Introduction
Prostate cancer is one of the most common
malignancies of the urinary tract. Based on incidence and mortality
data from several agencies, the American Cancer Society estimates
that 233,000 new prostate cancer cases and 29,480 mortalities from
prostate cancer are projected to occur in the United States in 2014
(1). Prostate cancer is a
heterogeneous disease that varies in spectrum from tumors with a
low risk of mortality to highly aggressive malignant disease
(2). Newly diagnosed prostate cancer
has been increasing in Japan, and is predicted to be the first or
second most common cancer by 2020 (3). Although the age-adjusted mortality rate,
which had rapidly increased up to ~2,000, began to reduce slightly
in 2004, the crude mortality rate has continued to rise gradually
due to the ageing population (4).
Radical prostatectomy has commonly been performed using an open
retropubic approach for localized prostate cancer. However, in the
past decade, with the development of laparoscopic and robotic
techniques, laparoscopic radical prostatectomy (LRP) or
robotic-assisted LRP (RALRP) has been widely accepted with the
advantages of less invasiveness, shorter recovery, reduced blood
loss, and improved visualization of the operative region compared
to open techniques (5–7) Severe hemorrhage following prostatectomy
is relatively rare, but is one of the serious complications. The
current study presents a case in which arteriography with
transarterial embolization (TAE) was beneficial for the treatment
of severe hemorrhage following LRP.
Case report
In May 2013, a 70-year-old man first presented with
lower urinary tract symptoms to the outpatient clinic of Kurume
University Hospital, Fukuoka, Japan and was demonstrated to have an
elevated the prostate-specific antigen (PSA) of 9.3 ng/ml. In
September 2013, subsequent transrectal ultrasound-guided biopsy of
the prostate showed prostate adenocarcinoma, with Gleason Score
3+4=7 involving 30% of the bilateral lobes. According to the
imaging and biopsy findings, the tumor was classified as cT2cN0M0.
In December 2013, LRP and pelvic lymphadectomy were performed
without nerve sparing bilaterally. Vesico-urethral anastomosis with
continuous suture was conducted using 3-0 absorbable monofilament
suture. The surgical duration was 183 min and the blood loss during
the procedure was 580 g. Early post-operative recovery was
uneventful. Cystography showed no urinary leakage and the Foley
catheter was removed on post-operative day 3.
On post-operative day 9, the patient complained of
lower abdominal pain. The hemoglobin (Hb) level decreased from 11.4
to 7.3 g/dl (normal range, 13.5–17.5 g/dl) and the hematocrit (Ht)
level decreased from 33.5 to 21.8% (normal range, 39.7–52.4%). Four
units of blood were transfused and emergent computed tomography
angiography (CTA) showed a large pelvic hematoma, with
extravasation of the contrast agent in the hematoma, suggesting
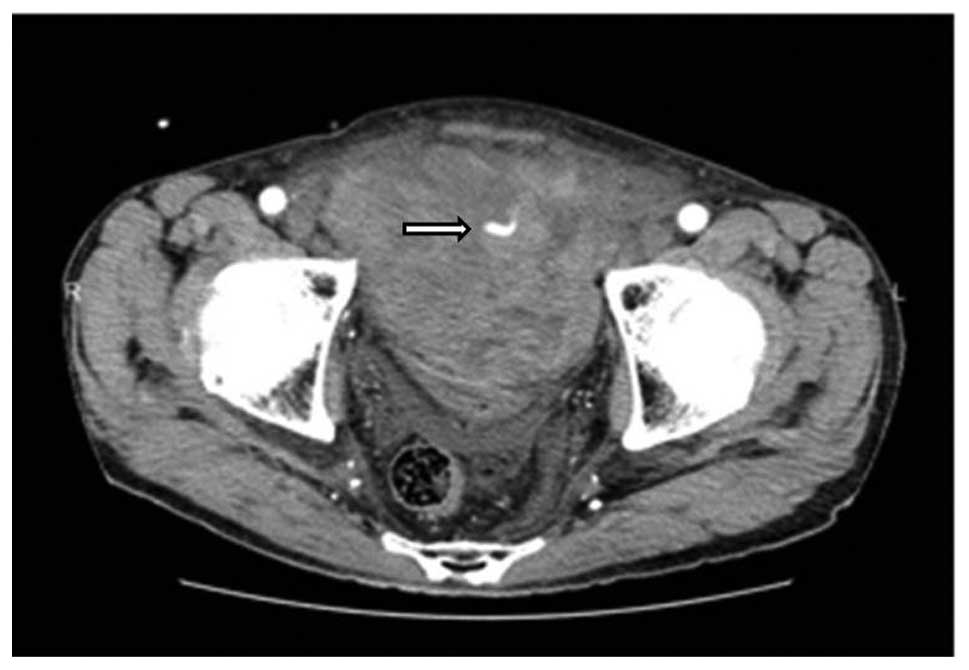
arterial bleeding. Digital subtraction angiography (DSA), performed
via a transfemoral approach with selective catheterization of the
two internal iliac arteries (Fig. 1),
revealed active bleeding from a branch of the right obturator
artery. We speculate that this branch may have been injured during
pelvic lymphadectomy (PLND). Super selective catheterization of the
bleeding vessel was performed using a microcatheter (2.2 Fr/2.8 Fr)
with a hydrophilic 0.016-inch guidewire. Embolization was performed
successfully using a platinum coil (2×10 mm).
However, the Hb level remained at 7.0 to 8.0 g/dl
and follow-up CT revealed that the pelvic hematoma had increased in
size. On post-operative day 16, a second DSA procedure was
performed, but no arterial bleeding was revealed. Following the
second DSA procedure, the Hb and Ht levels improved and the patient
was discharged on post-operative day 36. At 3 months post-surgery,
the pelvic hematoma was shown to have been absorbed on computed
tomography scans. The patient is currently mildly incontinent, with
a PSA level of 0.03 ng/ml.
Discussion
LRP was first described by Schuessler et al
(8) and Raboy et al (9) in 1997. The surgical procedure was
established in 1999 by Guillonneau et al (10). A large body of literature has shown
that LRP and RALRP are an effective option and the standard
surgical treatment for localized prostate cancer, as these
approaches are minimally invasive compared with open radical
prostatectomy (ORP) and achieve a level of cancer control
equivalent to that following ORP (5–7,10–13).
Severe post-operative hemorrhage following radical prostatectomy
has been reported in 0.5 to 1.6% of cases, according to a range of
definitions (14,15). A meta-analysis of the incidence of
complications showed that pelvic hematoma was significantly less
frequent following RALRP compared with ORP. In addition, the study
showed that there is no significant difference in the frequency
between LRP and ORP (16).
Severe hemorrhage following radical prostatectomy
was first described by Foss in 1923 (17). The incidence rates of intraoperative
and post-operative hemorrhage have decreased since Reiner and Walsh
(18) described the anatomy of the
dorsal venous complex and a method for early hemorrhage control
during radical prostatectomy. Hemorrhage following radical
prostatectomy is mainly of venous origin. Arterial hemorrhage is
uncommon. Compression of the retropubic space with tissue-to-tissue
contact leads to rapid resolution in cases of venous hemorrhage. By
contrast, surgical intervention is recommended for arterial
hemorrhage. In a retrospective study of 7 cases with serious
hemorrhage among 1,350 cases treated with ORP, Hedican and Walsh
(14) suggested that evacuation of
the pelvic hematoma decreased the likelihood of bladder neck
contracture and incontinence. In an examination of post-operative
and quality of life outcomes in patients with major hemorrhage
following ORP that was managed by reoperation or observation,
Kaufman and Lepor (15) reported that
reoperation facilitated the healing of the vesico-urethral
anastomosis and removal of the urinary catheter.
TAE has become an increasingly common treatment for
life-threatening hemorrhage from various bleeding sites. TAE has
the advantages of a rapid recovery, short hospital stay and early
resumption of physical activities compared with surgical
intervention (19). To the best of
our knowledge, 12 patients, including the present case, have been
reported thus far with post-operative hemorrhage treated by TAE
(Table I) (20–26). In
this previously reported literature, 3 patients underwent ORP, 4
underwent RALRP and 5 underwent LRP. Almost all cases, with the
exception of the present case, underwent bilateral or unilateral
nerve sparing. CTA revealed active bleeding in all cases, and
extravasation in CTA was important for discriminating between
venous and arterial hemorrhage. The bleeding focus was frequently
the internal pudendal or accessory pudendal artery. However, in the
present case, the bleeding focus was a branch of the obturator
artery which may have been injured during PLND. Bratt et al
(27) recorded 4 cases of
post-operative pelvic hematoma among 156 patients treated with PLND
following radical prostatectomy. TAE for hemorrhage from the
obturator artery following laparoscopic prostatectomy has not been
described previously.
 | Table I.Literature review of transarterial
embolization for hemorrhage following ORP, LRP or RALRP. |
Table I.
Literature review of transarterial
embolization for hemorrhage following ORP, LRP or RALRP.
| First author, year
(ref.) | Age, years | GS | T stage | Surgical method | Nerve sparing | Ht prior to TAE,
% | Blood transfusion,
units | Bleeding focus | Material |
|---|
| Ibarra et al,
2003 (20) | 70 | 4+3 | 2a | ORP | Unilateral or
bilataral | 20.7 | 4 | A branch of the lt
internal iliac artery to seminal vesicle | Microcoil |
| Beckley et al,
2007 (21) | 56 | 3+3 | 1c | RALRP | Unknown | Unknown | 2 | Lt accessory pudendal
artery | Microcoil
Gelfoam |
| Park et al,
2008 (22) | 54 | 3+3 | 1c | LRP | Unknown | 20.4 | 5 | A branch of the lt
internal iliac artery (a capsular artery) | NBCA |
| Lopes et al,
2009 (23) | 55 | 3+4 | 2c | LRP | Bilateral | Unknown | Unknown | Lt internal pudendal
artery | NBCA |
|
| 57 | 3+3 | 2c | LRP | Bilateral | Unknown | Unknown | Rt internal pudendal
artery | Microcoil |
| Jeong et al,
2010 (24) | 54 | 3+3 | 3a | LRP | Bilateral | 26.9 | 5 | A branch of the lt
internal iliac artery | NBCA |
|
| 69 | 3+4 | 3a | RALRP | Unilateral | 27.5 | 7 | A branch of the lt
internal iliac artery | NBCA |
|
| 69 | 4+3 | 2a | RALRP | Bilateral | 27.2 | 10 | A distal branch of
the rt internal pudendal artery | NBCA |
|
| 73 | 3+3 | 2a | ORP | Bilateral | 23.4 | 9 | A branch of the lt
internal iliac artery | NBCA |
| Cheng et al,
2012 (25) | 63 | 3+3 | Unknown | ORP | Unknown | 17.6 | 4 | Branches of the bil
internal iliac artery | Microcoil |
| Feng et al,
2013 (26) | 55 | 3+4 | Unknown | RALRP | Bilateral | Unknown | Unknown | Lt accessory pudendal
artery | Unknown |
| Present case | 70 | 3+4 | 2c | LRP | None | 21.8 | 4 | A branch of the rt
obturator artery | Microcoil |
Materials for use in embolization include coils,
polyvinyl alcohol particles, gelatin sponge (Gelfoam), and
N-butyl-cyanoacrylate (NBCA) (28). The major advantages of microcoils are
the absence of movement to a peripheral blood vessel and a lower
risk of recanalization compared with other materials. However, the
small diameters of distal branches usually do not allow the use of
microcoils. Collateralization is a further possible disadvantage of
microcoil embolization and may lead to the persistent flow of blood
into the vascular region of the embolized vessel, thus decreasing
the therapeutic efficacy (29).
Gelfoam has commonly been used for hemorrhage from small branches
in cases in which microcoils could not be used or were unavailable,
but the temporary nature of Gelfoam leaves a risk of
recanalization. NBCA has been used most commonly in previous
studies (24,26). NBCA is administered in liquid form
prior to polymerization, and is generally mixed with iodized oil to
minimize the exothermic reaction of NBCA, which delays and controls
the polymerization time. This feature is beneficial in the
occlusion of small vessels (29).
With regard to post-operative urinary incontinence,
6 cases from the literature regained excellent urinary continence
within a 6-month follow-up period, while only 2 patients
experienced mild incontinence. These continence results are not
inferior to those of previous studies of surgical intervention. In
the present case, the patient experienced a certain degree of
stress urinary continence at the 3-month follow-up, but it is
likely that the incontinence will improve with time.
In summary, the current study presented a case in
which TAE was performed for pelvic hematoma following LRP. Arterial
hemorrhage following prostatectomy is relatively rare, but is one
of the serious complications. It may be concluded that TAE for
arterial hemorrhage following radical prostatectomy is a safe and
minimally invasive treatment compared with surgical intervention.
Moreover, it may be advantageous with regard to urinary
incontinence.
References
|
1
|
Siegel R, Ma J, Zou Z and Jemal A: Cancer
statistics, 2014. CA Cancer J Clin. 64:9–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Teloken C, Da Ros CT, Caraver F, Weber FA,
Cavalheiro AP and Graziottin TM: Low serum testosterone levels are
associated with positive surgical margins in radical retropubic
prostatectomy: Hypogonadism represents bad prognosis in prostate
cancer. J Urol. 174:2178–2180. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Katanoda K, Hori M, Matsuda T, Shibata A,
Nishino Y, Hattori M, Soda M, Iokax A, Sobue T and Nishimoto H: An
updated report on the trends in cancer incidence and mortality in
Japan, 1958–2013. Jpn J Clin Oncol. 45:390–401. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Onozawa M, Hinotsu S, Tsukamoto T, Oya M,
Ogawa O, Kitamura T, Suzuki K, Naito S, Namiki M, Nishimura K,
Hirao Y and Akaza H: Recent trends in the initial therapy for newly
diagnosed prostate cancer in Japan. Jpn J Clin Oncol. 44:969–981.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tooher R, Swindle P, Woo H, Miller J and
Maddern G: Laparoscopic radical prostatectomy for localized
prostate cancer: A systematic review of comparative studies. J
Urol. 175:2011–2017. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ferronha F, Barros F, Santos VV, Ravery V
and Delmas V: Is there any evidence of superiority between
retropubic, laparoscopic or robot-assisted radical prostatectomy?
Int Braz J Urol. 37:146–158. 2011.PubMed/NCBI
|
|
7
|
Akand M, Celik O, Avci E, Duman I and
Erdogru T: Open, laparoscopic and robot-assisted laparoscopic
radical prostatectomy: Comparative analysis of operative and
pathologic outcomes for three techniques with a single surgeon's
experience. Eur Rev Med Pharmacol Sci. 19:525–531. 2015.PubMed/NCBI
|
|
8
|
Schuessler WW, Schulam PG, Clayman RV and
Kavoussi LR: Laparoscopic radical prostatectomy: I nitial
short-term experience. Urology. 50:854–857. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Raboy A, Ferzli G and Albert P: Initial
experience with extraperitoneal endoscopic radical retropubic
prostatectomy. Urology. 50:849–853. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guillonneau B, Cathelineau X, Barret E,
Rozet F and Vallancien G: Laparoscopic radical prostatectomy:
Technical and early oncological assessment of 40 operations. Eur
Urol. 36:14–20. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Greco F, Wagner S, Hoda MR, Kawan F,
Inferrera A, Lupo A, Reichelt O, Jurczok A, Hamza A and Fornara P:
Laparoscopic vs open retropubic intrafascial nerve-sparing radical
prostatectomy: surgical and functional outcomes in 300 patients.
BJU Int. 106:543–547. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Drouin SJ, Vaessen C, Hupertan V, Comperat
E, Misraï V, Haertig A, Bitker MO, Chartier-Kastler E, Richard F
and Rouprêt M: Comparison of mid-term carcinologic control obtained
after open, laparoscopic and robot-assisted radical prostatectomy
for localized prostate cancer. World J Urol. 27:599–605. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Moran PS, O'Neill M, Teljeur C, Flattery
M, Murphy LA, Smyth G and Ryan M: Robot-assisted radical
prostatectomy compared with open and laparoscopic approaches: A
systematic review and meta-analysis. Int J Urol. 20:312–321. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hedican SP and Walsh PC: Postoperative
bleeding following radical retropubic prostatectomy. J Urol.
152:1181–1183. 1994.PubMed/NCBI
|
|
15
|
Kaufman JD and Lepor H: Reoperation versus
observation in men with major bleeding after radical retropubic
prostatectomy. Urology. 66:561–565. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tewari A, Sooriakumaran P, Bloch DA,
Seshadri-Kreaden U, Hebert AE and Wiklund P: Positive surgical
margin and perioperative complication rates of primary surgical
treatments for prostate cancer: A systematic review and
meta-analysis comparing retropubic, laparoscopic and robotic
prostatectomy. Eur Urol. 62:1–15. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Foss HL: The control of hemorrhage
following prostatectomy. Ann Surg. 78:802–805. 1923. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Reiner WG and Walsh PC: An anatomical
approach to the surgical management of the dorsal vein and
Santorini's plexus during radical retropubic surgery. J Urol.
121:198–200. 1979.PubMed/NCBI
|
|
19
|
Beaujeux R, Saussine C, al-Fakir A,
Boudjema K, Roy C, Jacqmin D and Bourjat P: Superselective
endo-vascular treatment of renal vascular lesions. J Urol.
153:14–17. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ibarra R, Magee C, Ferral H and Thompson
IM: Post-prostatectomy bleeding managed by endovascular
embolization. J Urol. 169:276–277. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Beckley I, Patterson B, Hamaday M, Vale J
and Hrouda D: Case report: Delayed hemorrhage from an accessory
internal pudendal artery pseudoaneurysm after robotic radical
prostatectomy: Successful management with ct angiography and
embolization. J Endourol. 21:923–925. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Park YH, Lee JH and Kim HH: Severe
bleeding after laparoscopic radical prostatectomy: Successful
management with transarterial embolization. J Endourol.
22:2687–2689. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lopes RI, Mitre AI, Rocha FT, Piovesan AC,
da Costa OF and Karakhanian W: Case report: Late recurrent
hematuria following laparoscopic radical prostatectomy may predict
internal pudendal artery pseudoaneurysm and arteriovenous fistula.
J Endourol. 23:297–299. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jeong CW, Park YH, Ku JH, Kwak C and Kim
HH: Minimally invasive management of postoperative bleeding after
radical prostatectomy: Tvransarterial embolization. J Endourol.
24:1529–1533. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cheng S, Xu L, Li G, Chen Y, Hu H, Zhang Z
and Ding G: Superselective internal iliac arterial embolization for
severe hemorrhage following radical prostatectomy. Oncol Lett.
4:521–523. 2012.PubMed/NCBI
|
|
26
|
Feng T, Patel HD and Allaf ME: Pudendal
artery pseudoaneurysm after robot-assisted laparoscopic radical
prostatectomy. Urology. 81:e5–e6. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bratt O, Elfving P, Flodgren P and
Lundgren R: Morbidity of pelvic lymphadenectomy, radical retropubic
prostatectomy and external radiotherapy in patients with localised
prostatic cancer. Scand J Urol Nephrol. 28:265–271. 1994.PubMed/NCBI
|
|
28
|
Fratezi AC, Martins VM, Pereira Porta RM,
Prado MA, Prota R, Caldas JG and Cerri G: Endovascular therapy for
priapism secondary to perineal trauma. J Trauma. 50:581–584. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang MQ, Duan F, Liu FY, Wang ZJ and Song
P: Treatment of symptomatic polycystic liver disease: Transcatheter
super-selective hepatic arterial embolization using a mixture of
NBCA and iodized oil. Abdom Imaging. 38:465–473. 2013. View Article : Google Scholar : PubMed/NCBI
|