Introduction
Linzhou is a city in the province of Henan in China,
that has the highest oesophageal cancer morbidity and mortality
rate in the world (1–3). Oesophageal cancer patients in Linzhou
have an evident familial aggregation phenomenon. The family members
of oesophageal cancer patients are associated with a markedly
higher risk of prevalence (4). A
descendant of a family with a positive history of oesophageal
cancer (OCFH +) tends to have a higher tumour susceptibility when
compared with a descendant of a family that has a negative history
of oesophageal cancer (OCFH −); the susceptibility increases with
the positive family history (5–7). This
observation indicates that genetic factors may be significant in
the occurrence of oesophageal cancer; however, the molecular basis
for susceptibility to this disease remains unclear. A previous
study has shown that chromosomal instability and dysfunction in the
DNA damage repair mechanism may be involved (8). Fragile histidine triad (FHIT)
is a recently identified candidate tumour suppressor gene, which is
located on the most active site of the human genome (position
3P14.2) and studies demonstrated that the expression of FHIT
is reduced or absent in various malignant tumours (9,10).
MutL homolog 1 (MLH1) and breast cancer type 2
susceptibility protein (BRCA2) are key genes involved in DNA
damage repair, particularly when the damage is induced by foreign
carcinogenic factors (11,12). Furthermore, these genes are closely
associated with chromosomal stability. Variation in the tumour
protein 53 (p53)-retinoblastoma protein system is a common
molecular event (13) that is
observed in oesophageal cancer patients from Henan, where there is
a high incidence of oesophageal cancer. In the present study, the
expression of the fragile site genes, FHIT and p53,
which are associated with chromosomal stability, were analysed in
excised oesophageal cancer tissue specimens, as well as the DNA
damage repair genes, BRCA2 and MLH1. The association
between these genes and the family history of cancer was also
determined. The results of the present study may contribute to
understanding the molecular mechanism of, and genetic
susceptibility of humans to, oesophageal cancer in areas with a
high incidence of this type of cancer.
Patients and methods
Patients and samples
Of the subjects enrolled in the present study, 33
were OCFH + and 41 were OCFH −; all of the subjects were residents
of Linzhou (Henan, China). OCFH + patients had a minimum of two
family members who suffered from the disease and were descendants
of families who lived in a region with a high incidence of
oesophageal cancer, in which two generations had suffered from the
disease (8). OCFH − patients were
those who had no family members who had suffered from the disease
or from other types of cancer. Of the OCFH + patients, 24 (73%)
were male and nine (27%) were female. The patients were aged
between 46 and 72 years, with an mean age of 56±9 years. Of the
OCFH − patients, 26 (63%) were male and 15 (37%) were female. The
patients were aged between 35 and 71 years, with an average age of
56±9 years. None of the patients had received chemotherapy or
radiotherapy prior to radical resection. Following surgery, the
cancer specimen was immediately fixed with 85% alcohol, dehydrated
via routine histology, embedded in paraffin and sliced into 5-μm
serial sections. Subsequently, the specimens were classified as
well-, moderately or poorly differentiated squamous cell
carcinomas, according to the cellular morphology, tissue structure
and differentiation. The diagnostic criteria were based on a
previous study (13,14) and the clinical pathological
conditions of the patients are presented in Table I. Normal adjacent tissue was also
obtained, which was ≥5 cm from the carcinoma tissue, as a control.
These healthy specimens were confirmed to have no precancerous
lesions by pathological examination. Written informed consent was
obtained from all patients and the study was approved by the ethics
committee of the First Affiliated Hospital of Zhengzhou University
(Zhengzhou, China).
 | Table IClinical pathology of oesophageal
cancer patients with a positive or negative family history of
oesophageal carcinoma in Linzhou, China. |
Table I
Clinical pathology of oesophageal
cancer patients with a positive or negative family history of
oesophageal carcinoma in Linzhou, China.
| | OCFH + | OCFH − |
|---|
| |
|
|---|
| Clinical
pathology | Cases, n | n (%) | n (%) |
|---|
| Age, years |
| ≤40 | 2 | 2 (6) | 0 (0) |
| 41–50 | 20 | 10 (30) | 10 (24) |
| 51–60 | 32 | 15 (46) | 17 (42) |
| >60 | 20 | 6 (18) | 14 (34) |
| Gender |
| Male | 50 | 24 (73) | 26 (63) |
| Female | 24 | 9 (27) | 15 (37) |
| Infiltration |
| Mucosa | 7 | 4 (12) | 3 (7) |
| Submucosa | 11 | 6 (18) | 5 (12) |
| Muscularis | 20 | 10 (30) | 10 (25) |
| Fibrous
membrane | 36 | 13 (40) | 23 (56) |
|
Differentiation |
| Well− | 10 | 7 (21) | 3 (7) |
| Moderately | 48 | 19 (58) | 29 (71) |
| Poorly | 16 | 7 (21) | 9 (22) |
| Metastasis |
| Yes | 22 | 6 (18) | 16 (39) |
| No | 52 | 27 (82) | 25 (61) |
| Total | 74 | 33 | 41 |
Immunohistochemical detection
The specimen was analysed using the avidin-biotin
horseradish peroxidase complex (ABC) method as follows: The sample
was embedded in paraffin, sliced, dehydrated in graded alcohol and
washed three times with phosphate-buffered saline (PBS) for 5 min.
BRCA2 and FHIT antigens were retrieved via microwave irradiation
for 10 min. MLH1 was placed in boiling water for 30 min and then
cooled to room temperature. Subsequently, 0.5%
H2O2 was added to MLH1 at room temperature
for 20 min and the resulting mixture was washed three times with
PBS for 5 min. BRCA2 rabbit anti-human polyclonal antibody was
purchased from Boster Biological Engineering Co., Ltd., (Wuhan,
China; dilution 1:100), MLH1 rat anti-horse monoclonal antibody was
purchased from BD Pharmingen (San Diego, CA, USA; dilution, 1:50),
the FHIT polyclonal rabbit anti-goat antibody was purchased from
Beijing Zhongshan Biotechnology Co., Ltd. (Beijing, China)
(ZA-0410; 1:100 dilution) and p53 rat anti-horse monoclonal
antibody (1:1,000) was purchased from Nuclea Biotechnologies, Inc.,
(Pittsfield, MA, USA). The mixture was then incubated with normal
horse or sheep serum at room temperature for 20 min and the primary
antibody was added. FHIT, BRCA2 and MLH1 were diluted with 2%
bovine serum albumin (BSA) at ratios of 1:100, 1:100 and 1:50,
respectively. The mixtures were placed in a humidified chamber,
maintained for 12 h in a freezer at 4°C and washed three times with
PBS for 5 min. A secondary antibody [horse anti-rat, binding to the
rat antibodies of MLH1 and p53, or goat anti-rabbit, binding to the
rabbit antibody of BRCA2 and FHIT; dilution 1:200; Thermo Fisher
Scientific, Waltham, MA, USA) was added to the samples and the
mixtures were then incubated for 45 min (2% BSA dilution; 1:200)
and washed three times with PBS for 5 min. Subsequently, the
samples were incubated in ABC (that had been prepared 30 min prior
to use) for 60 min and washed three times with PBS for 5 min. The
samples were then incubated in 3,3′-diaminobenzidine (Vector
Laboratories Inc., Burlingame, CA, USA) and
H2O2, and observed under a microscope
(BX53T-32P01, Olympus Corporation, Tokyo, Japan). Following this,
the reactions were terminated in a timely manner. The samples were
stained with haematoxylin for 15–30 sec, observed under a
microscope (BX53T-32P01, Olympus Corporation), dehydrated in graded
alcohol and processed with xylene to produce transparent slices,
which were mounted with neutral gum (Nanjing Shenglide Biological
Technology Co., Ltd., Nanjing, China).
The negative control consisted of the sera of normal
animals that produce the secondary antibody that blocks
non-specific immunoglobulin responses; this sample did not contain
the primary antibody. A biopsy sample that was known to be positive
for MLH1, FHIT, p53 and BRCA2 served as the positive control.
Result determination
Each slice was observed under a high-power lens
(BX53T-32P01; magnification, ×40) and a minimum of five random
fields were counted to obtain the mean number of positive cells.
Immunohistochemical staining results for FHIT and BRCA2 were
determined based on the semiquantitative method described by
Greenspan et al (10). The
staining intensity scoring was conducted as follows: 1, Lack of
expression or weak expression; 2, moderate expression; and 3,
strong expression. The positive cell classification was determined
as follows: 1, <10% of cells were positive; 2, 10–50% of cells
were positive; and 3, >50% of cells were positive. The final
score was obtained by multiplying the two scores. An FHIT score of
≤3 points indicated decreased or absent expression and was
considered to be negative immune expression, whereas a score of ≥3
indicated a positive immune expression. A BRCA2 score of <3
points indicated reduced expression and was considered to be
negative immune expression, whereas a score of >3 indicated a
positive immune expression. For MLH1, a percentage of <10%
positive cells was considered to be negative immune expression,
whereas a value of ≥10% positive cells was considered to indicate
positive immune expression (14).
With regard to p53, the appearance of three or more brown-yellow or
brown cell nuclei under high-power (magnification, ×400) was
considered to be positive immune and positive protein expression
(13).
Statistical analysis
The results were processed using the SPSS 13.0
statistical software. The χ2 and Spearman’s
correlation tests were used to determine the correlation between
clinical pathology and protein expression data. P<0.05 was
considered to indicate a statistically significant difference.
Results
Immunohistochemical detection of FHIT,
p53, BRCA2 and MLH1
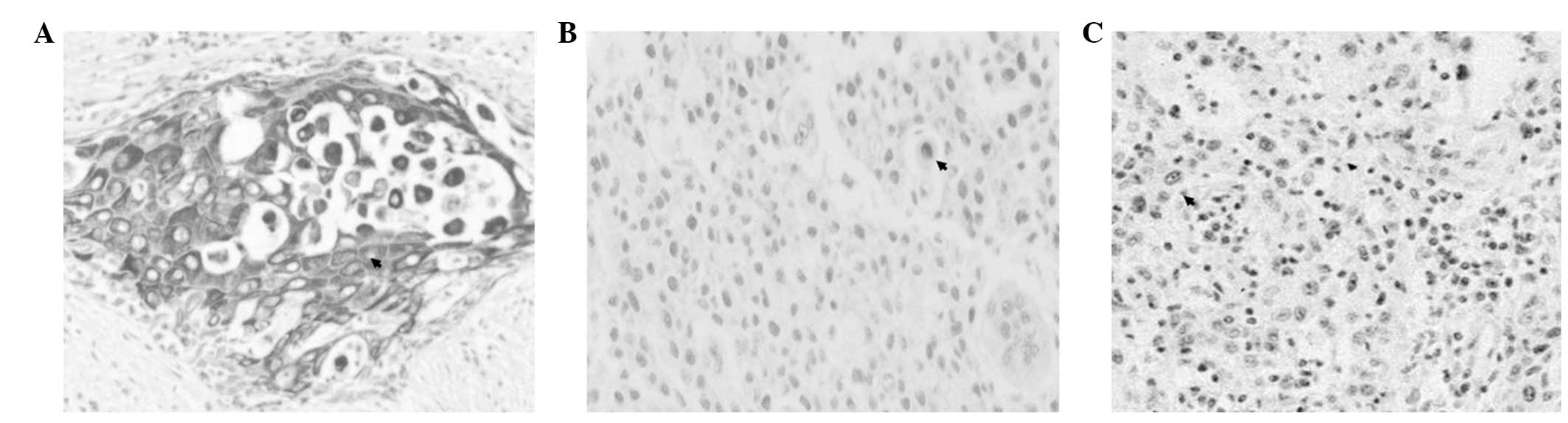
FHIT immunoreactivity was predominantly detected in
the cytoplasm and nucleus and visualised as black coloration
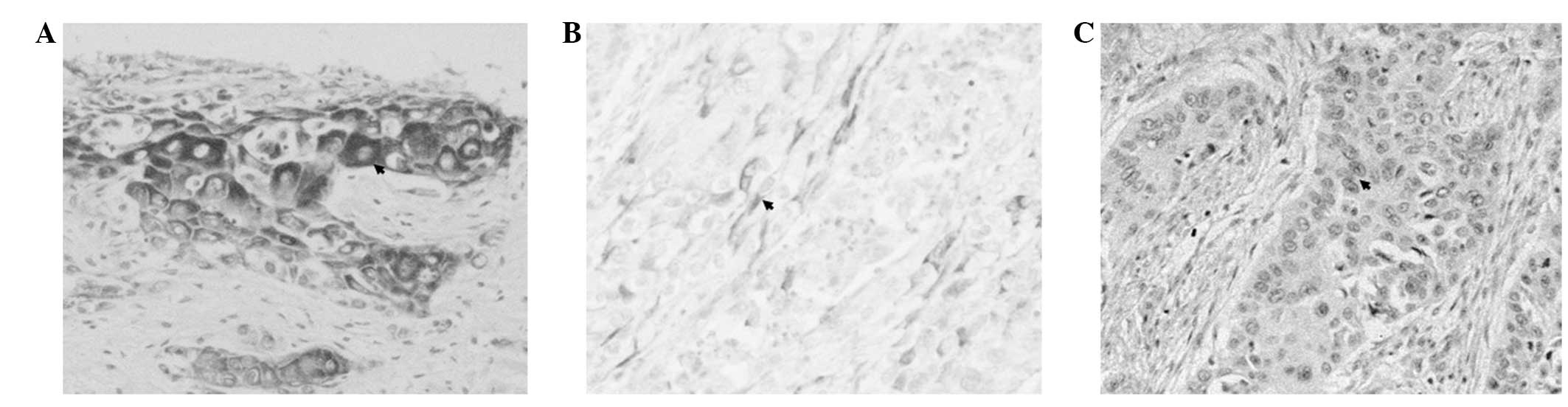
(Fig. 1). BRCA2 immunoreactivity
was predominantly observed in the cytoplasm and membrane as black
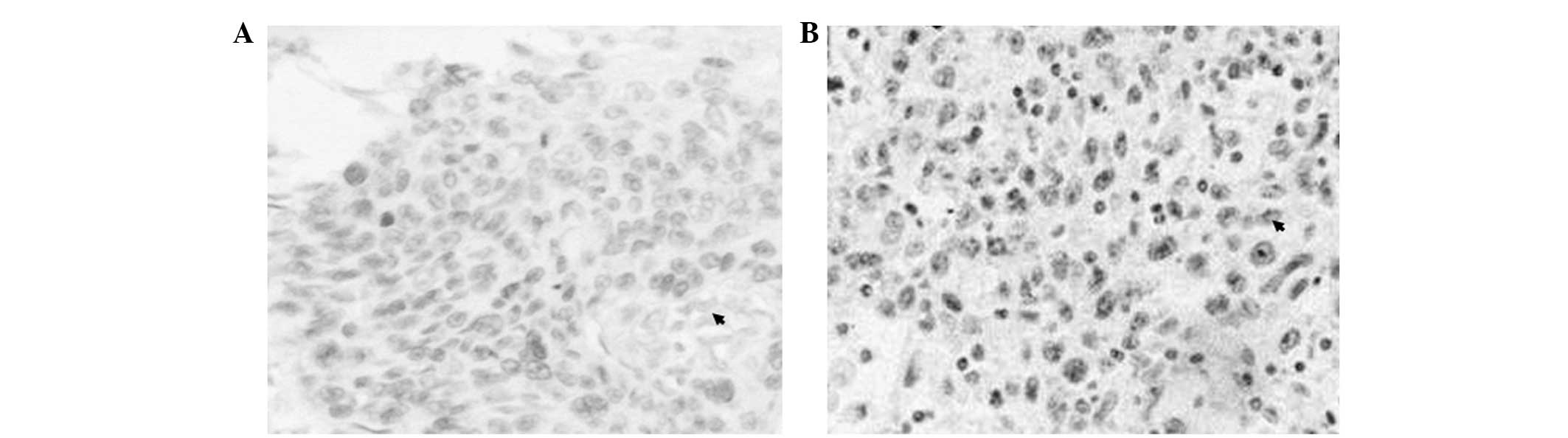
coloration (Fig. 2), and MLH1 and
p53 immunoreactivities were primarily detected in the nucleus as
black coloration (Fig. 3).
Analysis of FHIT, MLH1, BRCA2 and p53
expression levels
The positive expression rate of FHIT (61%;
45/74) in the oesophageal cancer tissues was identified to be lower
than that of the adjacent healthy tissues (97%; 29/30) and the
difference was statistically significant (P<0.01). The positive
expression rate of BRCA2 (50%; 37/74) in the oesophageal
cancer tissues was markedly lower than that in the adjacent healthy
tissues (87%; 26/30), and the difference was identified to be
statistically significant (P<0.01). Furthermore, the positive
expression rate of p53 in the oesophageal carcinoma tissues
of the OCFH + patients (52%; 17/33) was greater than that of the
OCFH − patients (46%; 19/41), although the difference was not
statistically significant (P>0.05). The positive expression rate
of FHIT in the cancer tissues of the OCFH + patients (46%;
15/33) was significantly lower than that of the OCFH − patients
(73%; 30/41), and the difference was statistically significant
(P<0.05; Table IV). The
positive expression rate of BRCA2 in the oesophageal
carcinoma tissues of the OCFH + patients (33%; 11/33) was lower
than that of the OCFH − patients (63%; 26/41) and the difference
was statistically significant (P<0.05). The MLH1 positive
expression rate in the cancer tissues of the OCFH + patients (27%;
9/33) was lower than that of the OCFH − patients (61%, 25/41) and
the difference was statistically significant (P<0.01; Table V).
| Table IVCorrelation analysis of BRCA2,
p53, MLH1 and FHIT expression in the cancer
tissues of oesophageal carcinoma patients with or without a family
history of oesophageal cancer. |
Table IV
Correlation analysis of BRCA2,
p53, MLH1 and FHIT expression in the cancer
tissues of oesophageal carcinoma patients with or without a family
history of oesophageal cancer.
| | BRCA2
negative expression | p53 positive
expression | MLH1
negative expression |
|---|
| |
|
|---|
| FHIT
expression | Cases, n | n (%) | n (%) | n (%) |
|---|
| OCFH + |
| Negative
expression | 18 | 13 (72) | 8 (44) | 12 (67) |
| Positive
expression | 15 | 9 (60) | 9 (60) | 12 (67) |
| OCFH − |
| Negative
expression | 11 | 1 (9) | 6 (55) | 5 (46) |
| Positive
expression | 30 | 14 (47) | 13 (43) | 11 (37) |
| Table VCorrelation analysis of BRCA2,
p53 and MLH1 expression in the cancer tissues of
oesophageal carcinoma patients with or without a family history of
oesophageal cancer. |
Table V
Correlation analysis of BRCA2,
p53 and MLH1 expression in the cancer tissues of
oesophageal carcinoma patients with or without a family history of
oesophageal cancer.
| | p53 +
expression | MLH1 −
expression |
|---|
| |
|
|---|
| BRCA2
expression | Cases, n | n (%) | n (%) |
|---|
| OCFH + |
| Negative
expression | 22 | 11 (50) | 15 (68) |
| Positive
expression | 11 | 6 (55) | 9 (82) |
| OCFH − |
| Negative
expression | 15 | 8 (53) | 5 (33) |
| Positive
expression | 26 | 11 (42) | 11 (42) |
Correlation analysis of FHIT, BRCA2 and
MLH1 expression levels
No significant correlation was observed between the
positive expression rates of FHIT (46 and 73%) and
BRCA2 (33 and 63%), between the positive expression rates of
FHIT (46 and 73%) and MLH1 (27 and 61%), and between
the positive expression rates of FHIT (46 and 73%) and
p53 (52 and 46%) in the oesophageal cancer tissues of all
patients. Furthermore, no significant correlation was identified
between the positive expression rates of BRCA2 (33 and 63%)
and MLH1 (27 and 61%), between the positive expression rates
of BRCA2 (33 and 63%) and p53 (52 and 46%), and
between the positive expression rates of MLH1 (27 and 61%)
and p53 (52 and 46%) (P>0.05; Tables IV–VII).
| Table VIIAssociation between BRCA2,
MLH1, FHIT and p53 positive expression and
clinicopathological characteristics of oesophageal carcinoma. |
Table VII
Association between BRCA2,
MLH1, FHIT and p53 positive expression and
clinicopathological characteristics of oesophageal carcinoma.
| | Positive
expression, n (%) |
|---|
| |
|
|---|
| Clinical
pathology | Cases, n | BRCA2 | MLH1 | FHIT | p53 |
|---|
| Gender |
| Male | 50 | 26 (62) | 27 (54) | 18 (36) | 27 (54) |
| Female | 24 | 11 (46) | 13 (54) | 11 (46) | 11 (46) |
|
Differentiation |
| Well− | 10 | 6 (60) | 8 (80) | 4 (40) | 5 (50) |
| Moderately | 48 | 22 (46) | 23 (48) | 18 (38) | 25 (52) |
| Poorly | 16 | 9 (56) | 9 (56) | 7 (44) | 9 (56) |
| Metastasis |
| Yes | 22 | 11 (50) | 9 (41) | 5 (23) | 13 (59) |
| No | 52 | 26 (50) | 43 (60) | 24 (46) | 25 (48) |
| Infiltration |
|
Mucosa/submucosa | 18 | 12 (67) | 14 (78) | 7 (35) | 10 (56) |
| Muscularis | 20 | 9 (45) | 9 (45) | 7 (35) | 10 (50) |
| Adventitia | 36 | 22 (44) | 17 (47) | 12 (33) | 18 (50) |
Associations between MLH1, BRCA2, and
FHIT expression levels and the clinicopathology of oesophageal
carcinoma
The BRCA2 negative expression rate gradually
decreased in the well− (60%; 6/10), moderately (46%; 22/48) and
poorly (56%; 9/16) differentiated cancer tissues, however, the
differences between results were not significant (P>0.05). The
negative expression rates of MLH1 in the well−, moderately,
and poorly differentiated oesophageal cancer tissues were 80%
(8/10), 48% (23/48) and 56% (9/16), respectively. These values
initially decreased and subsequently increased, although the
changes were not statistically significant (P>0.05). The
negative expression rates of FHIT in the well−, moderately,
and poorly differentiated carcinoma tissues were 40% (4/10), 38%
(18/48) and 44% (7/16), respectively. The negative expression
gradually decreased (P>0.05). The negative expression rates of
p53 in the well−, moderately, and poorly differentiated
carcinoma tissues were 50% (5/10), 52% (25/48) and 56% (9/16),
respectively. However, the difference was not statistically
significant (P>0.05).
The expression levels of BRCA2, FHIT,
MLH1 and p53 in the lymph node metastasis group
showed no statistically significant difference with those of the
lymph node non-metastasis group. As the extent of tumour invasion
increased (mucosa and submucosa to muscularis to adventitia), the
negative expression rates of BRCA2 and FHIT gradually
decreased (67 to 45 to 44% vs. 56 to 35 to 33%), the p53
negative expression rates gradually decreased (56 to 50 to 50%),
and the MLH1 negative expression rates initially decreased
and then increased (78 to 45 to 47%). However, these changes were
not statistically significant (P>0.05). In male patients, the
negative expression rate of BRCA2 and the negative
expression rate of p53 were marginally higher when compared
with female patients (52 and 46 vs. 54 and 46%), whereas the
FHIT negative expression rate was marginally lower than that
of the females (36 vs. 46%). However, the differences were not
statistically significant (P>0.05). The negative expression
rates of MLH1 in males and females showed no statistically
significant difference (Tables
VII).
Discussion
The high incidence of oesophageal cancer within
families is a common phenomenon in geographical regions with a high
incidence of oesophageal cancer, with members of families with a
history or oesophageal cancer being associated with a higher risk
of prevalence. A previous study demonstrated that various fragile
sites are present in the members of families with a high incidence
of oesophageal cancer (8).
Approximately 89% of subjects of the high incidence families were
carriers of fragile sites (primarily the common fragile sites),
which were vertically inherited according to the Mendelian
monogenic autosomal recessive model of blood relatives (15). Therefore, oesophageal cancer may be
associated with a familial predisposition to fragile sites, as well
as chromosomal instability (8). In
oesophageal cancer patients and their children, the rates of
chromosomal aberrations and appearance of fragile sites
significantly increased, when compared with healthy individuals
(16). Furthermore, the consistent
compliance rates of fragile sites, oncogenes and cancer breakpoints
in oesophageal cancer patients were also significantly higher than
those in the control group. This result indicates that chromosomal
instability increases the susceptibility of an individual to cancer
and may be the genetic basis of oesophageal cancer (16).
In the present study, OCFH + patients showed
significantly higher negative expression rates of FHIT,
BRCA2 and MLH1 when compared with the OCFH −
patients. These results indicate that FHIT may be involved
in the genesis of oesophageal cancer and is possibly closely
associated with the high susceptibility of family members in the
region of Linzhou, of high oesophageal cancer incidence. In
addition, the BRCA2, MLH1 and FHIT genes may
be involved in the genesis of oesophageal cancer in susceptible
populations, and the abnormal changes in BRCA2 and
MLH1 expression are important molecular events in the
occurrence of oesophageal cancer in OCFH + patients. These proteins
may be significant molecular bases for the genesis of a high
susceptibility of individuals to oesophageal carcinoma. In the
present study, the positive expression rates of p53 were
markedly high in all of the oesophageal cancer patients, regardless
of the family medical history. Although the rates are higher in the
OCFH + group, the difference was not significant, which indicates
that p53 is associated with additional predisposing factors
that exert synergistic effects on oesophageal cancer
susceptibility. Thus, the association between p53 and a high
susceptibility to oesophageal cancer requires further
investigation. As an identified tumour suppressor gene, FHIT
is positioned on the third chromosome (3p14.2), which contains the
majority of the active fragile sites of the human genome, as well
as numerous chromosomal abnormalities. A chromosomal exception that
occurs in this site commonly leads to FHIT inactivation and
abnormal protein expression (9).
Furthermore, the BRCA2 gene is located at chromosome 13q12,
where a high frequency of allelic loss in tumours occurs (17). Therefore, the BRCA2 protein is
essential in maintaining the stability of chromosomes and is
involved in the DNA repair process. BRCA2 is activated by
RAD51 and is involved in cell cycle regulation (18). In addition, the BRCA2 gene
203G>A polymorphism may be associated with susceptibility to
oesophageal cancer (19).
BRCA2 mutation causes single- or double-strand break repair
defects that lead to chromosomal instability; the incidence of
BRCA2 gene mutations in OCFH + patients was found to be
significantly higher than that in OCFH − patients (20). This result demonstrates that
BRCA2 is closely associated with a genetic susceptibility to
familial oesophageal cancer. Mismatch repairs primarily indicate an
excision and repair process that is directed towards the nucleotide
of the contralateral DNA chain. In addition to DNA repair, mismatch
repair also transfers DNA damage signals to the apoptosis
initiation system; DNA damages that cannot be repaired induce
apoptosis (11,12). Additionally, the carcinogenic
nitrosamine, methylbenzylnitrosamine inactivates or reduces the
expression of mismatch repair genes in oesophageal cancer and
inhibits the mismatch repair function of cells, thus increasing
cancer risk (21).
Damage to the FHIT gene, which is closely
associated with chromosomal abnormalities, may result from DNA
repair deficiencies (22). Previous
studies have shown that FHIT expression levels are
significantly increased in a number of DNA repair-deficiency
tumours, such as breast cancer and colorectal cancer (10,14,21,22).
Abnormal conditions, such as chromosome breakage are observed in
cell lines with mismatch repair and double-strand break repair gene
defects (23). This phenomenon
indicates that DNA repair deficiencies significantly affect
chromosomal stability and increase the susceptibility of a number
of fragile gene sites, such as FHIT to abnormalities.
In conclusion, it is hypothesised that individuals
who are susceptible to oesophageal cancer may exhibit a high
incidence of chromosomal instability. Therefore, the risk of
chromosomal abnormality is higher when individuals are affected by
the same carcinogenic factors in familiar environments. This
condition causes the abnormal expression of a number of key genes
(such as oncogenes or cancer suppressor genes) located in certain
unstable areas (such as fragile sites), which subsequently leads to
earlier carcinoma genesis. In the present study, however,
FHIT expression in oesophageal cancer patients showed no
significant association with BRCA2 and MLH1 negative
expression regardless of the family medical history. No significant
correlation was identified between the negative expression of
BRCA2 and MLH1, which indicates that the high
susceptibility to oesophageal cancer is a complicated synergy that
involves multiple genes. By contrast, the correlation among
FHIT, BRCA2 and MLH1 expression involves
simple, causal connections rather than multiple factors. In
addition to BRCA2 and MLH1, other important factors
also affect FHIT expression levels. The synergistic effect
of FHIT, BRCA2, MLH1 and other relevant
factors may be the molecular bases for the genesis of oesophageal
cancer. Further discussion of the association between DNA repair,
chromosomal stability, and FHIT, BRCA2 and MLH
expression in susceptible populations may contribute to elucidating
the molecular basis for the high susceptibility of
oesophageal-cancer families in regions with a high incidence of
oesophageal cancer.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81272227).
References
|
1
|
Du BL: Esophageal Carcinoma. Beijing:
China Science and Technology Press; pp. 30–60. 1994
|
|
2
|
Wang LD, Gao WJ, Yang WC, et al: Prelimary
analysis of the statistics on 3933 cases with esophageal cancer and
gastric cardia cancer from the subjects in the People’s Hospital of
Linzhou in 9 years. J Henan Med Univ. 32:9–11. 1997.(In
Chinese).
|
|
3
|
Lu JB, Yang WX, Zu SK, et al: Cancer
mortality and mortality trends in Henan, China, 1974–1985. Cancer
Detect Prev. 13:167–173. 1988.
|
|
4
|
Shi QL, Xu DZ and Sun C: Study on family
aggregation of esophageal cancer in Linzhou city. Zhonghua Yu Fang
Yi Xue Za Zhi. 34:269–270. 2000.(In Chinese).
|
|
5
|
Hu N, Dawsey SM, Wu M, et al: Familial
aggregation of oesophageal cancer in Yangcheng County, Shanxi
Province, China. Int J Epidemiol. 21:877–882. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Carter CL, Hu N, Wu M, et al: Segregation
analysis of esophageal cancer in 221 high-risk Chinese families. J
Natl Cancer Inst. 84:771–776. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hu N: Genetic epidemiclogy of esophageal
cancer: 10-year follow-up of 622 positive families in Yangcheng
County. Zhonghua Yi Xue Za Zhi. 70:679–681. 1990.(In Chinese).
|
|
8
|
Zhou HY, Liang M, Li SJ, Gao XK and Tao
DM: The study of four chromosomal fragile site of high incidence
familial esophageal cancer. Chinese Journal of Medical Genetics.
4:113–115. 1995.
|
|
9
|
Liu YL, Li XM, Jin GL, et al: The study of
FHIT expression and HPV testing in high incidence esophageal
squamous cell carcinoma in Ci County Hebei Province. Cancer.
22:492–494. 2003.
|
|
10
|
Greenspan DL, Connolly DC, Wu R, et al:
Loss of FHIT expression in cervical carcinoma cell lines and
primary tumors. Cancer Res. 57:4692–4698. 1997.PubMed/NCBI
|
|
11
|
Goode EL, Ulrich CM and Potter JD:
Polymorphisms in DNA repair genes and associations with cancer
risk. Cancer Epidemiol Biomarkers Prev. 11:1513–1530.
2002.PubMed/NCBI
|
|
12
|
Karran P, Offman J and Bignami M: Human
mismatch repair, drug-induced DNA damage, and secondary cancer.
Biochimie. 85:1149–1160. 2003. View Article : Google Scholar
|
|
13
|
Wang LD, Shi ST, Zhou Q, et al: Changes in
p53 and cyclin D1 protein levels and cell proliferation in
different stages of human esophageal and gastric-cardia
carcinogenesis. Int J Cancer. 59:514–519. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Giarnieri E, Mancini R, Pisani T,
Alderisio M and Vecchione A: Msh2, Mlh1, Fhit, p53, Bcl-2, and Bax
Expression in invasive and in situ squamous cell carcinoma of the
uterine cervix. Clin Cancer Res. 6:3600–3606. 2000.PubMed/NCBI
|
|
15
|
Hao D, Wang G, Yin Z, et al: Systematic
large-scale study of the inheritance mode of Mendelian disorders
provides new insight into human diseasome. Eur J Hum Genet. Jan
22–2014.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cao X, Li LY, Xie J, Cao Y and Li Y: The
study of chromosome fragile site in esophageal cancer patients and
their first-degree relatives. Cancer. 15:349–351. 1996.
|
|
17
|
Huang J, Hu N, Goldstein AM, et al: High
frequency allelic loss on chromosome 17p13.3-p11.2 in esophageal
squamous cell carcinomas from a high incidence area in northern
China. Carcinogenesis. 21:2019–2026. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vaughn JP, Cirisano FD, Huper G, et al:
Cell cycle control of BRCA2. Cancer Res. 56:4590–4594.
1996.PubMed/NCBI
|
|
19
|
Hu N, Li G, Li WJ, et al: Infrequent
mutation in the BRCA2 gene in esophageal squamous cell carcinoma.
Clin Cancer Res. 8:1121–1126. 2002.PubMed/NCBI
|
|
20
|
Hu N, Wang C, Han XY, et al: Evaluation of
BRCA2 in the genetic susceptibility of familial esophageal cancer.
Oncogene. 23:852–858. 2004. View Article : Google Scholar
|
|
21
|
Bertrand P, Tishkoff DX, Filosi N,
Dasgupta R and Kolodner RD: Physical interaction between components
of DNA mismatch repair and nucleotide excision repair. Proc Natl
Acad Sci USA. 95:14278–14283. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pekarsky Y, Zanesi N, Palamarchuk A,
Huebner K and Croce CM: FHIT: from gene discovery to cancer
treatment and prevention. Lancet Oncol. 3:748–754. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ingvarsson S, Agnarsson BA,
Sigbjornsdottir BI, et al: Reduced Fhit expression in sporadic and
BRCA2-linked breast carcinomas. Cancer Res. 59:2682–2689.
1999.PubMed/NCBI
|