occurrence of SD and summarized
its characteristics. DI and lymphatic invasion have been identified
in EC, which has the biological behavior of infiltrating along the
esophageal mucosa or spreading to the upper esophagus in lesions of
≤10 cm in size (13). Compared with
solid tumors from other areas, EC exhibits a longer diffusion
distance, as the cancer cells infiltrate the esophageal wall and
spread to the surrounding tissue. Notably, cancer cells can
infiltrate along the lymphatics in the lower lamina propria, and
occasionally cause nodular mucosal surface uplift. However, in the
majority of cases, no evident abnormalities are identified and
confirmation by microscope is required. This diffusion may be
identified 5 or even >10 cm away from the primary tumor range,
according to the published data. The majority of the literature
supports the hypothesis that the diffusion distance to the upper
end is larger than that to the lower end (13), which was also confirmed in the
current study.
Although large sections for pathological study have
a long production period, the entire tumor is included, as well as
the proximal and distal resected tissues. The end results also have
more integrity and continuity, and are excellent for investigating
the associations between tumors and their surrounding tissues.
In conclusion, esophageal squamous cell carcinoma
exhibits the characteristics of ML, SD and DI, and the occurrence
of ML and SD has been associated with lymphatic invasion. In 95% of
the subclinical lesions observed in the current study, the proximal
distance was 5.0 cm and the distal distance was 7.5 cm, while in
90% of the subclinical lesions, the proximal distance was 4.7 cm
and the distal distance was 5.0 cm. Further information may be
obtained by future investigations of the pathological
characteristics of EC, which could be used to identify a potential
breakthrough in cancer research to relieve the suffering of
patients, while reducing normal tissue damage and maximally
improving quality of life.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011.
|
|
2
|
Boonstra JJ, Kok TC, Wijnhoven BP, et al:
Chemotherapy followed by surgery versus surgery alone in patients
with resectable oesophageal squamous cell carcinoma: long-term
results of a randomized controlled trial. BMC Cancer.
11:1812011.
|
|
3
|
Yamashita H, Okuma K, Wakui R,
Kobayashi-Shibata S, Ohtomo K and Nakagawa K: Details of recurrence
sites after elective nodal irradiation (ENI) using 3D-conformal
radiotherapy (3D-CRT) combined with chemotherapy for thoracic
esophageal squamous cell carcinoma - a retrospective analysis.
Radiother Oncol. 98:255–260. 2011.
|
|
4
|
Ono S, Fujishiro M, Niimi K, et al:
Long-term outcomes of endoscopic submucosal dissection for
superficial esophageal squamous cell neoplasms. Gastrointest
Endosc. 70:860–866. 2009.
|
|
5
|
Sobin LH and Wittekind CH; International
Union Against Cancer (UICC). TNM Classification of Malignant
Tumors. 5th edition. Wiley; New York: 1997
|
|
6
|
Wang LD, Zhou Q, Hong JY, et al: p53
protein accumulation and gene mutation in multifocal esophageal
precancerous lesions from symptom free subjects in a high incidence
area for esophageal carcinoma in Henan, China. Cancer.
77:1244–1249. 1996.
|
|
7
|
Strong MS, Incze J and Vaughan CW: Field
cancerization in the aerodigestive tract - its etiology,
manifestation, and significance. J Otolaryngol. 13:1–6. 1984.
|
|
8
|
Zhou H: Multiple esophageal primary
cancer. Chinese J Clin Oncol. 13:2181986.
|
|
9
|
Liu FW, Qin DX and Wang QL: 172 cases of
multiple cancer clinical pathology analysis. Chinese J Cancer.
2:1131979.
|
|
10
|
Wang LD, Qiu SL, Yang GR, Lipkin M,
Newmark HL and Yang CS: A randomized double-blind intervention
study on the effect of calcium supplementation on esophageal
precancerous lesions in a high-risk population in China. Cancer
Epidemiol Biomarkers Prev. 2:71–78. 1993.
|
|
11
|
Tao YS and Zong S: Expression and meaning
of p53 protein in epithelial cells and carcinoma in situ.
Clinical Oncology. 7:168–169. 2002.
|
|
12
|
Zhang TL, Zhou HP, Yan SB, et al: Explore
the length of esophageal resection. Chinese J Clin Oncol.
22:141995.
|
|
13
|
Zhang TL and Zhou HP: One case of repeat
cancer by five surgery reported of long-term survival. Cancer
Prevention and Treatment Research. 21:3021994.
|