Introduction
Langerhans cell histiocytosis (LCH), formerly termed
histiocytosis X, is a disease characterized by the neoplastic
proliferation of Langerhans cells (1). LCH is rare in the adult population,
and additional multifocal involvement is even rarer (2–5). LCH
includes three subtypes: Eosinophilic granuloma (EG),
Hand-Schuller-Christian disease and Letterer-Siwe disease. EG is
the major type, accounting for 60–70% of all LCH cases; it is a
localized form and presents as unifocal or multifocal bone lesions
(6,7).
Adult LCH may involve the temporal bone and jaws
(8,9). In extremely rare cases, the jaws
involved may be fractured due to continuous enlargement of the
osteolytic lesion. The present study reports a case of LCH in an
adult male in which multiple bones (mandible, rib and pelvis) were
involved. In this case, the mandible was pathologically fractured
and spontaneously healed eight months later. To the best of our
knowledge, no similar case has ever been reported. Therefore, the
clinical, radiographical and histopathological features of this
rare case are highlighted. Patient provided written informed
consent.
Case report
A 39-year-old male presented with a one-year history
of pain, swelling of the gingiva and an occasional pus-like
discharge in the right mandible. Several teeth had slowly become
loose and one tooth had fallen out. The patient was previously
prescribed antibiotics by a local dentist who considered the
problem to be a bacterial infection. The symptoms were alleviated,
yet the problem was never completely resolved. Eight months prior
to the current presentation, an initial panoramic radiography of
the jaw was taken in a local hospital and the patient was diagnosed
with osteomyelitis of the jaw. Although it was suggested that the
patient should receive further treatment at a tertiary hospital,
since the symptoms were tolerable, this advice was not followed in
the eight months previous to the current presentation. At this
time, the patient was immediately admitted to the Department of
Oral and Maxillofacial Surgery, Second Affiliated Hospital,
Zhejiang University School of Medicine (Hangzhou, China) for
further investigation.
Clinical palpation of the right mandible revealed
that the lateral surface of the mandibular body bulged and that the
inferior margin of the body was concave. The first molar was
missing and mobility of the neighboring teeth was detected. The
second and third molars sloped anteriorly, resulting in immature
tooth contact. There was a conspicuous pit in the right mandible,
between the first premolar and the second molar, yet no obvious
pus-like discharge was found (Fig.
1). The midline of the mandible was shifted to the right by ~2
mm.
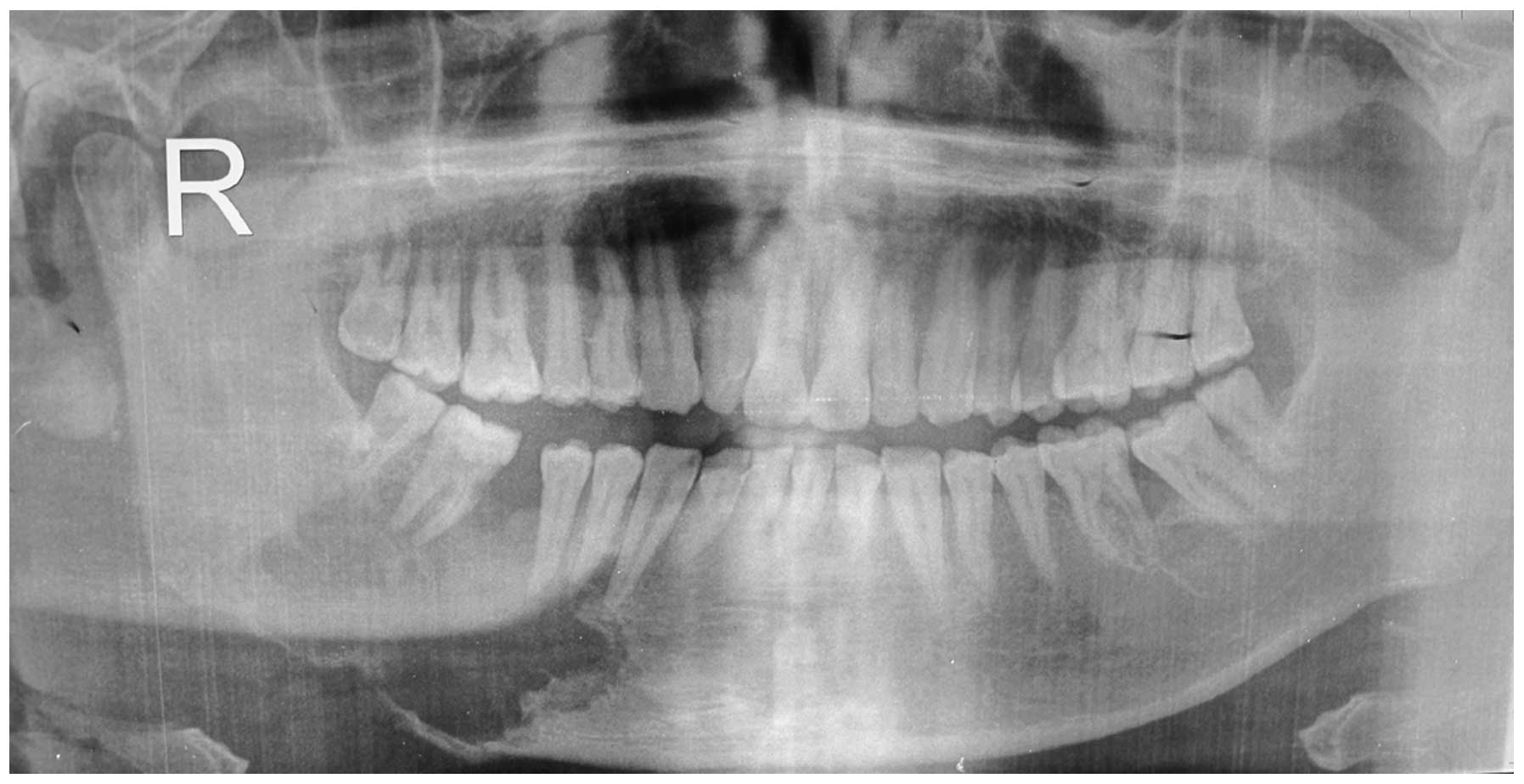
The initial panoramic radiograph showed an
osteolytic lesion in the right mandible, ranging from the canine to
the third molar, and with a moth-eaten margin. The lesion had
already invaded the cortices and resulted in a pathological
fracture of the mandible (Fig. 2).
As the supporting bone was destroyed, the involved teeth appeared
to be floating in the osteolytic lesion. The displacement of bone
fragments led to immature contact of the lower third molar with the
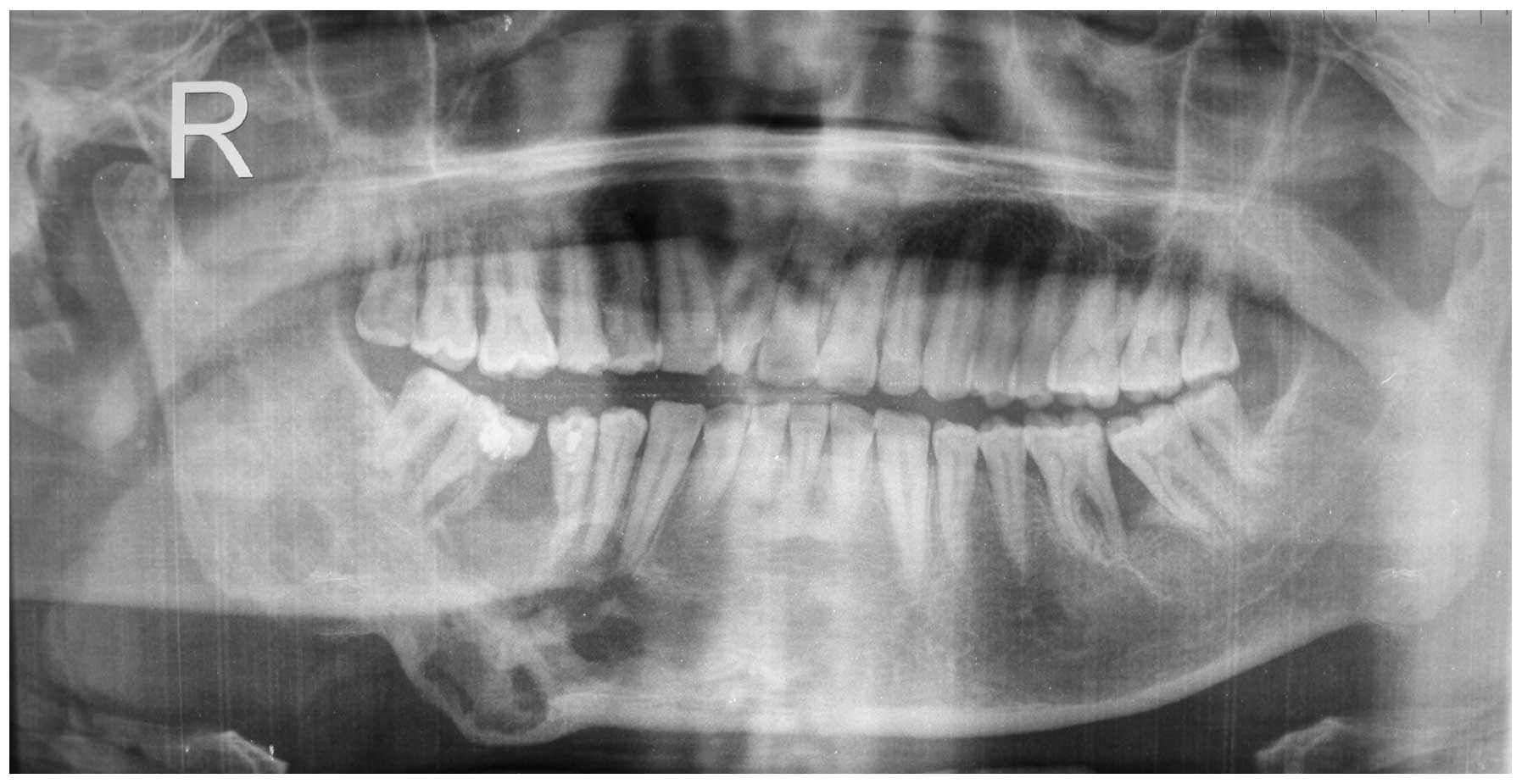
upper second molar (Fig. 2). A
second panoramic radiograph taken at the Second Affiliated
Hospital, Zhejiang University School of Medicine (Hangzhou, China)
showed that eight months later, although the lesion had continued
to expand slightly, there was apparent new bone regeneration in the
previous osteolytic area, which had resulted in a malunion of the
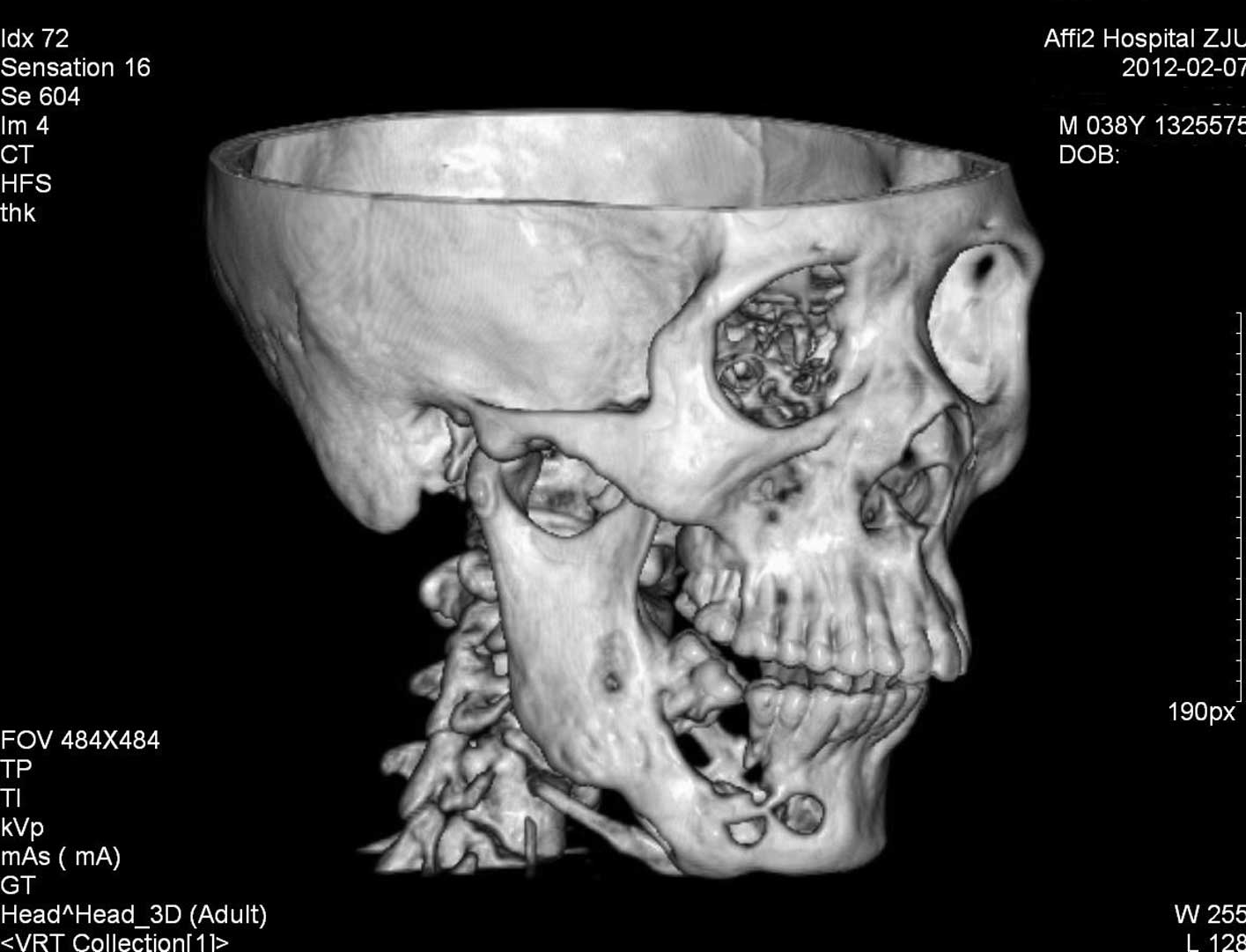
fractured bone segments (Fig. 3).
The continuity of the right mandible was also confirmed by computed
tomography (CT) scanning (Fig.
4).
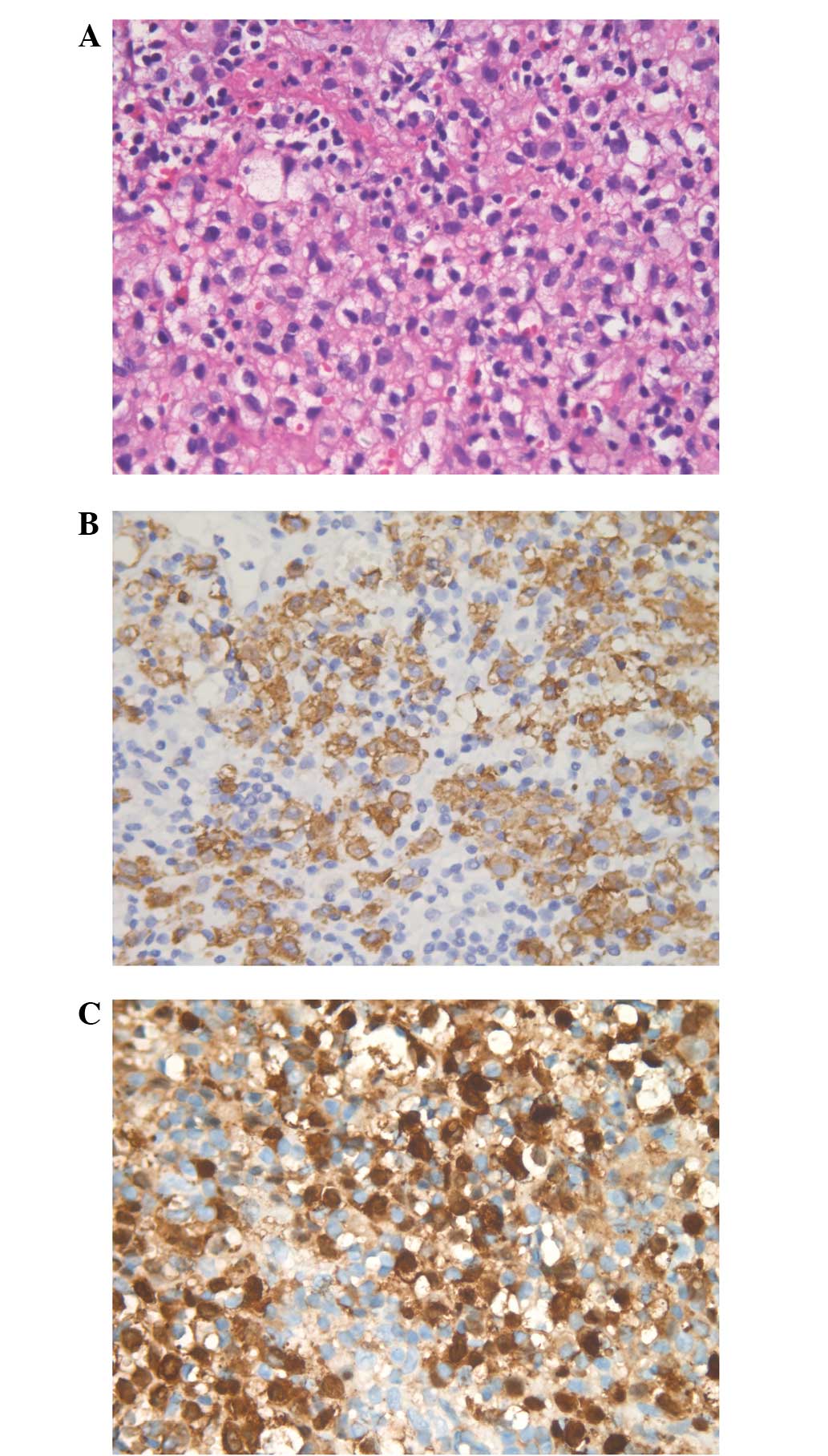
To establish a diagnosis, an incisional biopsy was
performed. This showed clusters of medium-sized cells with coffee
bean-like nuclei that were folded or grooved; the characteristic
feature of Langerhans cells. A few eosinophils were also found
around these characteristic cells (Fig.
5A). These clusters of cells were finally identified as
Langerhans cells by their intense immunoreactivity for S-100
protein and cluster of differentiation (CD)1a (Fig. 5B and C). The diagnosis of LCH was
consequently confirmed.
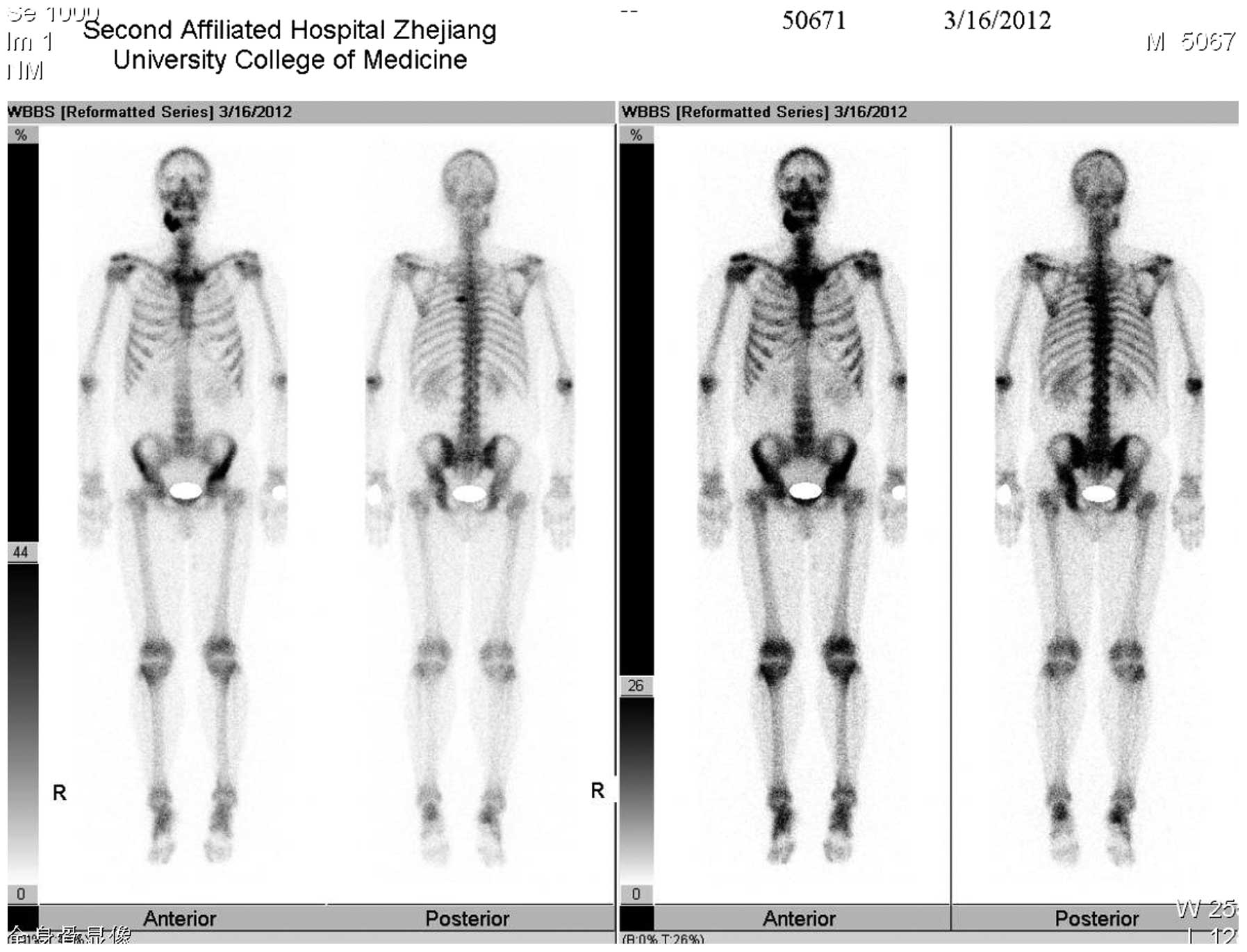
Nuclear bone scanning with technetium-99m was then
performed to investigate whether other bones were involved; besides
the right mandible, the left ilium and the left fifth rib also
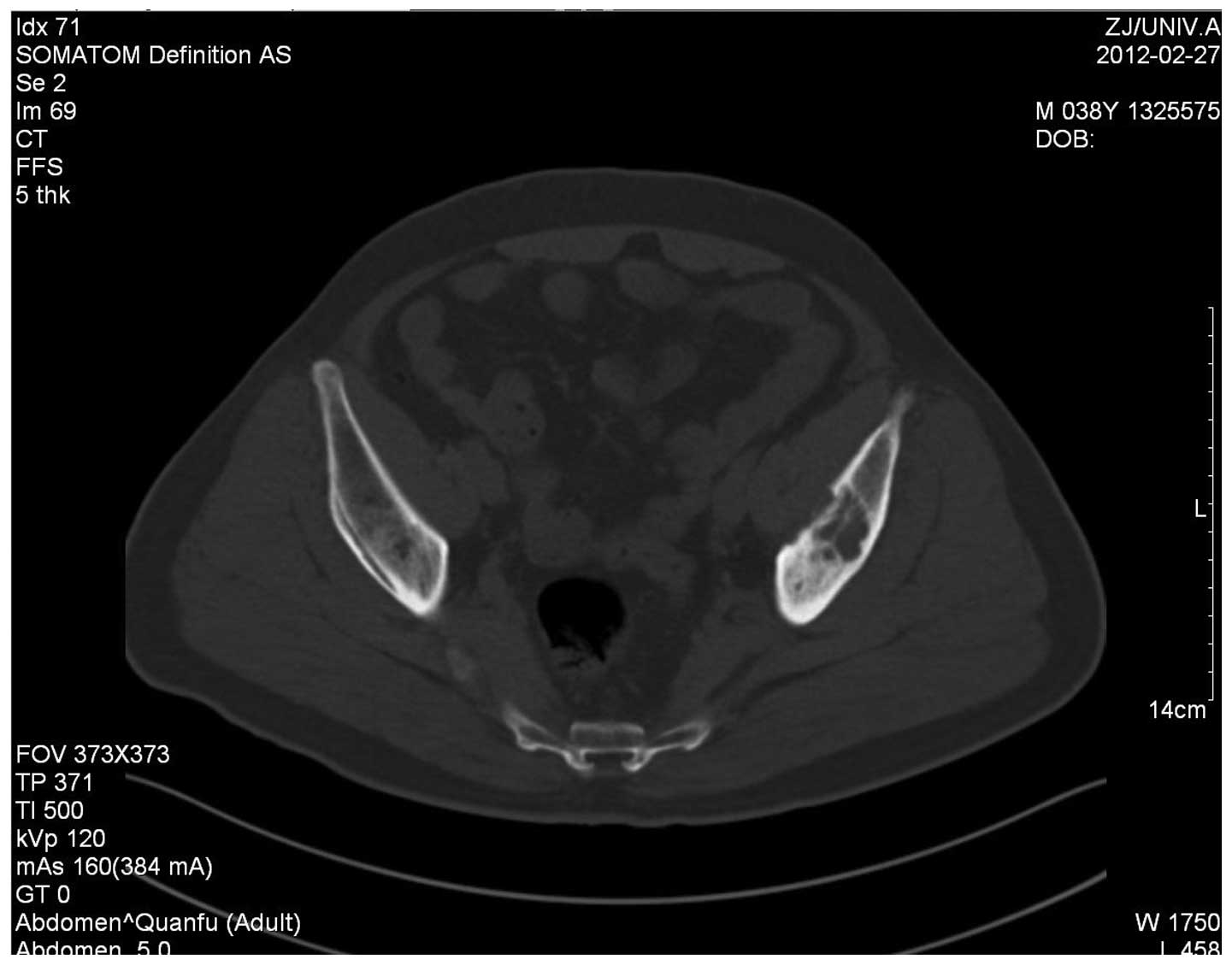
showed increased uptake of the radionuclide (Fig. 6). CT scanning also confirmed the
osteolytic focus in the left ilium (Fig. 7). No more organs were found to be
involved by either chest radiography or magnetic resonance (MR)
scanning of the abdomen. The patient was finally diagnosed with LCH
with multifocal bone lesions.
As multiple bones were involved, surgical oblation
or curettage was not the first treatment option. The patient was
referred to the hematological department and received combination
chemotherapy. The chemotherapy lasted for nine months and was
divided into six courses. In each course the patient was
administeres 750 mg etoposide, 160 mg vincaleukoblastine and 1.47 g
prednisone.
Discussion
In the present rare case, multiple bones were
involved in LCH in an adult patient. It was noteworthy that the
mandible involved was fractured due to the enlargement of the
osteolytic lesion, and was re-united simultaneously, without any
special medical interference, eight months later. This case
presents valuable clinical evidence that intralesional bone
regeneration may occur under natural conditions in an adult with
LCH.
LCH is a rare disease, with an incidence of five
cases per million individuals and one to two cases per million
adults (1–5). Various organs may be involved,
including the liver, skin, lungs, lymph nodes, bone marrow and
spleen. However, the bone is the organ most frequently involved.
The jaws are reported to be affected in 10–20% of all LCH cases
(10,11) and the mandible is three times more
frequently involved than the maxilla. The posterior mandibular
region is the most frequently affected region (10).
The common clinical manifestations of LCH in the
maxillofacial region include intraoral masses or swelling, pain,
gingivitis, ulcers of the mucosa and loss of/loose teeth due to the
erosion of the supporting bone tissue (10,12).
Radiographically, these osteolytic jaw lesions tend to have a
well-defined radiolucent appearance. Erosion of the bone around the
teeth often gives the appearance that the teeth are floating on the
radiolucent lesion (7,10,12).
Root resorption of the involved teeth may occur, but is not common.
A radiographical differentiation diagnosis is necessary between LCH
and other osteolytic diseases, including osteomyelitis,
osteosarcoma, odontogenic cysts and giant cell granuloma.
In the present case, a biopsy showed there were
clusters of cells with a reniform nucleus that was deeply indented
or grooved like a coffee bean. This is the typical feature of
Langerhans cells, the hallmark cells of LCH. Immunohistochemesitry
showed that these cells were positively stained for S-100 protein
and CD1a antibodies. Generally, a biopsy is mandatory to
differentiate LCH from other osteolytic malignant tumors. A
presumptive diagnosis is made when the typical morphological
features of Langerhans cells are found, and confirmed if stains for
S-100 protein and CD1a antigen are both positive. In addition, the
finding of Birbeck granules under electric microscope also confirms
the diagnosis (5). Once a diagnosis
of LCH has been established, it is necessary to perform further
examinations, such as nuclear bone scanning, CT and MR imaging, to
decide if occult lesions exist in other skeletal sites or other
organs. This is an important aspect of the planning of a definitive
treatment.
Treatment modalities for adult LCH include surgical
curettage or resection, irradiation, local drug injection and
systemic chemotherapy. These methods may be used either alone or in
combination. With regard to a focal bone lesion, surgical curettage
or bone resection remain choices for treatment (13,14).
Local radiation may aid in the relief of symptoms, but seldom
achieves complete remission when used alone (7). Intralesional drug injections may be an
effective option for a localized LCH. Libicher et al
reported cases of complete remission of a solitary bone lesion
within 6 months following a single local application of
methylprednisolone (15). Other
studies reported satisfactory results with intralesional steroid
injections or indomethacin (16–19).
With regard to a soft tissue lesion or multifocal bone lesions
however, systemic chemotherapy is often the first choice (20). A previous study has even recommended
multiagent chemotherapy for bone-only LCH, whether unifocal or
multifocal, based on clinical data that single agent chemotherapy
or irradiation is associated with a higher recurrence rate
(10). The prognosis of LCH is
related to the age of patients at the time of onset. Generally, the
prognosis is poorer in young patients and improved in elderly
patients. The prognosis is also associated with the number of
organs involved, being poorer when multiple organs are affected
(21).
The current study presented a case of LCH with
multiple bone lesions in an adult. Considering the chief
complaints, it could easily have been misdiagnosed as an
inflammatory disease. The radiographical appearance of an
osteolytic lesion with a moth-eaten margin in the mandible was
similar to that of an osteosarcoma. This case highlighted the fact
that LCH should be one of the differential diagnoses for an
osteolytic lesion of the jaw in an adult. The panoramic radiograph
showed that the mandible was fractured and displaced due to
enlargement of the lesion. However, a second radiograph showed that
the fracture had been mal-united eight months later and that a
quantity of new bone had formed in the previous radiolucent cavity.
This indicated that the patient had a relatively good prognosis.
However, since there were other lesions in the rib and ilium,
multiagent chemotherapy was necessary. The effectiveness of the
treatment was proven by the findings of recent CT scans. However,
resection of the mandibular lesion and immediate reconstruction
with autogenous bone grafting can be reserved for later use, in
case chemotherapy fails to result in complete healing. Also, an
osteotomy of the mandible may be performed later to correct the
malocclusion.
In summary, the present study documented the
clinical and radiographical manifestations of an unusual case of
LCH in an adult. In this case, multiple bones were involved and a
pathological mandibular fracture occurred. For the first time, this
case provides evidence that spontaneous intralesional bone
regeneration exists and may subsequently lead to reunification of
the fractured mandible in an adult patient with LCH.
Acknowledgements
This study was supported by the Qianjiang
Intelligent Project Fund of Zhejiang Province (no. 2010R10070) and
the Department of Education of Zhejiang Province (no
Y201018977)
References
|
1
|
Nicholson HS, Egeler RM and Nesbit ME: The
epidemiology of Langerhans cell histiocytosis. Hematol Oncol Clin
North Am. 12:379–384. 1998.
|
|
2
|
Favara BE, Feller AC, Pauli M, et al:
Contemporary classification of histiocytic disorders. The WHO
Committee On Histiocytic/Reticulum Cell Proliferations
Reclassification Working Group of the Histiocyte Society. Med
Pediatr Oncol. 29:157–166. 1997.
|
|
3
|
Aricò M, Girschikofsky M, Généreau T, et
al: Langerhans cell histiocytosis in adults. Report from the
International Registry of the Histiocyte Society. Eur J Cancer.
39:2341–2348. 2003.
|
|
4
|
Coppes-Zantinga A and Egeler RM: The
Langerhans cell histiocytosis X files revealed. Br J Haematol.
116:3–9. 2002.
|
|
5
|
Leonidas JC, Guelfguat M and Valderrama E:
Langerhans’ cell histiocytosis. Lancet. 361:1293–1295. 2003.
|
|
6
|
Piattelli A and Paolantonio M:
Eosinophilic granuloma of the mandible involving the periodontal
tissues. A case report. J Periodontol. 66:731–736. 1995.
|
|
7
|
dos Anjos Pontual ML, da Silveira MM, de
Assis Silva Lima F and Filho FW: Eosinophilic granuloma in the
jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 104:e47–51.
2007.
|
|
8
|
Alexander RL, Worthen ML, Pang CS and May
JS: Langerhans cell histiocytosis: temporal bone invasion in an
adult. Ear Nose Throat J. 92:4964982013.
|
|
9
|
Yepes JF, Khalaf M, Cunningham L, et al:
Chronic focal Langerhans cell histiocytosis of the left mandibular
condyle presenting as limited jaw opening: a case report. Ear Nose
Throat J. 91:E26–E30. 2012.
|
|
10
|
Hicks J and Flaitz CM: Langerhans cell
histiocytosis: current insights in a molecular age with emphasis on
clinical oral and maxillofacial pathology practice. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 100(2 Suppl): S42–S66. 2005.
|
|
11
|
Neville BW, Damm DD, Allen CM, et al:
Hematologic disorders. Oral and Maxillofacial Pathology. 2nd
edition. WB Saunders; Philadelphia: pp. 513–515. 2002
|
|
12
|
Eckardt A and Schultze A: Maxillofacial
manifestations of Langerhans cell histiocytosis: a clinical and
therapeutic analysis of 10 patients. Oral Oncol. 39:687–694.
2003.
|
|
13
|
Alexiou GA, Mpairamidis E, Sfakianos G and
Prodromou N: Cranial unifocal Langerhans cell histiocytosis in
children. J Pediatr Surg. 44:571–574. 2009.
|
|
14
|
Bartnick A, Friedrich RE, Roeser K and
Schmelzle R: Oral Langerhans cell histiocytosis. J Craniomaxillofac
Surg. 30:91–96. 2002.
|
|
15
|
Libicher M, Roeren T and Tröger J:
Localized Langerhans cell histiocytosis of bone: treatment and
follow-up in children. Pediatr Radiol. 25(Suppl 1): S134–S137.
1995.
|
|
16
|
Esen A, Dolanmaz D, Kalayci A, et al:
Treatment of localized Langerhans’ cell histiocytosis of the
mandible with intralesional steroid injection: report of a case.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 109:e53–e58.
2010.
|
|
17
|
Moralis A, Kunkel M, Kleinsasser N, et al:
Intralesional corticosteroid therapy for mandibular Langerhans cell
histiocytosis preserving the intralesional tooth germ. Oral
Maxillofac Surg. 12:105–111. 2008.
|
|
18
|
Park JW and Chung JW: Long-term treatment
of Langerhans cell histiocytosis of the mandibular condyle with
indomethacin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
109:e13–e21. 2010.
|
|
19
|
Putters TF, de Visscher JG, van Veen A and
Spijkervet FK: Intralesional infiltration of corticosteroids in the
treatment of localised langerhans’ cell histiocytosis of the
mandible: Report of known cases and three new cases. Int J Oral
Maxillofac Surg. 34:571–575. 2005.
|
|
20
|
Liu YH, Fan XH and Fang K: Langerhans’
cell histiocytosis with multisystem involvement in an adult. Clin
Exp Dermatol. 32:765–768. 2007.
|
|
21
|
Muramatsu T, Hall GL, Hashimoto S, et al:
Clinico-pathologic conference: case 4. Langerhans cell
histiocytosis (LCH). Head Neck Pathol. 4:343–346. 2010.
|