Introduction
In breast cancer, the common sites of metastasis are
the lung, bones, liver and brain (1)
and metastases to the gastrointestinal tract rarely occur. Among
the histological subtypes, which include ductal carcinoma, lobular
carcinoma, mucinous carcinoma, apocrine carcinoma and spindle cell
carcinoma, invasive lobular carcinoma (ILC) is well known to
metastasize to the gastrointestinal tract, gynecological organs,
peritoneum, and retroperitoneum in comparison with invasive ductal
carcinoma (IDC) (2). Although
patients with gastric metastasis from breast cancer are rarely
encountered, the recognition and awareness of this metastatic
pattern is important in making an accurate diagnosis and providing
appropriate treatment.
The present study reports a rare case of metastatic
gastric cancer from IDC of breast, which was initially diagnosed as
primary gastric linitis plastica.
Case report
In July 2013, a 51-year-old premenopausal woman, who
had a history of partial mastectomy for right breast cancer at the
age of 40, was referred to Toyama City Hospital (Toyoma, Japan) for
a diagnosis of gastric linitis plastica. She presented with upper
abdominal pain and a complaint of body weight loss (−10 kg/6
months). Following partial mastectomy, which was performed in July
2002, the patient received administration of tamoxifen (20 mg,
daily) as adjuvant hormone therapy for 3 years.
Endoscopy revealed a Borrmann type 4 tumor (3) on the greater curvature of the upper
stomach (Fig. 1A). Gastrography
indicated scirrhous gastric cancer localized in the upper stomach
(Fig. 2). Enhanced abdominal computed
tomography (CT) revealed increased wall thickness of the stomach
and left hydronephrosis. Nodal metastasis and liver metastasis were
not detected. Peritoneal metastasis and malignant ascites were also
not detected. Abdominal magnetic resonance imaging revealed
hydronephrosis with stenosis of the uretovesical junction,
indicating retroperitoneal metastasis. Chest CT detected a left
lung tumor that had invaded the left upper bronchus. Bronchial
fiberscopy revealed left upper bronchial stenosis by the extrinsic
tumor (Fig. 1B). The biopsy specimens
of the stomach demonstrated poorly differentiated adenocarcinoma,
while those of the lung tumor also revealed poorly differentiated
adenocarcinoma, suggestive of a metastatic lung tumor (Fig. 3). Levels of tumor markers were within
normal limits, as follows: Carcinoembryonic antigen (CEA), 1.7
ng/ml (normal, <5.0 ng/ml); carbohydrate antigen (CA) 19-9, 6.2
ng/ml (normal, <37.0 ng/ml); CA125, 10.7 U/ml (normal, <35.0
U/ml); and CA15-3, 12.6 U/ml (normal, <28.0 U/ml).
Immunohistochemistry (IHC) revealed that the biopsy
specimens of the gastric and lung tumors were estrogen receptor
(ER) positive/progesterone receptor (PgR) positive/human epithelial
growth factor receptor-2 (HER2) negative (Fig. 4). IHC also indicated positivity for
cytokeratin (CK) 7 and negativity for CK20 in both tumors. By
contrast, the histology of the original breast cancer was IDC with
a solid-tubular type (Fig. 3), which
was 3.5 cm, ER positive, PgR positive, HER2 negative, and without
nodal involvement. Thereafter, these molecular characteristics
indicated metastatic gastric carcinoma from the breast cancer with
lung metastasis. In addition, left hydronephrosis was probably
caused by the retroperitoneal metastasis from the breast origin.
However, the possibility of primary gastric cancer could not be
completely ruled out by the endoscopic biopsied materials, even in
combination with IHC.
When comparing the prognosis of recurrent breast
cancer at a later stage without a history of receiving chemotherapy
with that of primary gastric linitis plastica, the gastric
malignancy would be more life-threatening in the case of primary
gastric cancer. The therapeutic strategy was explained to the
patient, who decided to undergo a surgical resection of the gastric
tumor for local control of the gastric lesion. Subsequently, a
total gastrectomy with splenectomy was performed after confirming
the absence of macroscopic peritoneal dissemination and no evidence
of cancer cells on intraoperative peritoneal lavage cytology. The
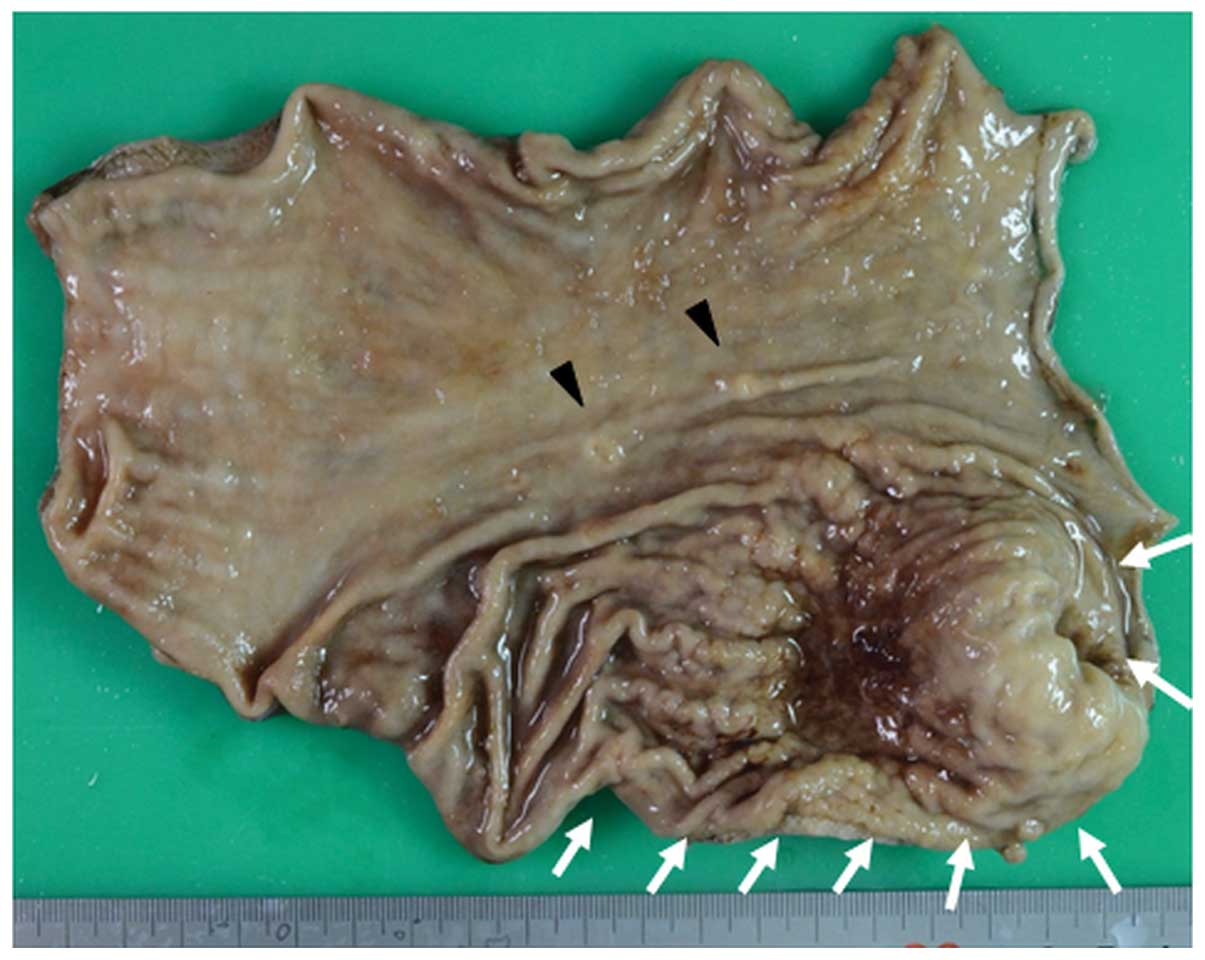
postoperative period was uneventful. Macroscopic findings of the
resected stomach revealed multiple gastric lesions (Fig. 5). Pathological examination of the
resected specimens provided a definite diagnosis of multiple
metastatic gastric carcinomas from IDC of the breast. Based on the
diagnosis, administration of tamoxifen was restarted as endocrine
therapy. After a one-year follow-up period, the patient was
asymptomatic and regular examinations have not demonstrated a
relapse of the disease.
Written informed consent for the present study was
obtained from the patient.
Discussion
Gastric metastases are predominantly a result of
malignant melanoma, followed by lung and breast cancer (4,5).
Metastatic lesions due to hematogenous or lymphatic spread usually
implant in the submucosal layer of the stomach, appearing as one or
multiple submucosal nodules, sometimes accompanied by ulcerative
change and large masses (6). Hence,
localized lesions tend to exhibit submucosal appearance and
diffused lesions may appear to be scirrhous gastric cancer on
endoscopical findings (7). Since
metastatic lesions of stomach cancer often invade the gastric wall
without mucosal destruction, endoscopic biopsy often presents as a
false negative (8). Therefore, in
certain cases, deep biopsies are recommended to obtain sufficient
materials for histological diagnosis and special staining. Madeya
et al (9) reported that 73% of
patients with gastric metastases had diffuse intramural
infiltration presenting as linitis plastica. As for breast cancer,
ILC has been reported to be the most common type that metastasizes
to the stomach mimicking gastric linitis plastica (10). However, gastric metastasis from IDC of
breast presenting linitis plastic has not been described
previously. In the present case, histological examination revealed
IDC. Although the possibility of ILC was considered for the
original breast cancer, no evidence of ILC was demonstrated because
E-cadherin expression was not reduced when assessed by IHC.
Metastatic gastric linitis plastica is clinically
indistinguishable from primary gastric linitis plastica (5), as was observed in the present case. As a
supplemental diagnostic tool, IHC is often used for exploration of
molecular characteristics. Since about 80% of human breast tumors
express hormone receptors (10,11), ER
and PgR have been used as reliable markers to determine the breast
origin. By contrast, it is well known that ER, PgR, and HER2
expression may be altered at the metastatic site over the course of
disease progression (12). Previous
reports also have demonstrated that the discordance of ER and PgR
status between primary breast cancer and those metastases is
15–40%, and most of the discordances included loss of ER and PgR
expression (13,14). While expression of the hormone
receptors plays a major role in progression of breast cancer, it is
little known that primary gastric carcinomas also express ER and
PgR in some cases; according to Matsui et al (15), the positivity rates of ER and PgR are
32 and 12%, respectively in gastric cancer patients. Tokunaga et
al (16) also described that
primary gastric carcinoma expressed ER in 26.6% and PgR in 20.6%.
In summary, it is concluded that regardless of whether a gastric
lesion derives from the stomach or breast, discordance of ER and
PgR status is likely to occur regardless. Therefore, ER or PgR
status is not always a suitable diagnostic marker to confirm that a
tumor originated from the breast. However, concordance of these
hormone receptor expression levels between primary and secondary
lesions may be useful for a differential diagnosis. And their
combination with other supplemental diagnostic markers would be
valuable to improve the accuracy of diagnosis. Apart from the
expression of hormone receptors, the CK7+/CK20-group may also be
used to characterize a primary breast tumor: 33% of primary gastric
cancers exhibit a CK7+/CK20− expression
phenotype (17). Mammoglobin has been
also described as a valuable specific marker of breast origin. Its
expression rate has been reported to be 47.8–80% in primary and
metastatic breast tumors (18–20). In
contrast to ER and PgR expression, the expression of mammoglobin
does not change at the metastatic site (21).
A clinical image of a metastatic gastric tumor is
important in addition to histological examination for a diagnosis.
The first and foremost priority is to establish whether there are
metastatic lesions in other organs. In the present case, gastric
metastasis was the first presentation of the disease, though the
other asymptomatic metastases were also complicated. If lesions
within other organs exist, they should be differentiated from
metastases of the breast origin. Secondly, gastric metastasis often
presents as multiple lesions and tends to be located in the middle
or upper third of the stomach (22).
In the present case, a retrospective observation of the endoscopic
images enabled the detection of another overlooked lesion in the
middle of the stomach (Fig. 5).
Comparison with the histology of the second lesion's biopsy made
the diagnosis of metastatic gastric cancer more reliable.
Thereafter, at an endoscopic examination, information on a
patient's clinical history, especially for ILC, would be useful to
determine whether the gastric lesion derived from the breast or
stomach. In cases where there is a history of breast cancer,
comparison with the original histological slides of the primary
breast cancer should be made to differentiate gastric metastasis
from primary gastric cancer.
Distinguishing between primary and metastatic
gastric carcinoma in patients with a history of breast cancer is
important because the treatment completely differs depending on
whether the primary lesion derives from the stomach or breast. In
the case of primary gastric cancer, surgical resection is the most
effective treatment for patients without distant and peritoneal
metastasis. In regards to breast cancer, because metastasis of
breast cancer is a systemic disease, metastatic gastric cancer is
indicated for systemic therapy with chemotherapy and hormone
therapy. In atypical cases of metastatic gastric cancer affecting
general condition, including uncontrollable gastrointestinal
bleeding and obstruction, gastrectomy or gastrojejunostomy may be
indicated as palliative surgery.
Metastatic gastric carcinoma is relatively rare,
accounting for 2–18% of breast cancer patients (23). Considering the high incidence of
breast cancer and low incidence of gastric linitis plastica,
clinicians should not exclude the possibility of a secondary
gastric lesion from the breast origin in any woman who has been
diagnosed with gastric linitis plastica. Particularly in a patient
with a history of ILC, endoscopic examinations should be performed
carefully (24). If metastasis to the
stomach is definitively diagnosed, unnecessary surgery may be
avoided.
In conclusion, it is important to make an accurate
diagnosis in combination with IHC for metastatic gastric carcinoma.
To the best of our knowledge, metastatic gastric carcinoma derived
from the breast presenting as linitis plastica 11 years, as was
observed in the present study, following the surgical removal of
IDC has not been described previously.
References
|
1
|
Cummings MC, Simpson PT, Reid LE,
Jayanthan J, Skerman J, Song S, McCart Reed AE, Kutasovic JR, Morey
AL, Marquart L, et al: Metastatic progression of breast cancer:
Insights from 50 years of autopsies. J Pathol. 232:23–31. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Borst MJ and Ingold JA: Metastatic
patterns of invasive lobular versus invasive ductal carcinoma of
the breast. Surgery. 114:637–641. 1993.PubMed/NCBI
|
|
3
|
Kitamura K, Beppu R, Anai H, Ikejiri K,
Yakabe S, Sugimachi K and Saku M: Clinicopathologic study of
patients with Borrmann type IV gastric carcinoma. J Surg Oncol.
58:112–117. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Campoli PM, Ejima FH, Cardoso DM, Silva
OQ, Santana Filho JB, Queiroz Barreto PA, Machado MM, Mota ED,
Araujo Filho JA, Alencar Rde C and Mota OM: Metastatic cancer to
the stomach. Gastric Cancer. 9:19–25. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Oda Kondo H, Yamao T, Saito D, Ono H,
Gotoda T, Yamaguchi H, Yoshida S and Shimoda T: Metastatic tumors
to the stomach: Analysis of 54 patients diagnosed at endoscopy and
347 autopsy cases. Endoscopy. 33:507–510. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Menuck LS and Amberg JR: Metastatic
disease involving the stomach. Am J Dig Dis. 20:903–913. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Levine MS, Kong V, Rubesin SE, Laufer I
and Herlinger H: Scirrhous carcinoma of the stomach: Radiologic and
endoscopic diagnosis. Radiology. 175:151–154. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pectasides D, Psyrri A, Pliarchopoulou K,
Floros T, Papaxoinis G, Skondra M, Papatsibas G, Macheras A,
Athanasas G, Arapantoni-Datioti P and Economopoulos T: Gastric
metastases originating from breast cancer: Report of 8 cases and
review of the literature. Anticancer Res. 29:4759–4763.
2009.PubMed/NCBI
|
|
9
|
Madeya S and Börsch G: Gastrointestinal
metastases of breast carcinoma. Gastrointest Endosc. 39:103–104.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Almubarak MM, Laé M, Cacheux W, de Cremoux
P, Pierga JY, Reyal F, Bennett SP, Falcou MC, Salmon RJ, Baranger B
and Mariani P: Gastric metastasis of breast cancer: A single centre
retrospective study. Dig Liver Dis. 43:823–827. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
de Decker L, Campone M, Retornaz F, Berrut
G, Kabeshova A, Molinié F and Beauchet O: Association between
oestrogens receptor expressions in breast cancer and comorbidities:
A cross-sectional, population-based study. PLoS One. 9:e981272014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Amir E, Clemons M, Purdie CA, Miller N,
Quinlan P, Geddie W, Coleman RE, Freedman OC, Jordan LB and
Thompson AM: Tissue confirmation of disease recurrence in breast
cancer patients: Pooled analysis of multi-centre,
multi-disciplinary prospective studies. Cancer Treat Rev.
38:708–714. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Simmons C, Miller N, Geddie W, Gianfelice
D, Oldfield M, Dranitsaris G and Clemons MJ: Does confirmatory
tumor biopsy alter the management of breast cancer patients with
distant metastases? Ann Oncol. 20:1499–1504. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Amir E, Miller N, Geddie W, Freedman O,
Kassam F, Simmons C, Oldfield M, Dranitsaris G, Tomlinson G,
Laupacis A, et al: Prospective study evaluating the impact of
tissue confirmation of metastatic disease in patients with breast
cancer. J Clin Oncol. 30:587–592. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Matsui M, Kojima O, Kawakami S, Uehara Y
and Takahashi T: The prognosis of patients with gastric cancer
possessing sex hormone receptors. Surg Today. 22:421–425. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tokunaga A, Nishi K, Matsukura N, Tanaka
N, Onda M, Shirota A, Asano G and Hayashi K: Estrogen and
progesterone receptors in gastric cancer. Cancer. 57:1376–1379.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tot T: Cytokeratins 20 and 7 as
biomarkers: Usefulness in discriminating primary from metastatic
adenocarcinoma. Eur J Cancer. 38:758–763. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Luo MH, Huang YH, Ni YB, Tsang JY, Chan
SK, Shao MM and Tse GM: Expression of mammaglobin and gross cystic
disease fluid protein-15 in breast carcinomas. Hum Pathol.
44:1241–1250. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Galvis-Jiménez JM, Curtidor H, Patarroyo
MA, Monterrey P and Ramírez-Clavijo SR: Mammaglobin peptide as a
novel biomarker for breast cancer detection. Cancer Biol Ther.
14:327–332. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chia SY, Thike AA, Cheok PY and Tan PH:
Utility of mammaglobin and gross cystic disease fluid protein-15
(GCDFP-15) in confirming a breast origin for recurrent tumors.
Breast. 19:355–359. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Watson MA and Fleming TP: Mammaglobin, a
mammary-specific member of the uteroglobin gene family, is
overexpressed in human breast cancer. Cancer Res. 56:860–865.
1996.PubMed/NCBI
|
|
22
|
De Palma GD, Masone S, Rega M, Simeoli I,
Donisi M, Addeo P, Iannone L, Pilone V and Persico G: Metastatic
tumors to the stomach: Clinical and endoscopic features. World J
Gastroenterol. 12:7326–7328. 2006.PubMed/NCBI
|
|
23
|
Jones GE, Strauss DC, Forshaw MJ, Deere H,
Mahedeva U and Mason RC: Breast cancer metastasis to the stomach
may mimic primary gastric cancer: Report of two cases and review of
literature. World J Surg Oncol. 5:752007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tan L, Piao Y, Liu Z, Han T, Song F, Gao
F, Han Y and Xie X: Breast cancer metastasis to the stomach
confirmed using gastroscopy: A case report. Oncol Lett.
8:1205–1207. 2014.PubMed/NCBI
|