Introduction
Osteoid osteoma is a type of benign bone tumor,
which was first described by Jaffe in 1935 (1). It is a rare condition, which accounts
for only 3% of primary bone tumors. Individuals aged between 5 and
24 years old are the most commonly affected (2). The main symptom of the disease is pain
that worsens at night, which may be alleviated by aspirin. Current
treatment modalities include surgical excision, as well as less
invasive techniques (3,4). After treatment, symptoms can be
controlled. The most commonly affected sites are the long bones of
the lower extremities and the patient outcome is good. The ribs are
rarely involved. The present study describes two cases of osteoid
osteomas located in the rib. Written informed consent was obtained
from both patients.
Case reports
Case 1
A 22 year-old male presented with back pain in the
right side that had been apparent for one year. The pain was
intermittent and more severe at night, while it was reduced by
taking aspirin. A local hospital was unable to establish a
diagnosis and, thus, the patient was referred to the Beijing
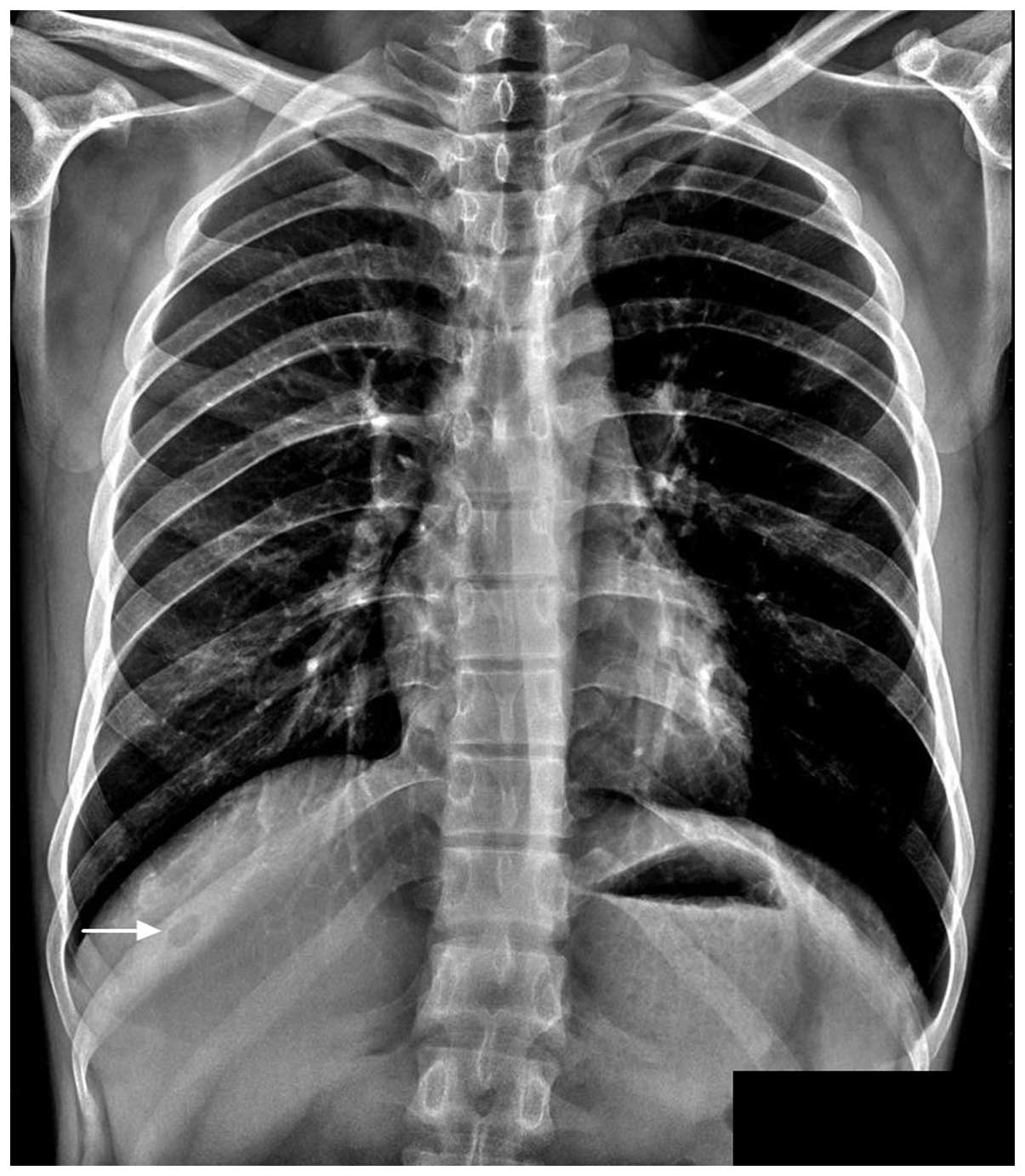
Jishuitan Hospital (Beijing, China) in December 2011. A fixed
tenderness point was identified on the right side of the back. An
X-ray image revealed a radiolucent lesion located in the tenth rib
of the right side, which exhibited prominent sclerosis surrounding
a central radiolucent nidus (Fig.
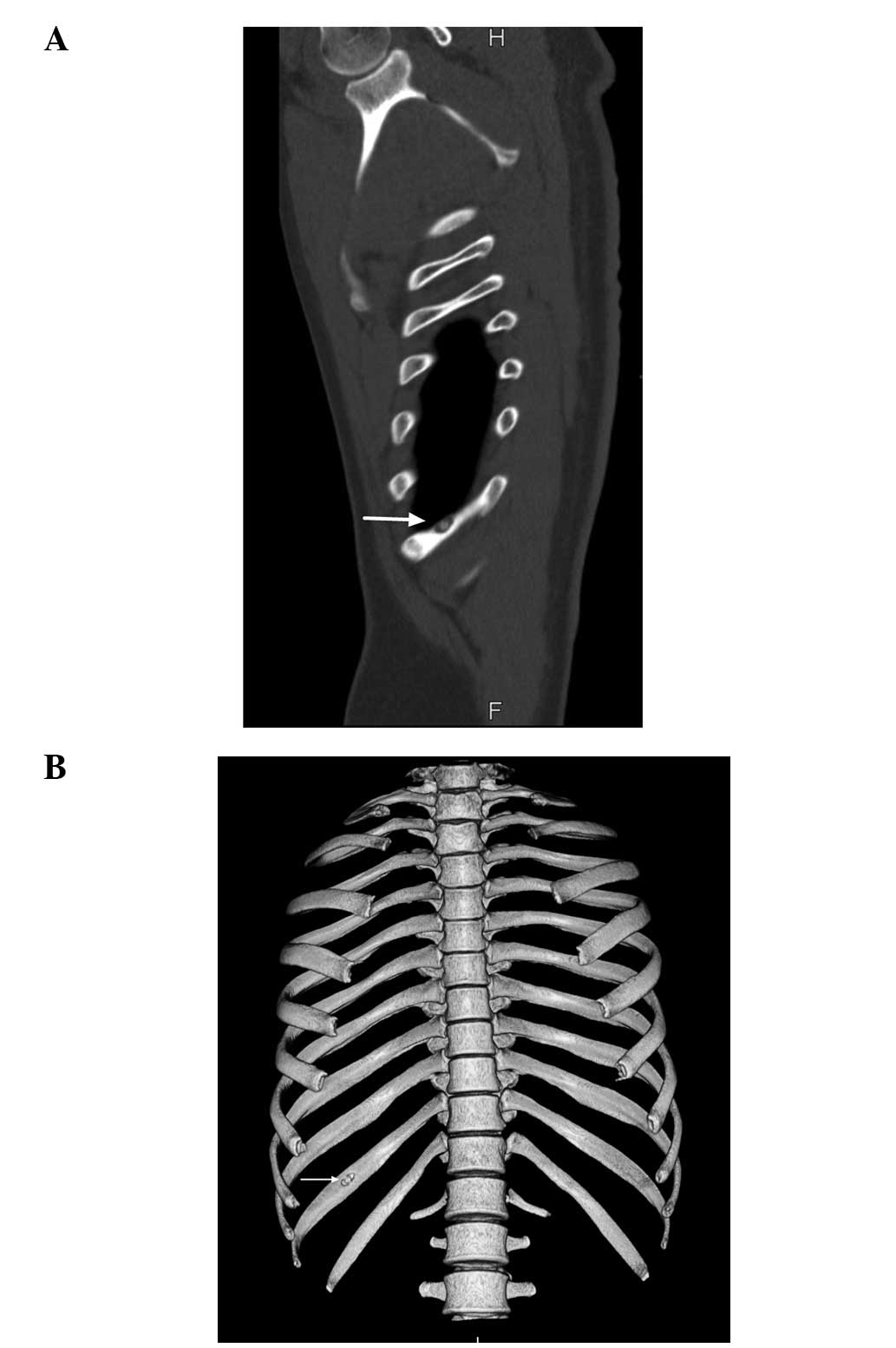
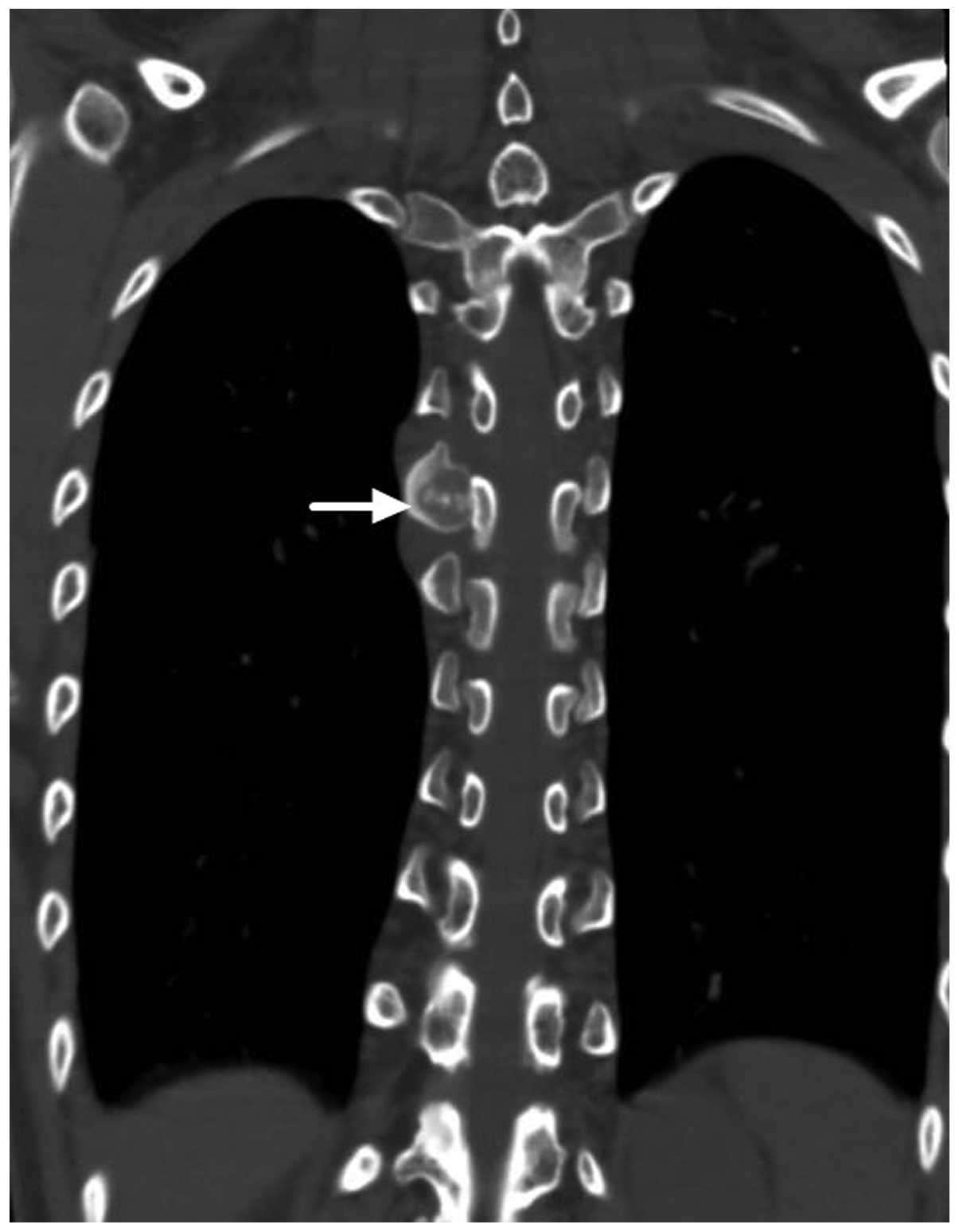
1). A computed tomography (CT) scan revealed clear central
calcification of the lesion, which was located in the visceral side
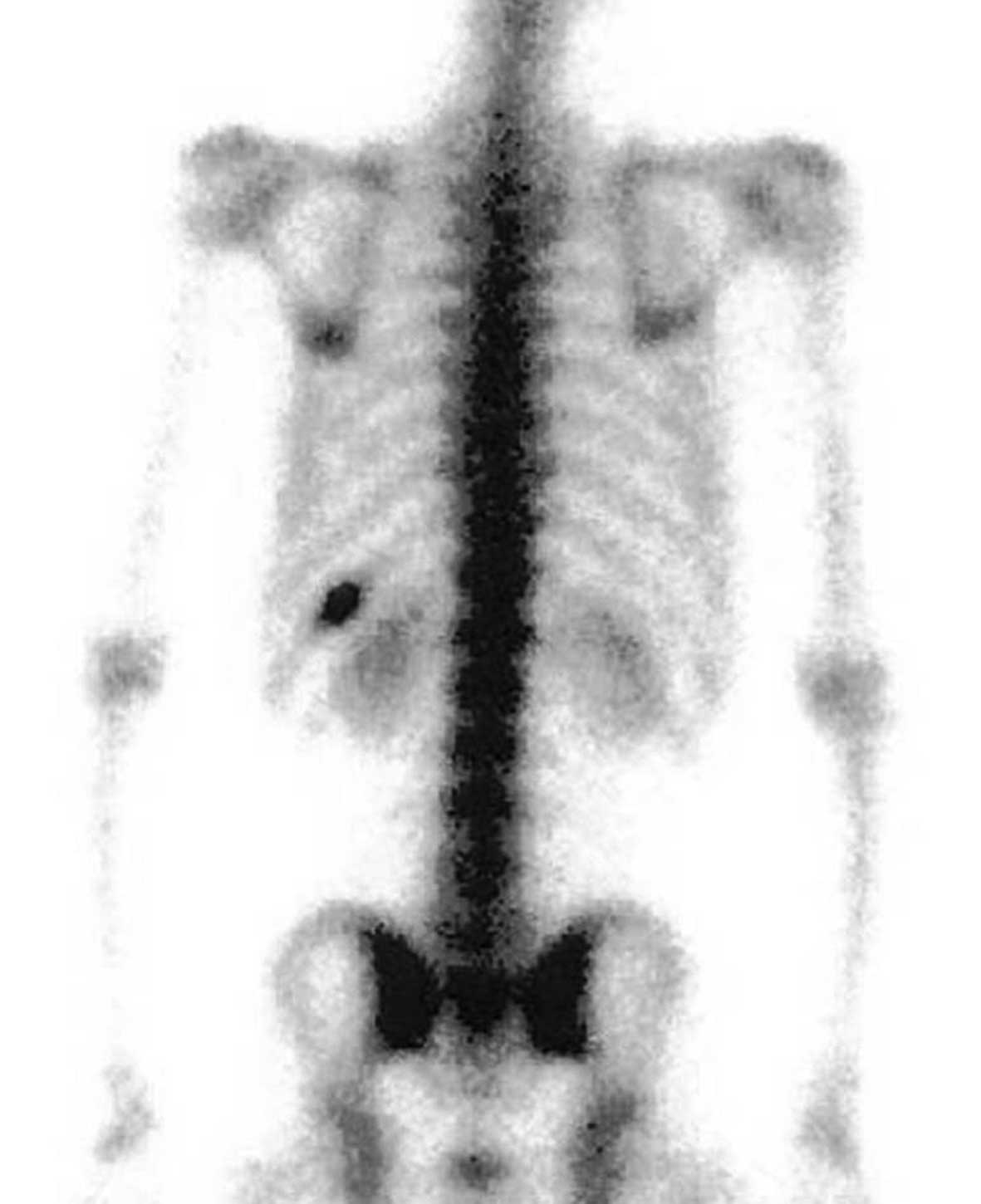
of the rib at the reconstructed view (Fig. 2). Technetium-99m medronic acid bone
scintigraphy revealed a single focus of intense uptake in the
posterior shaft of the right tenth rib (Fig. 3). A diagnosis of osteoid osteoma was
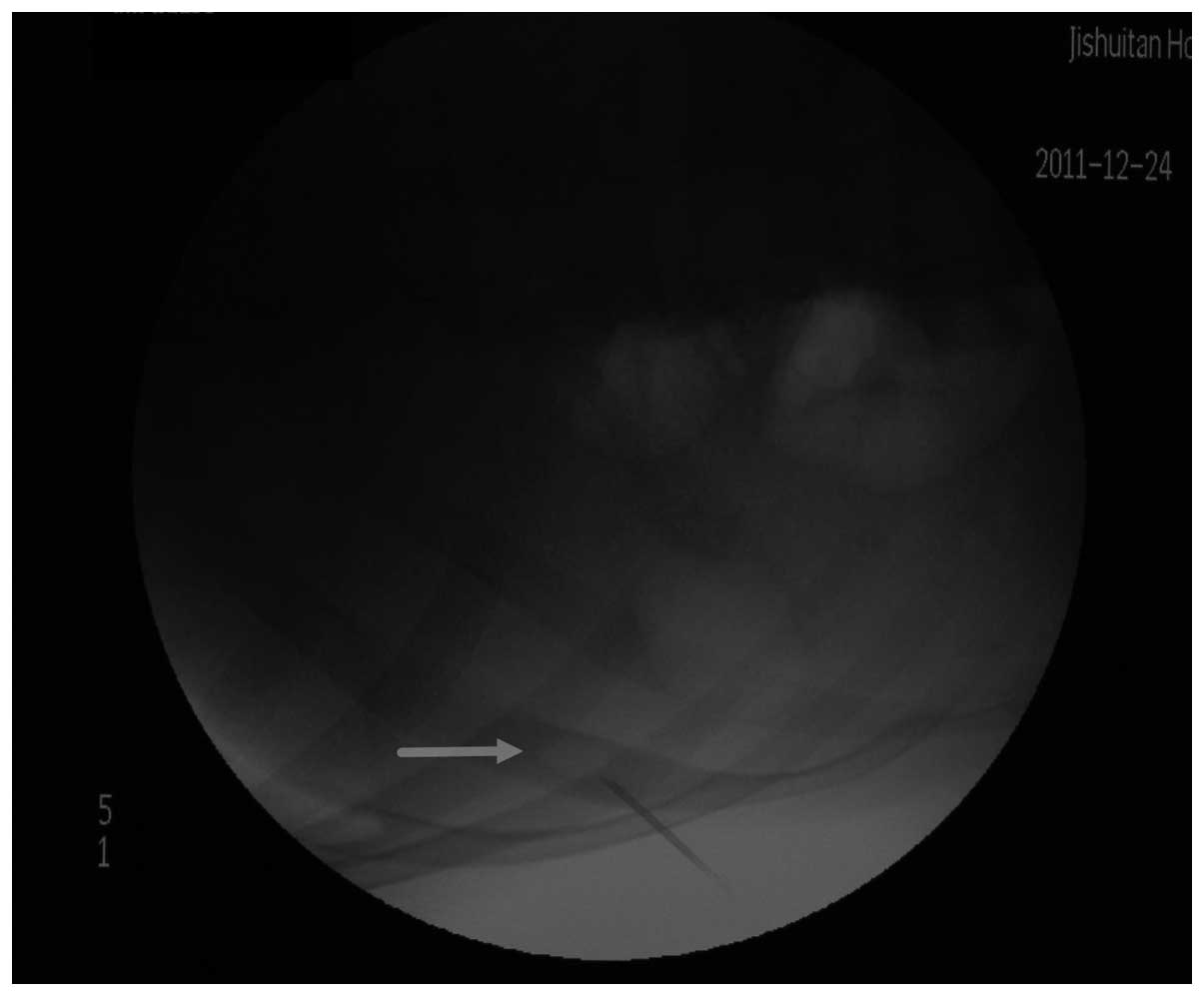
subsequently established. A C-arm fluoroscopic device (BV Libra,
Philips, Amsterdam, Netherlands) was used to locate and completely
resect the lesion during surgery (Fig.
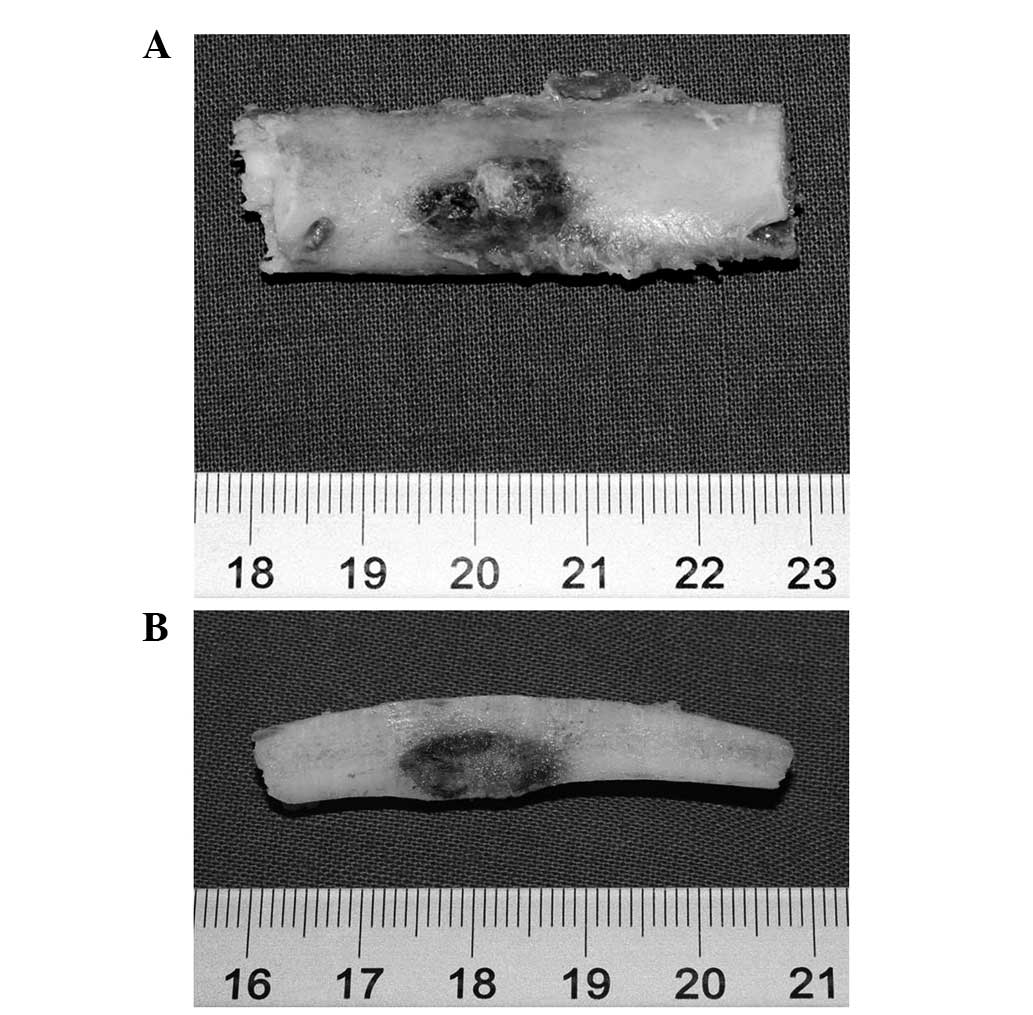
4). The specimen revealed that the visceral side of the rib was
involved. In the cross section, the tumor was located in the cortex
of the rib. The nidus and central calcification were clearly
observed in the gross specimen (Fig.
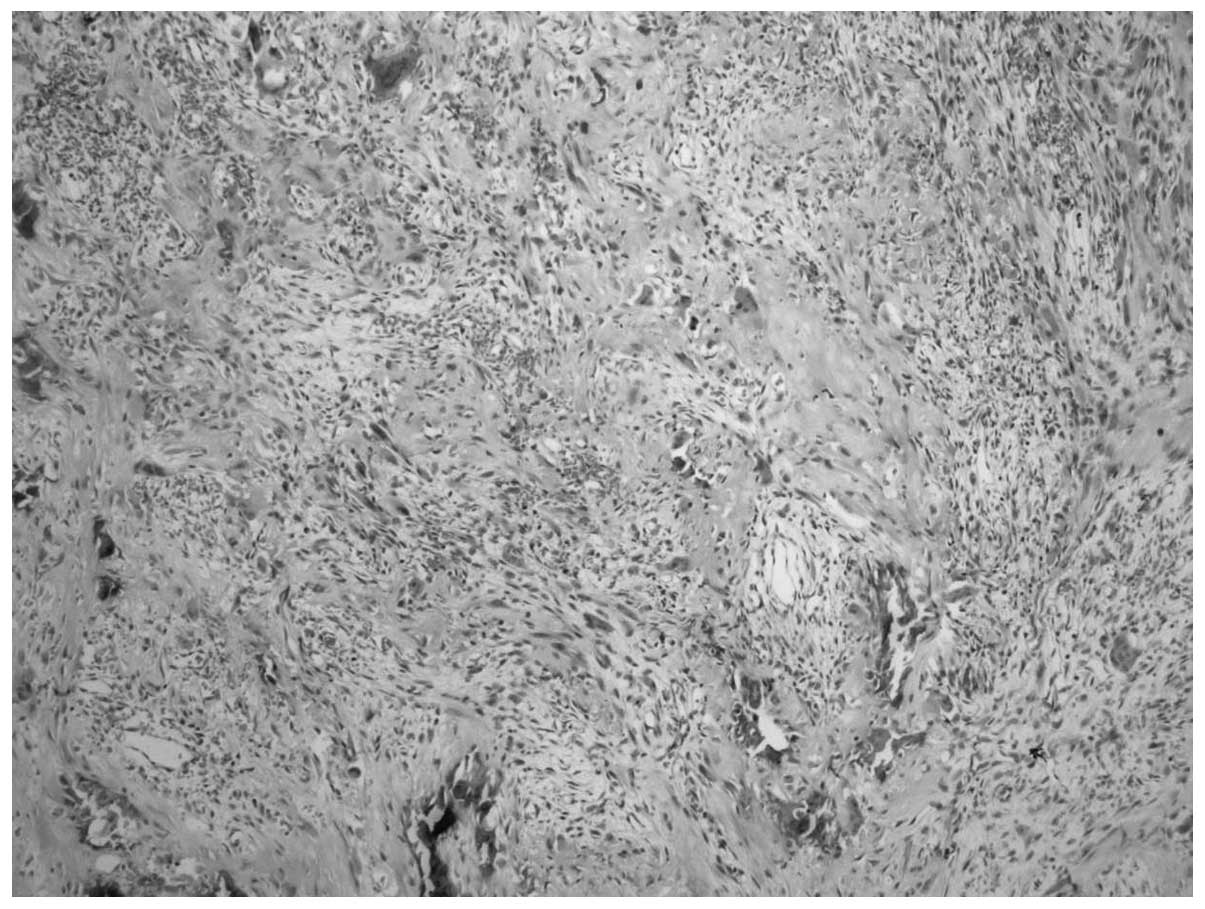
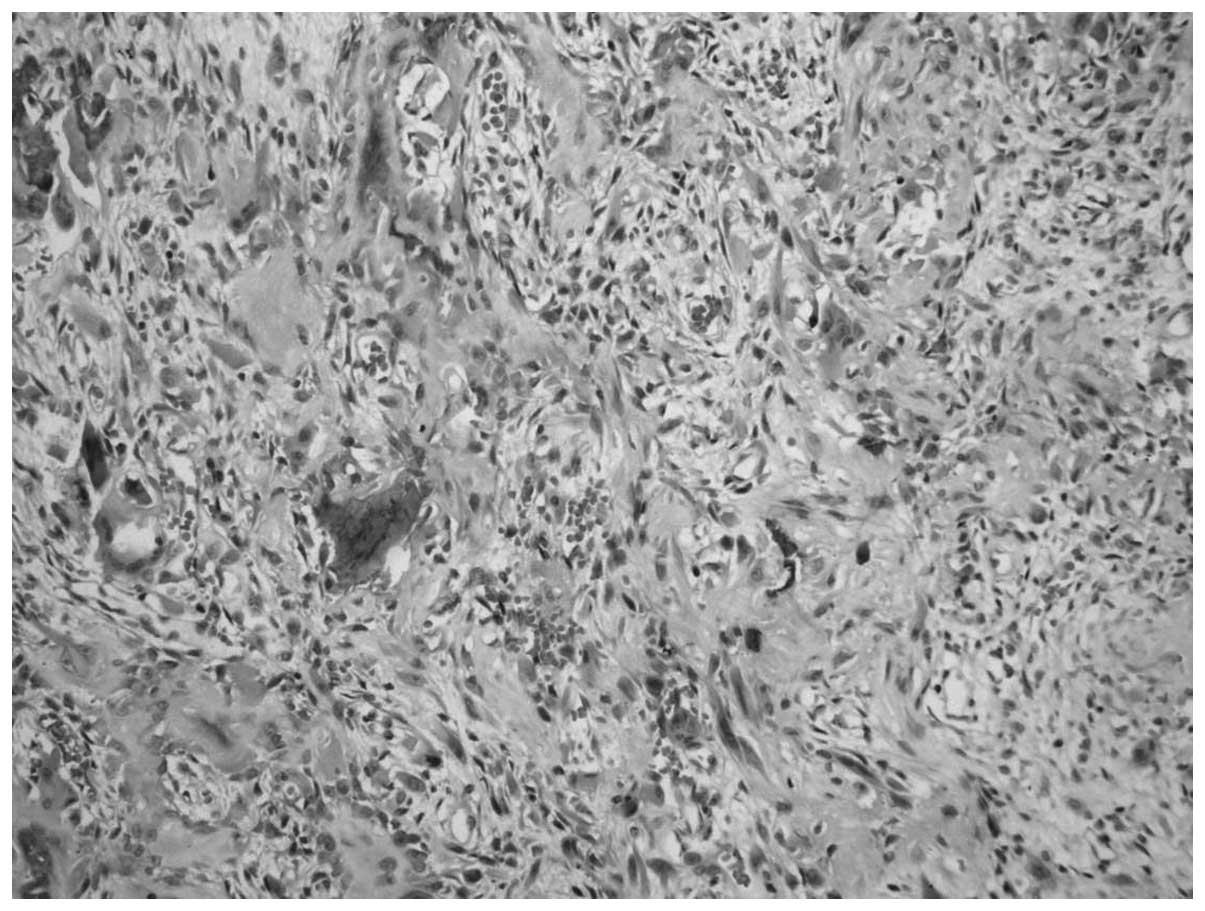
5). A high-power photomicrograph (BX41, Olympus Corporation,
Tokyo, Japan) revealed the presence of osteoid tissue in a
background stroma of fibrovascular tissue and thin trabeculae
inter-anastomosing with a single layer of osteoblasts. The
intertrabecular space was filled with fibrovascular stroma
(Fig. 6; stain, hematoxylin and
eosin). The diagnosis was confirmed by the histological analysis.
Following surgery, the chest pain was alleviated. At the time of
writing, the patient remained tumor-free.
Case 2
In February 2011, a 16 year-old female was admitted
to the Beijing Jishuitan Hospital. The patient presented with back
pain that had been apparent for six months. A slight curve towards
the left side of the patient’s back was observed. The patient
complained of pain at night that was reduced by taking aspirin. A
fixed tenderness point was identified in close proximity to the
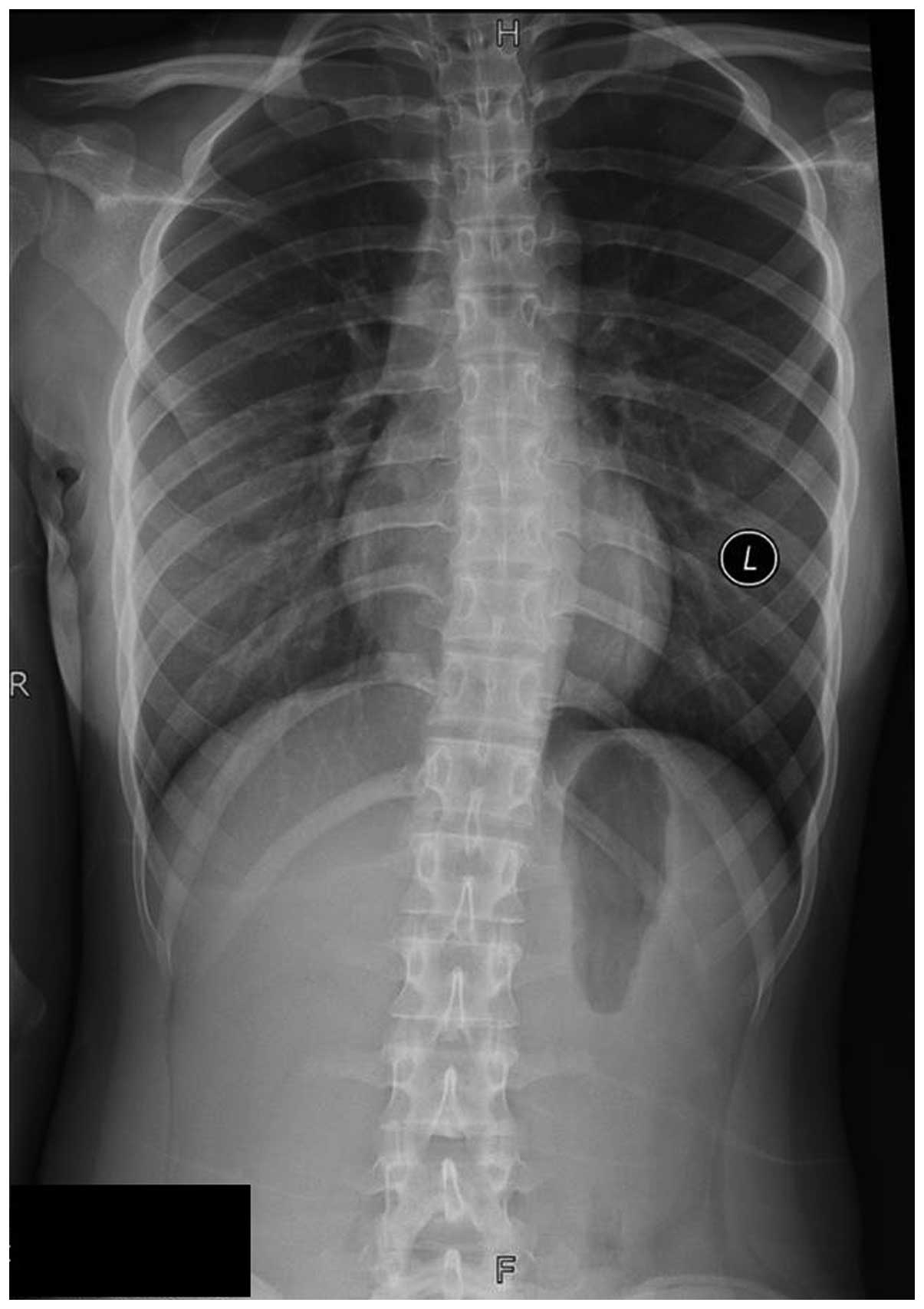
spine. A CT scan revealed a lesion that was located at the top of
the sixth right rib with calcification present in the center
(Fig. 7), while an X-ray scan
revealed scoliosis of the thoracic spine (Fig. 8). An intra-operative three
dimensional C-arm-based navigation system (REF 7700-500-000,
Stryker, Kalamazoo, MI, USA) was used to locate and completely
resect the tumor and curette the nidus (Fig. 9). The diagnosis was confirmed by
histological analysis, which revealed interconnected, ossified bone
trabeculae with abundant osteoblasts (Fig. 10; stain, hematoxylin and eosin,
Tianhe Lien Company, Beijing, China). At the time of writing, the
patient remained tumor-free.
Discussion
Tumors of the rib are uncommon, constituting only
5–10% of all bone neoplasms. Osteoid osteomas are benign
osteoblastic neoplasms, which are characterized by a
well-demarcated core with a typical size of <1 cm and by a
distinctive surrounding zone of reactive bone formation (2). An osteoid osteoma may occur anywhere
in the cortex or medulla of the skeleton. However, the lesions
usually affect the lower extremities. Although pain is the primary
symptom of initial and recurrent disease (5), cases of osteoid osteoma without
presence of pain have also been reported (6).
The most common types of tumors that affect the ribs
are metastases and myelomas. Primary tumors of the ribs are
uncommon. Therefore, the location of a tumor within the rib may
help establish a differential diagnosis (7). Cartilaginous tumors frequently occur
close to the costochondral junction, while rib sarcomas are more
likely to present with symptoms of pain (8).
In total, <1% of osteoid osteomas affect the ribs
(2). The defining symptom of
osteoid osteoma is pain during the night that responds to
nonsteroidal anti-inflammatory drugs and salicylates. The lesions
most commonly involve the posterior or posterolateral shaft of the
rib and, upon imaging, present with similar features to tumors
located elsewhere in the body. Imaging typically reveals a small
radiolucent lesion with a thick sclerotic margin of reactive bone.
Due its accuracy in detecting the nidus, CT is the preferred
imaging technique used for the assessment of osteoid osteomas
(9–11). When the osteoid osteoma occurs in
the posterior portion of the rib, it may lead to scoliosis
(7), as observed in case 2 of the
present study. In case 1, the tumor was located at the shaft of the
rib, away from the spine; therefore, scoliosis did not occur. Small
rib lesions may not be detected in the lung window of a chest X ray
image, whereas CT scanning provides an improved field of view.
The differential diagnosis of painful lesions
located close to the ribs should consider tumors of the bone.
Aneurysmal bone cysts of the posterior vertebral elements,
eosinophilic granulomas and osteoid osteomas are the most commonly
occurring lesions (12). Due to the
characteristic symptoms and the presence of the nidus in the CT
scan, a diagnosis of other potential painful rib tumors was ruled
out in the present study.
Complete surgical excision is the standard treatment
method for osteoid osteoma and is usually offered to patients
experiencing chronic and substantial pain that is not relieved by
conservative treatment. In circumstances where excision is
challenging, curettage is a good option. Removal of the nidus is
the main aim of the treatment (13). Recent techniques for treating cases
of osteoid osteoma involve the removal of the tumor by
radiofrequency (14). However, as
the lesions in the present study were located close to the pleura,
the use of radiofrequency was deemed unsafe. Therefore, surgical
excision and curettage were the selected treatment methods for
cases 1 and 2, respectively. The diagnoses were confirmed by
histological analysis.
In conclusion, osteoid osteoma of the rib is an
extremely rare condition. The typical clinical symptoms and
characteristic imaging features often allow for a clear diagnosis.
The method used for the treatment of osteoid osteoma depends on the
tumor location.
References
|
1
|
Jaffe HL: Osteoid osteoma. A benign
osteoblastic tumorcomposed of osteoid and atypical bone. Arch Surg.
31:709–728. 1935. View Article : Google Scholar
|
|
2
|
Unni KK: Osteoid osteoma. Dahlin’s bone
tumors: general aspects and data on 11,087 cases. 5th edition.
Lippincott-Raven; Philadelphia, PA: pp. 121–130. 1996
|
|
3
|
Yildiz Y, Bayrakci K, Altay M and Saglik
Y: Osteoid osteoma: the results of surgical treatment. Int Orthop.
25:119–122. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ghanem I, Collet LM, Kharrat K, et al:
Percutaneous radiofrequency coagulation of osteoid osteoma in
children and adolescents. J Pediatr Orthop B. 12:244–252.
2003.PubMed/NCBI
|
|
5
|
Atesok KI, Alman BA, Schemitsch EH, et al:
Osteoid osteoma and osteoblastoma. J Am Acad Orthop Surg.
19:678–689. 2011.PubMed/NCBI
|
|
6
|
McDermott MB, Kyriakos M and McEnery K:
Painless osteoid osteoma of the rib in an adult. A case report and
a review of the literature. Cancer. 77:1442–1449. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mehdian H, Summers B and Eisenstein S:
Painful scoliosis secondary to an osteoid osteoma of the rib. Clin
Orthop Relat Res. 273–276. 1988.PubMed/NCBI
|
|
8
|
Walsh GL, Davis BM, Swisher SG, et al: A
single-institutional, multidisciplinary approach to primary
sarcomas involving the chest wall requiring full-thickness
resections. J Thorac Cardiovasc Surg. 121:48–60. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kargar S, Arefanian S, Ghasemi A, et al:
Osteoid osteoma of the rib presenting as thoracic outlet syndrome.
Ann Thorac Surg. 96:2221–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Touraine S, Emerich L, Bisseret D, et al:
Is pain duration associated with morphologic changes of osteoid
osteomas at CT? Radiology. 271:795–804. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Veluvolu P, Winkler T, Sajjad SM, et al:
Osteoid osteoma involving body of right rib. Preoperative
localization and postoperative confirmation. Clin Nucl Med.
17:895–896. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hoeffel JC, Lascombes P, Delgoffe C, et
al: Osteoid osteoma of the rib: a case report. J Pediatr Surg.
28:738–740. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gasbarrini A, Cappuccio M, Bandiera S, et
al: Osteoid osteoma of the mobile spine: surgical outcomes in 81
patients. Spine (Phila Pa 1976). 36:2089–2093. 2011. View Article : Google Scholar
|
|
14
|
Rehnitz C, Sprengel SD, Lehner B, et al:
CT-guided radiofrequency ablation of osteoid osteoma and
osteoblastoma: clinical success and long-term follow up in 77
patients. Eur J Radiol. 81:3426–3434. 2012. View Article : Google Scholar : PubMed/NCBI
|