Introduction
Over the last two decades, inflammatory
myofibroblastic tumors (IMTs) have emerged from within the broad
category of inflammatory pseudotumors, with distinctive clinical,
pathological and molecular features (1). The etiology and pathogenesis of IMT
remains unclear, however, infection, surgery, autoimmunity and
chromosomal variation have all been hypothesized to contribute to
IMT development (2). IMT has been
hypothesized to represent an inflammatory reaction to viral
infection, including human herpes virus 8 and Epstein-Barr Virus,
however, it has also been considered as a type of autoimmune
disease (3). Recently, IgG4-related
disease has been associated with the pathogensis of IMT (4); however, the exact mechanism remains
unclear (5,6). At the molecular level, positive
immunohistochemical staining of ALK is observed in ~40–100% of IMT
cases, depending on the anatomical sites at which they arise
(2,7).
Clinically, the majority of IMTs are benign, but they require
adequate surgical treatment, as they have a tendency for local
recurrence (8). IMTs exhibit a
predilection for children and adolescents are are considered to
metastasize in ≤5% of cases (2). The
most common anatomical locations are the abdominopelvic region, the
lungs and the retroperitoneum (9),
however, it rarely occurs in the limbs (10). Previously described cases of IMT have
been described in the somatic soft tissue and bone (10). We present a case of an IMT in the hand
of an adult. Written informed consent was obtained from the
patient.
Case report
In November 2009, a 58-year-old male presented to
the Department of Hand Surgery at The First Affiliated Hospital of
Zhejiang University (Hangzhou, China) with right dorsal hand ulcers
that had been recurring for more than one year. The patient had
previously undergone debridement and drainage without biopsy three
times. Local clinics had diagnosed the condition as cellulitis
(infection of the tissues below the skin), and found that the ulcer
in the dorsal hand was refractory, with a trend for spreading. A
physical examination showed a red and swollen hand and fingers,
several ulcerous wounds with previous incision scars and bone
exposure in the proximal phalanx of the index finger. The flexion
and extension of the metacarpophalangeal joint was limited. X-ray
showed no destruction of the bones and joints. Metal foreign matter
was also found in the hand, which was caused by an injury 10 years
ago (Fig. 1). Thus, the magnetic
resonance imaging (MRI) scan was canceled. The laboratory findings
were normal, except for normocytic, normochromic anemia. A fungal
culture of the wound revealed the presence of Candida
albicans.
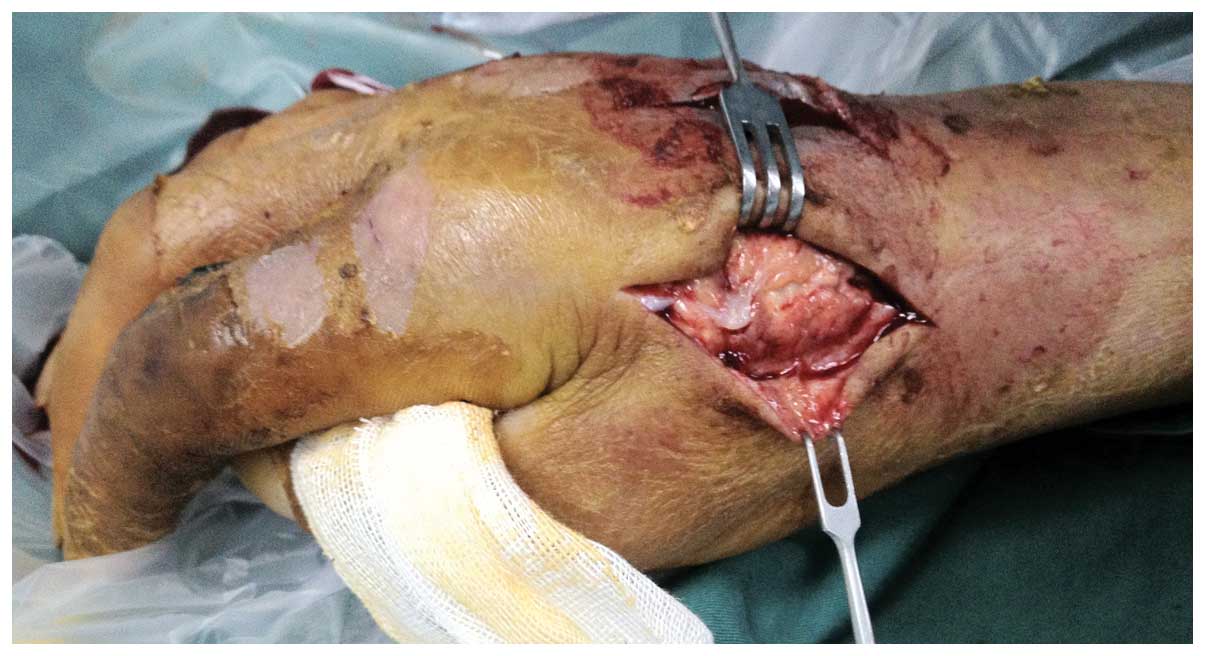
Following one week of antifungal treatment
(nystatin; 500,000 units every 6 h; YunPeng Inc., Linfen, China),
debridement was performed under general anesthesia. A tumor with
granulation of the vascularization in the subcutaneous tissue,
which bled easily, was found. The dorsal extensor tendons, dorsal
vein and cutaneous nerve were involved. The diffuse tumor grew
within the superficial layer of the dorsal interosseous. No tumor
capsule was noted. The involved tissue was removed with the tumor,
except for the tendons and cutaneous nerve. The involved tendon
sheath and epineurium were carefully resected (Fig. 2).
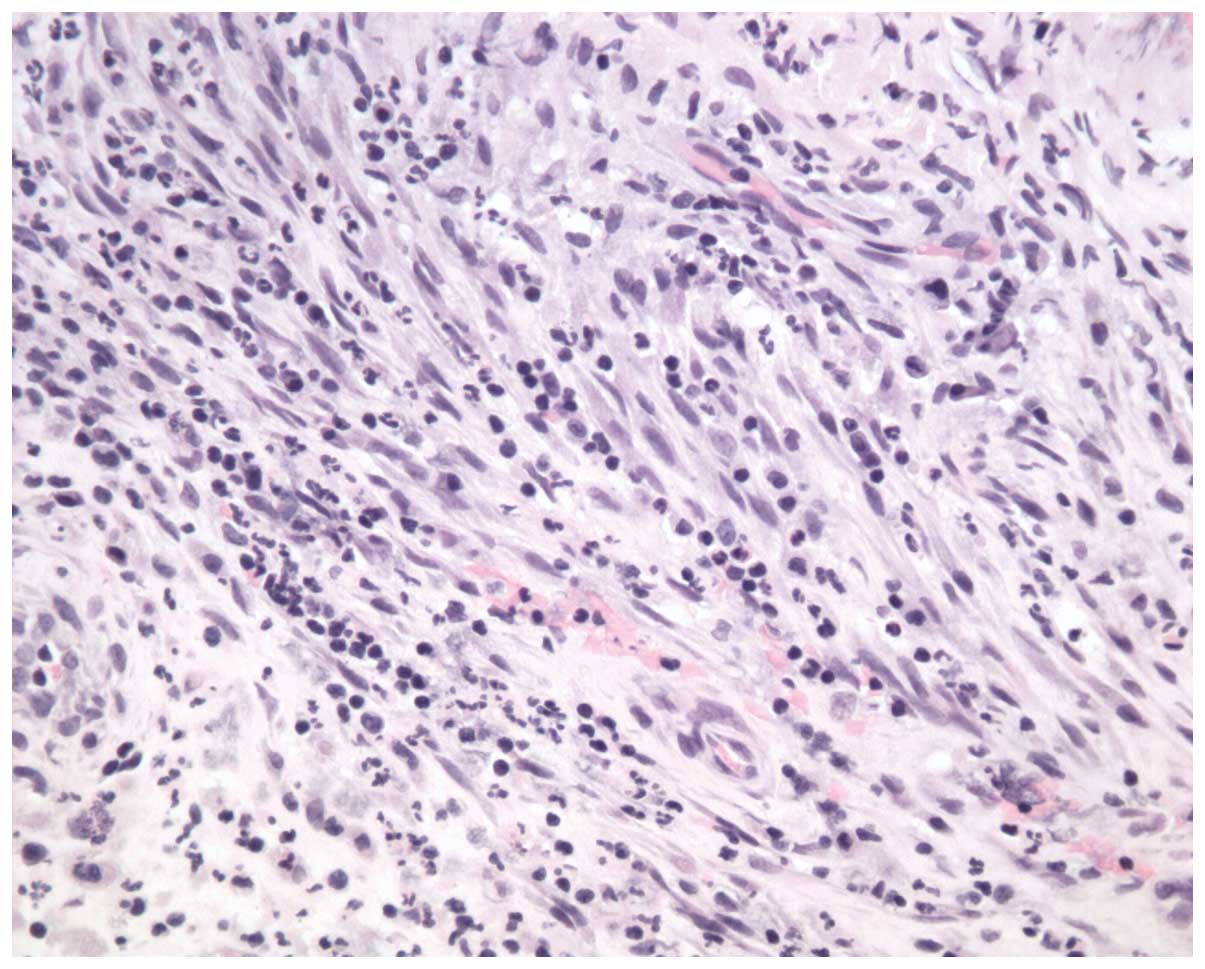
The intraoperative frozen section revealed that the
tissue showed degeneration, necrosis and inflammatory granulation,
with atypical hyperplasia. An extended resection of the granulation
tissue and inflammatory veins was performed. Relaxation incisions
were designed in the dorsal hand to close the incisions.
Histologically, the tumor was composed of spindle cells in a
mesenchymal arrangement, with evident cellularity and necrosis,
accompanied by mononuclear cell infiltration consisting of dense
lymphocytes and plasma cells (Fig.
3). Immunohistochemical stains were positive for smooth muscle
actin and desmin and negative for CD34, S100 and CD117. In
addition, the spindle cells were not reactive with antibodies
specific for cyclin D1, p53, B-cell lymphoma-2 or anaplastic
lymphoma kinase. An IMT was consequently diagnosed.
Following one week of negative pressure draining,
the relaxation incisions were closed. The patient underwent an
uneventful post-operative course and was discharged. No signs of
recurrence were detected on follow-up at 24 months.
Discussion
IMTs are histologically characterized by dominant
myofibroblast invasion and variable inflammatory infiltrates. The
tumors behave as benign lesions, but occasionally can be locally
aggressive. The literature to date shows that IMTs most typically
occur in the lungs and retroperitoneum. Little focus has been
placed on the localization of IMTs in the limbs and extremities
(10). Currently, the etiology of IMT
is unclear, however, an inflammatory origin has been suggested due
to an association with minor trauma, surgery and/or infections
(6,10). The causes of IMT in the present case
arose from infection and debridement. Debridement without biopsy is
the main cause of the misdiagnosis of IMTs. Using MRI, it is
possible to evaluate the lesional extension of IMTs in the soft
tissues, although this was not feasible in the present case due to
the presence of metal foreign matter in the patient's hand, which
was caused by an injury 10 years ago.
IMTs in the soft tissues have seldom been reported
in the literature. The tumors usually displace and distort the soft
tissues or bones (10). Meanwhile,
IMTs in the hand have not yet been reported at all. In the present
case, the tumor was found to be locally invasive. In the confined
space of the dorsal hand, the dorsal extensor tendons and cutaneous
nerve were involved. Thus, an enlarged resection would have
destroyed the functional structure in the hand. The treatment of
such IMTs can be challenging, as there is no established medical
treatment protocol, and the proximity of the tumors to vital
structures tumors can mean that they are not resectable. The
decision to treat this lesion only by tumor resection with
preservation of the extensor tendons, dorsal vein and cutaneous
nerve turned out to be appropriate. A reconstructive approach after
an enlarged resection would have been invasive with a less
functional result, however, it may have reduced the risk of local
recurrence, which is ~25% for IMTs (5).
IMTs in the hands are relatively rare and are often
easily misdiagnosed as infection. An early and correct diagnosis is
the key to successful treatment. A biopsy is necessary following
debridement of infection lesions, particularly recurrent infected
lesions. The surgical approach is should be conservative, in order
to maintain maximum hand function.
References
|
1
|
Gleason BC and Hornick JL: Inflammatory
myofibroblastic tumours: where are we now? J Clin Pathol.
61:428–437. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cantera JE, Alfaro MP, Rafart DC, et al:
Inflammatory myofibroblastic tumours: a pictorial review. Insights
Imaging. 6:85–96. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lui PC, Fan YS, Wong SS, et al:
Inflammatory pseudotumors of the central nervous system. Hum
Pathol. 40:1611–1617. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rafeek N, Joseph LD, Rajendiran S and
Narayanan CD: Inflammatory myofibroblastic tumor of spermatic cord.
Int J Surg Case Rep. 3:618–621. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathologic and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen WC, Jiang ZY, Zhou F, et al: A large
inflammatory myofibroblastic tumor involving both stomach and
spleen: A case report and review of the literature. Oncol Lett.
9:811–815. 2015.PubMed/NCBI
|
|
7
|
Cook JR, Dehner LP, Collins MH, et al:
Anaplastic lymphoma kinase (ALK) expression in the inflammatory
myofibroblastic tumor: a comparative immunohistochemical study. Am
J Surg Pathol. 25:1364–1371. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Katakwar A, Gedam BS, Mukewar S and Agasti
A: Primary gastric inflammatory myofibroblastic tumor in an
adult-case report with brief review. Indian J Surg Oncol. 5:66–70.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathological and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Masciocchi C, Lanni G, Conti L, et al:
Soft-tissue inflammatory myofibroblastic tumors (IMTs) of the
limbs: potential and limits of diagnostic imaging. Skeletal Radiol.
41:643–649. 2012. View Article : Google Scholar : PubMed/NCBI
|