Introduction
In 1939, Buchbinder and Lipkopf initially used the
term ‘splenosis’ to describe the heterotopic autotransplantation of
splenic tissues (1); following
this, reports of such conditions are gradually increasing.
Currently, splenosis is not considered to be a rare disease, and
the incidence of splenosis in patients with spleen trauma or
splenectomy may be ≤67% (2).
However, splenosis is often diagnosed incidentally. Splenosis is
commonly observed in the abdomen and pelvic cavity; it mimics
malignancy on abdominal imaging, regardless of the signs and
symptoms, and may also lead to unnecessary surgical interventions
(3). The current study reports a
case of duodenal splenosis located outside of the descending
section of the duodenum. The patient underwent unnecessary
laparotomy due to a significant diagnostic dilemma, as the
possibility of a malignant tumor could not be eliminated. Written
informed consent was obtained from the patient.
Case report
A 55-year-old female was admitted to the Department
of Biliary Surgery, West China Hospital (Chengdu, China) with a
history of duodenal mass, which was identified following a routine
physical examination in a local hospital. No systemic symptoms were
observed and there was no history of malignancy or weight loss. The
patient had a history of splenectomy following a traumatic spleen
rupture due to a traffic accident 27 years previously. No history
of drug and alcohol abuse was evident, the patient had a normal
dietary history and had not previously visited the nomadic areas,
where echinococcosis is prevalant. Physical examination and the
initial laboratory tests at the West China Hospital revealed no
abnormalities with the exception of the presence of a postoperative
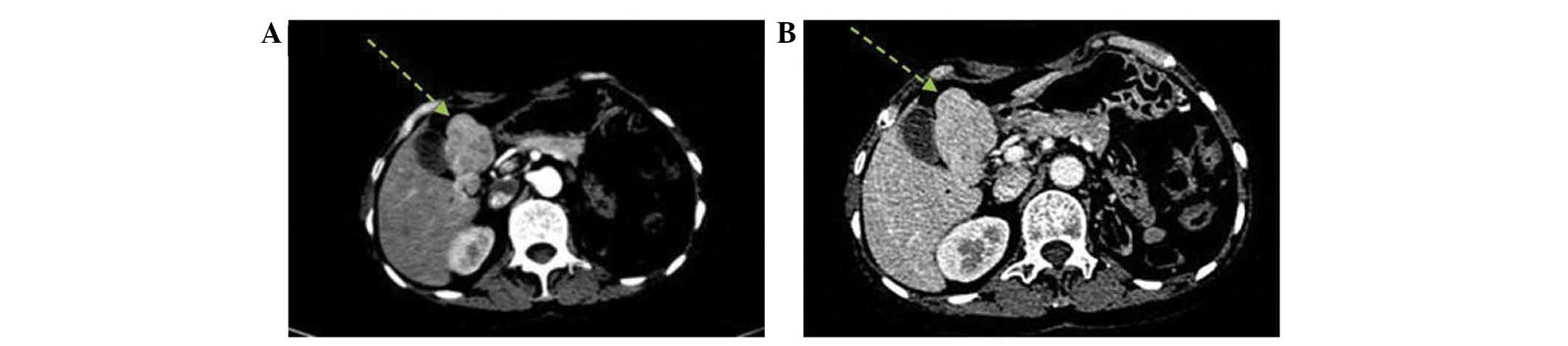
abdominal scar in the left upper quadrant. Abdominal ultrasound
revealed no visual spleen due to the splenectomy, and a hilar mass
measuring 3.9×2.6×4.9 cm with a rich blood supply. Subsequent
contrast helical computed tomography (CT) imaging showed no spleen
and a mass with a maximum diameter of 6.1×3.6 cm, mass arising from
the duodenal bulb (Fig. 1), which
was considered to be a malignant duodenal stromal tumor.
Following preoperative preparation and counselling
with the patient and relatives, exploratory laparotomy was
conducted. During surgery, a multi-nodular soft tissue mass with a
dark red appearance, of 6.5×4.8×2.6 cm in size was observed around
the duodenal bulb, hilar and the gastric antrum, with a blood
supply from the duodenal wall (Fig.
2). The mass was predicted to be spleen tissue, confirmed by
intraoperative tissue biopsy, however, the mass was resected to
avoid any future problems that may arise. Following this, the
patient was diagnosed with post-splenectomy duodenal splenosis, and
was discharged on postoperative day 8 without any complications.
During hospitalization, the platelet count increased from a
preoperative level of 165×109/l (reference range,
100×109/l–300×109/l) to 314×109/l
on the day of discharge. During the six month follow-up, the
patient was asymptomatic and monthly ultrasonography revealed no
abdominal abnormalities, however, the platelet count continued to
rise to a maximum of 425×109/l in the first month
following surgery, and thereafter, a progressive decline was
observed and subsequently, platelet levels remained within the
normal range.
Discussion
The majority of cases of splenosis are the result of
post-traumatic splenectomy (4).
Following splenic rupture, damaged splenic pulp seeds in the
adjacent cavities, and grows using the blood supply from adjacent
blood vessels (5). Duodenal
splenosis is rare, and splenosis was not predicted in this patient
prior to surgery. A preliminary diagnosis of splenosis may be
determined with caution. A detailed medical history, including any
instance of post-traumatic splenectomy, and thorough physical
examination is essential, however further tests are required to
confirm the diagnosis. X-ray, ultrasound, CT and standard magnetic
resonance imaging are of limited value in the diagnosis of
abdominal splenosis (3,6). These imaging findings are nonspecific
in this entity, indicating the size, shape, number and location of
the masses, but cannot distinguish splenosis nodules from numerous
conditions such as metastatic disease; this occurred in the present
case. Technetium-99 m heat-damaged erythrocytes (RBC) or Indium
111-labeled platelets scintigraphy, have been accepted by an
increasing number of clinicians as a noninvasive nuclear
scintigraphy for the diagnosis of splenosis, due to the ability of
spleen tissue to absorb radio-labeled, damaged red blood cells
(7,8). Notably, RBC scintigraphy has been
demonstrated to exhibit increased sensitivity in early splenosis,
functional hyposplenism and poor splenic uptake (9,10).
However, despite these advanced imaging techniques, a pathological
diagnosis of splenosis is usually required, predominantly due to
the possibility of malignancy or to preoperative diagnostic
uncertainty. Therefore, in the present case, a laparoscopic
approach was adopted, providing a minimally invasive method to
directly visualize the suspected mass, allowing the biopsy and
resection, if required (11).
This was the first case of splenosis in the
Department of Biliary Surgery, West China Hospital. Due to
insufficient information with regard to this condition and
increased suspicion with regard to the progressive growth of the
mass, leading to duodenal compression, resection appeared to be
urgent. Splenosis is a benign condition and usually asymptomatic,
therefore, the removal of an asymptomatic splenosis mass is not
required. Additionally, it has been reported that splenic implants
may exert a protective immune response against bacterial infections
in asplenic patients, however, this effect is limited (12). In the present case, the gradual rise
in platelet count during the month following surgery was similar to
the change in platelet levels observed in other splenectomized
patients, where platelet levels increased before returning to
normal levels, suggesting a functional reticuloendothelial system
within the splenosis (13).
Splenosis is not a rare disease. In patients with a
history of splenic trauma or splenectomy and an abdominal mass as
the predominant clinical manifestation, particularly in the absence
of systemic symptoms, abdominal splenosis must be included in the
differential diagnosis. Once considered, combined with a
comprehensive history, noninvasive nuclear scintigraphy may serve
as a suitable diagnostic approach for splenosis, thereby avoiding
unnecessary laparotomy. In cases where a pathological diagnosis of
splenosis is required due to concern of malignancy or preoperative
diagnostic uncertainty, a laparoscopy as a minimally invasive
technique, may be utilized. Following confirmation, the removal of
splenosis nodules is not required in asymptomatic cases, as
splenosis is harmless and may exert beneficial effects in asplenic
patients.
References
|
1
|
Buchbinder JH and Lipkoff CJ: Splenosis:
multiple peritoneal splenic implants following abdominal injury.
Surgery. 6:927–934. 1939.
|
|
2
|
Kiroff GK, Mangos A, Cohen R, Chatterton
BE and Jamieson GG: Splenic regeneration following splenectomy for
traumatic rupture. Aust N Z J Surg. 53:431–434. 1983.
|
|
3
|
Fremont RD and Rice TW: Splenosis: a
review. South Med J. 100:589–593. 2007.
|
|
4
|
Brewster DC: Splenosis: report of two
cases and review of the literature. Am J Surg. 126:14–19. 1973.
|
|
5
|
Cotlar AM and Cerise EJ: Splenosis: the
autotransplantation of splenic tissue following injury to the
spleen. Report of two cases and review of the literature. Ann of
Surg. 149:402–404. 1959.
|
|
6
|
Ksiadzyna D and Peña AS: Abdominal
splenosis. Rev Esp Enferm Dig. 103:421–426. 2011.
|
|
7
|
Storm BL, Abbitt PL, Allen DA and Ros PR:
Splenosis: superparamagnetic iron oxide-enhanced MR imaging. AJR Am
J Roentgenol. 159:333–335. 1992.
|
|
8
|
Schiff RG, Leonidas J, Shende A and
Lanzkowski P: The noninvasive diagnosis of intrathoracic splenosis
using technetium-99m heat-damaged red blood cells. Clin Nucl Med.
12:785–787. 1987.
|
|
9
|
Atkins HL, Goldman AG, Fairchild RG, et
al: Splenic sequestration of Tc-99m labeled, heat treated red blood
cells. Radiology. 136:501–503. 1980.
|
|
10
|
Gunes I, Yilmazlar T, Sarikaya I, Akbunar
T and Irgil C: Scintigraphic detection of splenosis: Superiority of
tomographic selective spleen scintigraphy. Clin Radiol. 49:115–117.
1994.
|
|
11
|
Barbaros U, Dinccag A and Kabul E:
Minimally invasive surgery in the treatment of splenosis. Surg
Laparosc Endosc Percutan Tech. 16:187–189. 2006.
|
|
12
|
Pearson HA, Johnston D, Smith KA and
Touloukian RJ: The born-again spleen. Return of splenic function
after splenectomy for trauma. N Engl J Med. 298:1389–1392.
1978.
|
|
13
|
Corazza GR, Zoli G, Massai G, Mulè P,
Beltrandi E and Gasbarrini G: Changes in peripheral blood
lymphocytes and immune complexes in splenectomized patients: lack
of correlation with residual splenic function. J Clin Lab Immunol.
31:33–38. 1990.
|