Introduction
Benign nodular goiter is a common disease affecting
5% of the general population in non-endemic and 15% in endemic
areas (1). The natural history of
non-endemic benign goiters is characterized by a gradual increase
in goiter size, with simultaneous development of increasing thyroid
nodularity and thyroid autonomy (2).
There are four main treatment options for these diseases:
monitoring without treatment, surgery, levothyroxine suppression
and radioactive iodine-131 (3). Large
goiters with obstructive symptoms including shortness of breath and
dyspnea are a clear indication for surgery (4); however, acute upper airway obstruction,
particularly in benign cervical goiter cases, is rare (5–9).
We herein report a rare case with acute upper airway
obstruction due to a benign cervical nodular goiter.
Case report
A 46-year-old female was referred to Iida Municipal
Hospital, Nagano, Japan, for treatment of a large goiter in
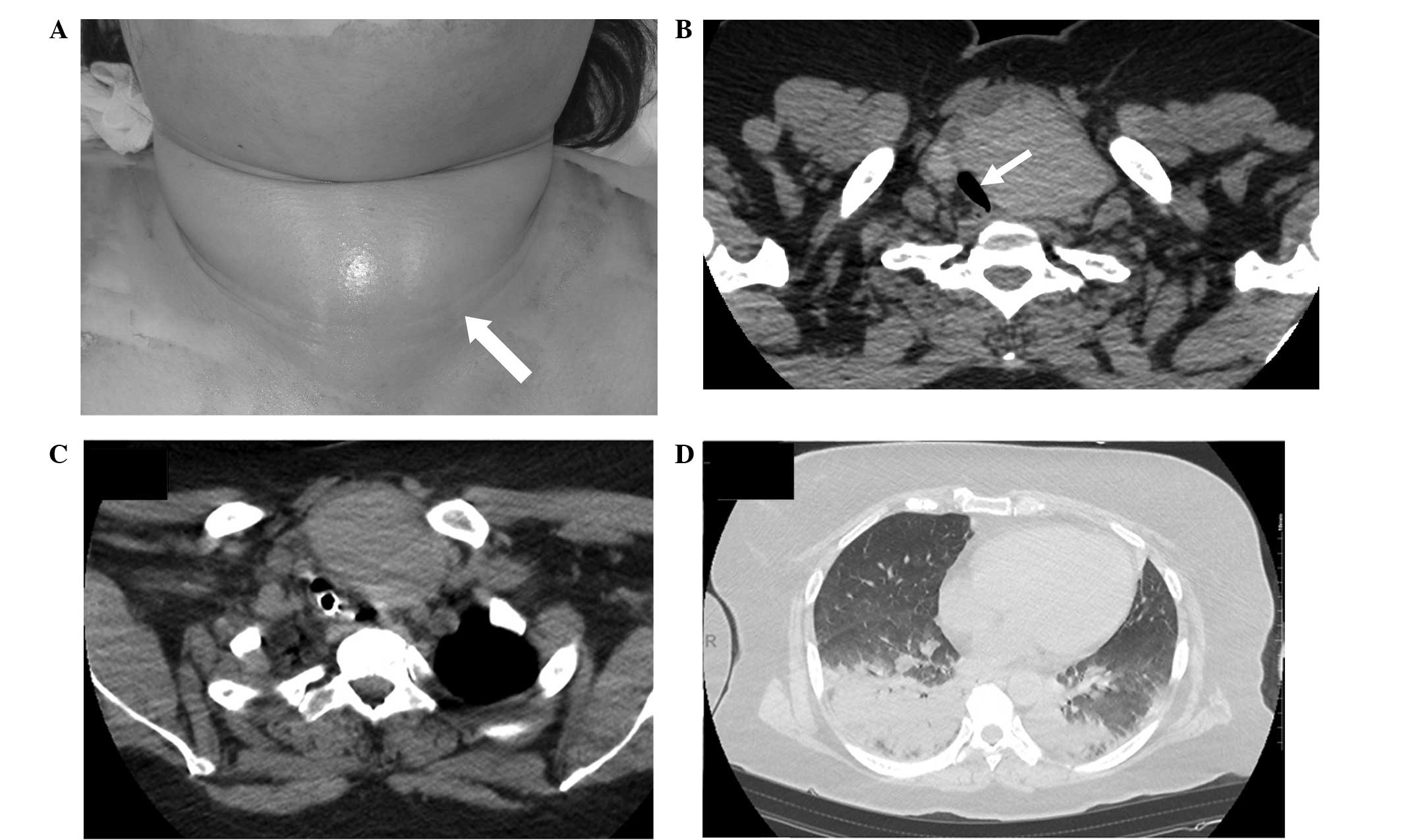
December 2011. The patient had few complaints on presentation, but
occasionally experienced difficulty breathing. She had a large,
elastic and non-tender goiter which was more pronounced on the left
side of her neck (Fig. 1A).
Laboratory studies revealed a euthyroid state; antithyroglobulin
and thyroid peroxidase antibodies were both negative. A computed
tomography (CT) scan of the neck and thorax revealed gross
enlargement of the left lobe of the thyroid, measuring 75×51 mm,
with a clear border and a relatively homogeneous structure, which
was mostly located in the cervical region (Fig. 1B). The trachea was narrowed and
shifted to the right side by the nodular goiter. Fine needle
aspiration biopsy revealed the nodule to be benign. The diagnosis
of a benign nodular goiter was confirmed and surgery was scheduled
for within a few months.
Three months later, the patient was brought to our
emergency room by ambulance due to loss of consciousness with
breathing difficulty and was immediately intubated for mechanical
ventilation. The patient's height was 160 cm and she weighed 90 kg.
Carbon dioxide narcosis was indicated by arterial blood gas
analysis: pH 6.76; pCO2, 106.5 mmHg; pO2, 46.3 mmHg. The CT scan
revealed that the trachea was markedly compressed (the diameter of
the narrowest portion of the lumen was 4 mm) by the nodular lesion
in the left lobe of the thyroid, and bilateral pneumonia was also
evident (Fig. 1C and D). However, the
size of the nodule itself was unchanged compared with that observed
at the first visit. Total thyroidectomy was immediately performed
via a supraclavicular approach without median sternotomy. We were
able to fully palpate the nodule from the supraclavicular region to
identify a well-encapsulated mass with a smooth surface. Following
removal of the thyroid, the trachea returned to the center of the
neck and was normal with no features of tracheomalacia. The patient
had an uneventful postoperative course and recovered well.
The resected specimen included a well-encapsulated
solid mass measuring 45 mm in size. Part of the specimen was a
monocular cyst. Histopathological examination mainly revealed an
adenomatous goiter but there was a micro-papillary carcinoma in
part of the goiter. The patient provided informed consent for
publication of the present study.
Discussion
Acute airway obstruction due to retrosternal benign
goiters or thyroid malignancies has been widely described, however,
benign cervical goiters causing acute airway obstruction are rare
(9). Deaths from such goiters due to,
for example, suffocation by airway obstruction, should be
prevented, considering that these are benign diseases which
generally have a low mortality rate.
With respect to the risk factors for acute airway
obstruction, studies have suggested that acute obstruction is due
to sudden hemorrhage into a cyst, an upper respiratory tract
infection causing edema, tracheal collapse or worsening of
comorbidities (5,8,10,11). Since the patient in our case was
asymptomatic, it was decided not to operate immediately. It was not
anticipated that such a nodular enlargement of the thyroid would
cause sudden upper airway obstruction. There was no histological
evidence of hemorrhage into the thyroid gland. The acute
exacerbation could, however, have been due to upper airway
infection or smoking, resulting in edema and retention of
secretions, since the patient later caught a cold and, moreover,
was a heavy smoker. Kadhim et al (12) reported that chronic obstructive airway
disease, substernal extension and long-standing goiter were
considered to be risk factors for developing acute,
life-threatening airway compromise in the presence of benign
thyroid disease. In addition, these authors advocated that
following emergency thyroidectomy, close observation was mandatory
to exclude airway compromise due to tracheomalacia and laryngeal
edema. Nakadate et al (13)
reported that the risk factors for tracheomalacia following
thyroidectomy were as follows: goiter for more than 5 years,
preoperative recurrent laryngeal nerve palsy, significant tracheal
narrowing and/or deviation, retrosternal extension, difficulty with
endotracheal intubation, reoperation and retrotracheal extension of
a thyroid nodule. Fortunately, the present case did not have
tracheomalacia, although the patient was carefully monitored for
this condition following thyroidectomy in our intensive care
unit.
Thus, it appears that the risk factors for acute
benign cervical goiter causing acute airway obstruction are edema
of the tracheal mucosa, secretion retention and bleeding. Edema of
the tracheal mucosa is often caused by acute airway infection.
Secretion retention is also caused by infection and certain other
events, including chronic obstructive airway disease and smoking.
Rapid enlargement of a nodular goiter due to bleeding from the
cystic wall occasionally causes acute airway obstruction.
In conclusion, it should be kept in mind that benign
asymptomatic nodular goiter mostly located in the neck may cause
acute airway obstruction, even if the nodules are not particularly
large. Nodular goiters causing tracheal deviation and stenosis,
visible on CT scans, necessitate that surgery be scheduled as soon
as possible. If surgical treatment is delayed for any reason,
patients should be strictly followed up until surgery, with
attention paid to the above-mentioned risk factors.
References
|
1
|
Abraham D, Singh N, Lang B, et al: Benign
nodular goitre presenting as acute airway obstruction. ANZ J Surg.
77:364–367. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Berghout A, Wiersinga WM, Smits NJ, et al:
Interrelationships between age, thyroid volume, thyroid nodularity
and thyroid function in patients with sporadic nontoxic goiter. Am
J Med. 89:602–608. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Samuels MH: Evaluation and treatment of
sporadic nontoxic goiter - some answers and more questions. J Clin
Endocrinol Metab. 86:994–997. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Clark OH, Duh QY and Kebebew E: Textbook
of Endocrine Surgery. 2nd. Saunders Elsevier; Philadelphia: 2005,
View Article : Google Scholar
|
|
5
|
Sajja LR, Mannam GC, Sompalli S, et al:
Multinodular goiter compressing the trachea following open heart
surgery. Asian Cardiovasc Thorac Ann. 14:416–417. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tseng KH, Felicetta JV, Rydstedt LL, et
al: Acute airway obstruction due to a benign cervical goiter.
Otolaryngol Head Neck Surg. 97:72–75. 1987.PubMed/NCBI
|
|
7
|
Shaha AR: Surgery for benign thyroid
disease causing trachea-oesophageal compression. Otolaryngol Clin
North Am. 23:391–401. 1990.PubMed/NCBI
|
|
8
|
Melliere D, Saada F, Etienne G, et al:
Goiter with severe respiratory compromise: evaluation and
treatment. Surgery. 103:367–373. 1988.PubMed/NCBI
|
|
9
|
Sharma A, Naraynsingh V and Teelucksingh
S: Benign cervical multi-nodular goiter presenting with acute
airway obstruction: a case report. J Med Case Rep. 4:2582010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rios A, Rodriguez JM, Galindo PJ, et al:
Spirometric evaluation of respiratory involvement in asymptomatic
multinodular goiter with an intrathoracic component. Arch
Bronchoneumol. 44:504–506. 2008.(In Spanish). View Article : Google Scholar
|
|
11
|
Raftos JR and Etekk AT: Goitre causing
acute respiratory arrest. ANZ J Surg. 66:331–332. 1996. View Article : Google Scholar
|
|
12
|
Kadhim AL, Sheahan P and Timon C:
Management of life-threatening airway obstruction caused by benign
thyroid disease. J Laryngol Otol. 120:1038–1041. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakadate Y, Fukuda T, Hara H, et al:
Tracheomalacia after reoperation for an adenomatous goiter located
in a unique position. J Anesth. 25:745–748. 2011. View Article : Google Scholar : PubMed/NCBI
|