Introduction
Schwannomas are a type of uncommon benign nerve
sheath tumor originating from the Schwann cells of the neural crest
and accounting for ~5% of all head and neck tumors (1). Schwannomas always present as
encapsulated, firm, slow-growing and painless masses, the majority
of which are located in the parotid gland or infratemporal fossa.
The tumors have also been reported in the mandible, but are rarely
observed in the larynx. Symptoms rarely present themselves, but
include a sore throat, difficulty in swallowing, a change of voice
or a globus sensation (2–4). The use of laser applications in
otorhinolaryngology has undergone significant advances over the
past several years; laser technology is now used in a wide variety
of procedures, and has become the primary treatment modality or
standard of care for many otorhinolaryngology conditions (5). CO2 laser surgery is surgery
using a CO2 laser (instead of a scalpel) to cut tissue
(6). Examples include the use of a
laser scalpel in otherwise conventional surgery, and soft tissue
laser surgery, in which the laser beam vaporizes soft tissue with
high water content (7,8). Conservative surgery has always been
proposed for the treatment of this disease. The current study
presents the case of a schwannoma arising in the supraglottic area
in a 36-year-old male. Written informed consent was obtained from
the patient.
Case report
A 36-year-old male presented at the The First
Affiliated Hospital of Chongqing Medical University (Chongqing,
China) with a two-week history of hoarseness. According to the
patient, other symptoms, such as a sore throat, globus sensation
and difficulty in swallowing and breathing, were not present.
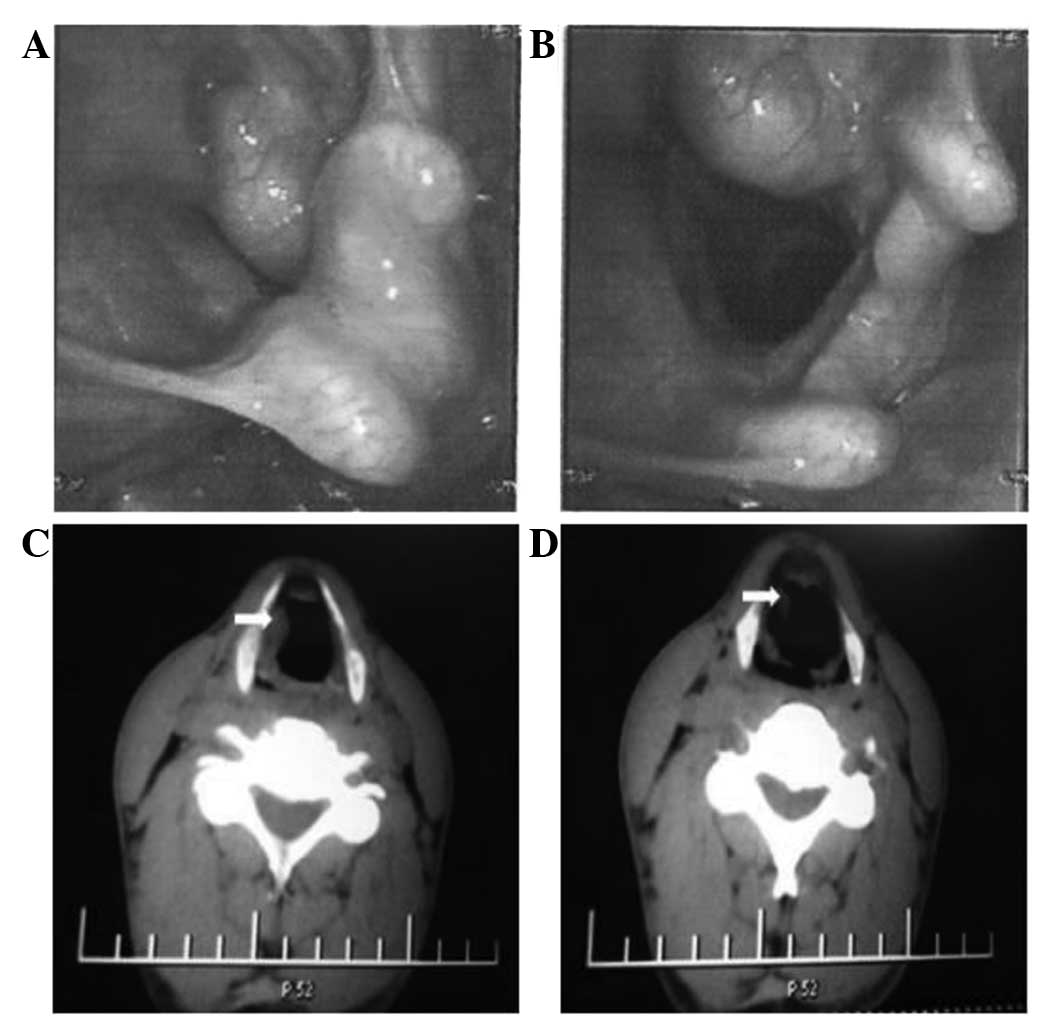
Electronic laryngoscopy showed a submucosal mass at the level of
the right supraglottic area (Fig. 1A
and B). A computed tomography scan of the larynx showed an
8×11-mm expansile mass in the right supraglottic area, with
well-defined boundaries. There was no enlargement of the lymph
nodes in the neck (Fig. 1C and D).
The differential diagnosis of the tumor included squamous cell
carcinoma, fibroma, neurofibroma, lymphoma and schwannoma.
Resection of the tumor was performed by
CO2 laser through an endoscopic transoral approach under
general anesthesia. During the surgery, the tumor was completely
resected along the tumor boundary. No nerves were connected
caudally to the tumor. Histopathological examination of the frozen
section demonstrated that the tumor was mainly composed of active
spindle cells. Next, ~2 mm of tissue was resected along the edge of
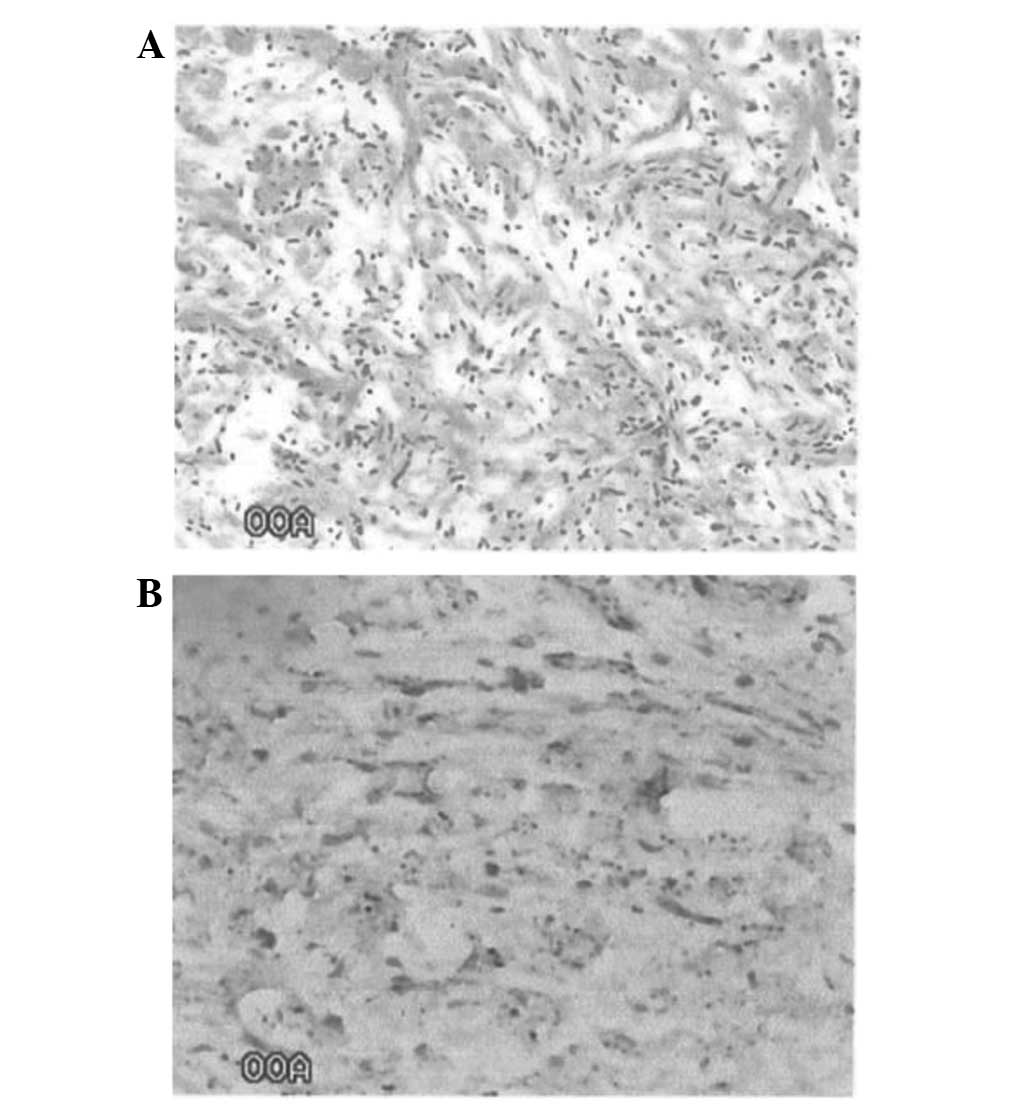
the tumor by CO2 laser. Histopathological examination
subsequent to the surgery demonstrated benign spindle cell lesions
(Fig. 2A). Immunohistochemically,
the tumor was strongly positive for cluster of differentiation 56
and S-100 (Fig. 2B), but negative
for smooth muscle actin, vimentin and maltose-binding protein. On
the basis of these findings, the tumor was diagnosed as a
schwannoma of the larynx, originating from the distal portion of
the internal branch of the superior laryngeal nerve or the
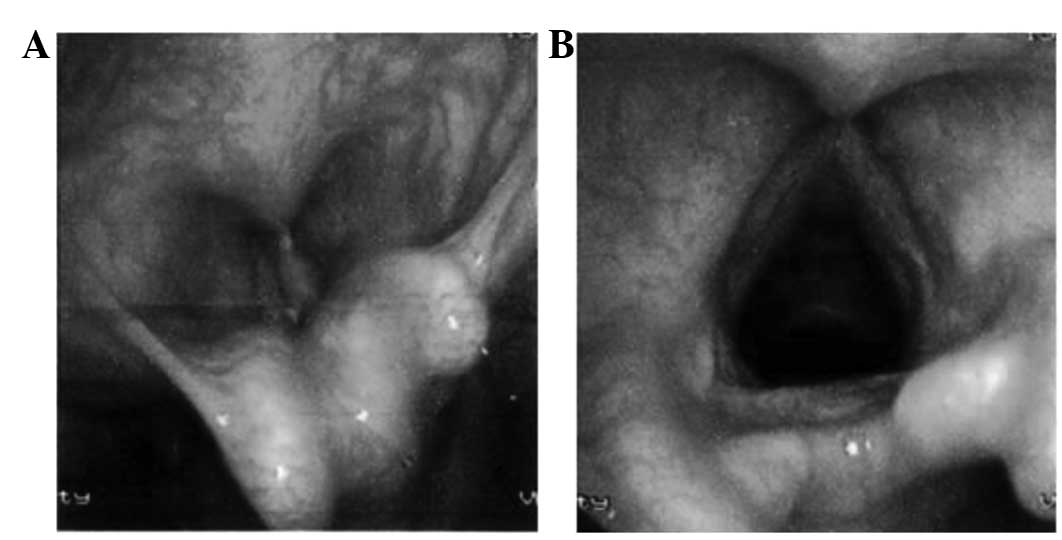
recurrent laryngeal nerve. The patient has since been followed up
for 12 months and no evidence of recurrence has been observed
(Fig. 3A and B).
Discussion
Schwannomas are slow-growing, benign tumors of the
nerve sheath, first described by Verocay in 1908 (9). Since then, few cases have been
reported in the literature (10). A
study by Enzinger and Weiss (11)
suggested that the histological diagnosis of schwannoma could be
characterized by three features: i) Encapsulation; ii) the presence
of Antoni A and B areas; and iii) a positive reaction for S-100.
The present case exhibited each of these features, and the tumor
was well-defined; these findings eventually led to a diagnosis of
schwannoma.
The majority of laryngeal schwannomas occur in the
supraglottic area and are present at any age. The etiology of
schwannomas is not well understood. Surgical excision is the main
strategy for treatment. Furthermore, the preservation of laryngeal
function and protection of the laryngeal mucosa from injury during
surgery must also be guaranteed. However, recurrences have been
reported by long-term follow-up subsequent to conventional surgery
(2).
CO2 lasers are widely used to remove thin
layers from the surface of the mucosa without undermining the
deeper layers. This procedure can be performed with fairly little
bleeding, swelling, pain or scarring. The lasers are more precise
than scalpels and the high temperature generated by the lasers aids
in cleaning the edges of the body tissue that it is cutting,
reducing the risk of infection and recurrence. Using this approach,
the surgery time may be reduced and the healing time may be
shortened. CO2 lasers now play an increasingly important
role as a minimally invasive alternative to conventional surgical
interventions for patients in a number of oncology services
(12).
Although differing surgical approaches for removing
laryngeal schwannomas have been discussed in the literature,
including endoscopic removal and a laryngofissure approach
(13,14). The use of a CO2 laser via
a transoral approach can be applied in patients with early-stage
laryngeal carcinoma and atlanto-axial vertebral chronic dislocation
(15) In the present case, the
tumor was resected by CO2 laser, demonstrating that safe
removal of the tumor is possible using this approach, without
severe injury to the laryngeal mucosa and with low recurrence.
References
|
1
|
Fournier J, St Pierre S and Morrissette Y:
Neurilemmoma of the parapharyngeal space. Report of three cases and
review of the literature. J Otolaryngol. 8:439–442. 1979.PubMed/NCBI
|
|
2
|
Ridder GJ, Kayser G, Teszler CB and
Pfeiffer J: Solitary fibrous tumors in the head and neck: new
insights and implications for diagnosis and treatment. Ann Otol
Rhinol Laryngol. 116:265–270. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zbären P and Markwalder R: Schwannoma of
the true vocal cord. Otolaryngol Head Neck Surg. 121:837–839. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sanghvi V, Lala M, Borges A, et al:
Lateral thyrotomy for neurilemmoma of the larynx. J Laryngol Otol.
113:346–348. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Weir N: Otorhinolaryngology. Postgrad Med
J. 76:65–69. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jerjes W, Hamdoon Z and Hopper C: CO2
lasers in the management of potentially malignant and malignant
oral disorders. Head Neck Oncol. 30:172012. View Article : Google Scholar
|
|
7
|
Ayari S, Aubertin G, Girschig H, et al:
Management of laryngomalacia. Eur Ann Otorhinolaryngol Head Neck
Dis. 130:15–21. 2013. View Article : Google Scholar
|
|
8
|
Remacle M and Lawson G: Carcinoma of the
larynx. Surgery: general aspects. Acta Otorhinolaryngol Belg.
46:175–186. 1992.PubMed/NCBI
|
|
9
|
Verocay J: Multiple geschwulste als
Systemerkrankung am nervosen Apparate. Festschrift fur Chiari, Wein
and Leipzig. 378–415. 1908.
|
|
10
|
Taylor J, Stiefel M and Park SY:
Schwannoma of the true vocal fold: a rare diagnosis. Ear Nose
Throat J. 85:52–53. 592006.PubMed/NCBI
|
|
11
|
Enzinger FM and Weiss SW: Benign tumors of
peripheral nerves. Soft Tissue Tumors. 2nd edition. Mosby Inc.; St.
Louis: pp. 725–735. 1988
|
|
12
|
Stafford RJ, Fuentes D, Elliott AA, et al:
Laser-induced thermal therapy for tumor ablation. Crit Rev Biomed
Eng. 38:79–100. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lo S and Ho WK: Schwannoma of the larynx -
an uncommon cause of vocal cord immobility. Hong Kong Med J.
10:131–133. 2004.PubMed/NCBI
|
|
14
|
Cadoni G, Bucci G, Corina L, et al:
Schwannoma of the larynx presenting with difficult swallowing.
Otolaryngol Head Neck Surg. 122:773–774. 2000.PubMed/NCBI
|
|
15
|
Werner JA, Dunne AA, Folz BJ and Lippert
BM: Transoral laser microsurgery in carcinomas of the oral cavity,
pharynx, and larynx. Cancer Control. 9:379–386. 2002.PubMed/NCBI
|