Introduction
Thymic carcinomas are rare invasive neoplasms, and
their clinical course tends to be more aggressive than that of
thymomas (1–3). The World Health Organization has
established a thymic epithelial tumor classification criteria,
according to which, neuroendocrine carcinoma (NEC) is classified as
a subtype of thymic carcinoma, and LCNEC is classified under thymic
NEC as a pulmonary neuroendocrine tumor (4). Thymic NECs are relatively rare neoplasms
that account for only 2–4% of all anterior mediastinal neoplasms
(5) Due to this low frequency rate,
no standard chemotherapy has been established for thymic LCNEC
following failure of initial chemotherapy, which has been
recognized as effective against high-grade NEC. Ogawa et al
(6) previously reported the case of a
patient with primary thymic LCNEC. The patient received a curative
thymectomy and subsequent successful adjuvant chemotherapy. In the
present study, a case of chemorefractory thymic LCNEC that
exhibited a good response to carboplatin and nab-paclitaxel
combination chemotherapy as a salvage therapy is reported. Written
informed consent was obtained from the patient.
Case report
A 59-year-old male was admitted to the Kitasato
University Hospital (Sagamihara, Japan) in April 2009 for further
examination and treatment following the identification of an
abnormal shadow on a regular health check-up chest X-ray. Following
the differential diagnosis of thymic carcinoma, the patient
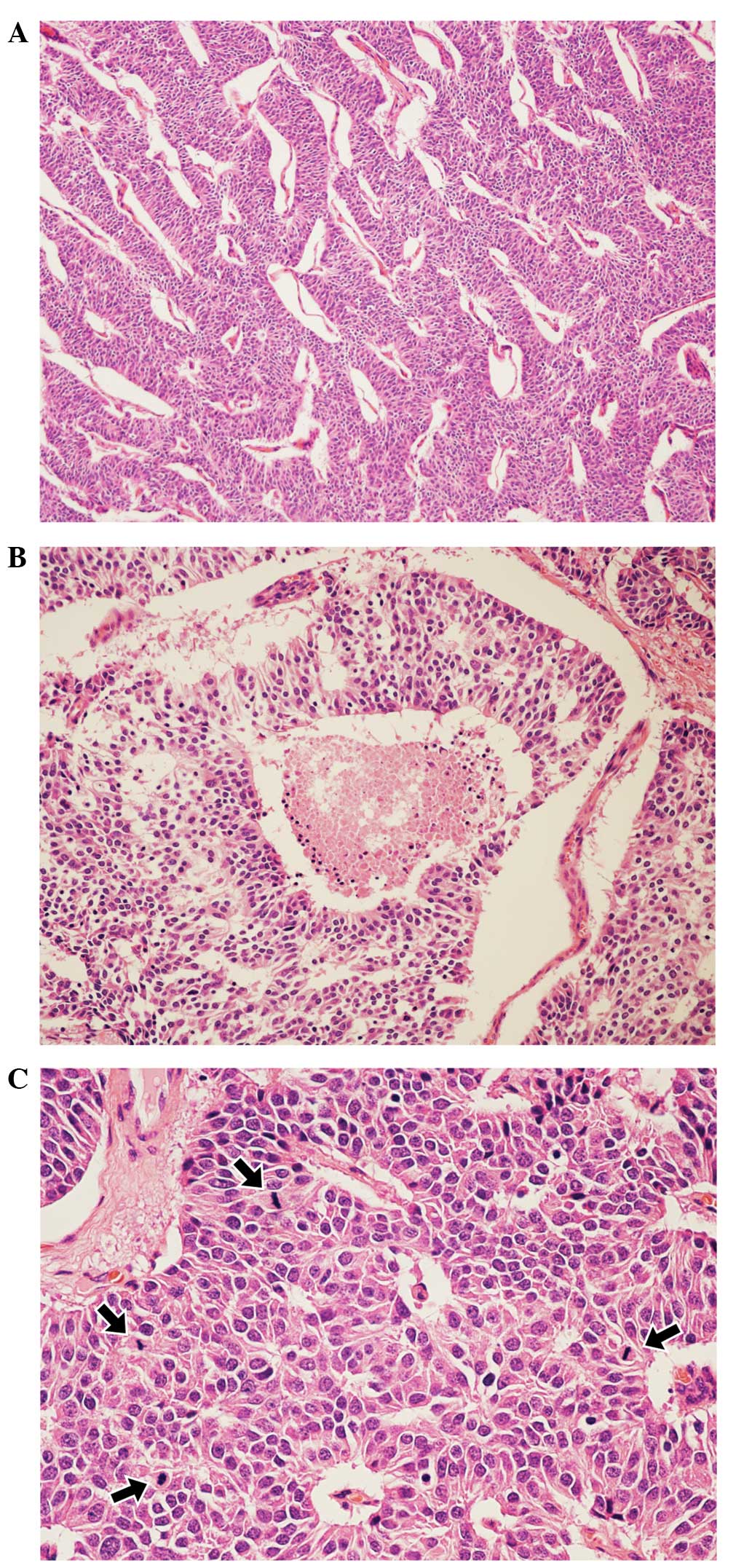
underwent a total thymectomy. The elastic soft tumor was surrounded
by thymic fat tissue and measured 40×35×28 mm. Histologically, the
tumor displayed thick trabeculae with irregular nests separated by
fibrovascular stroma and scattered abortive rosette-like structures
(Fig. 1A). The tumor cells were
large, oval-to-polygonal in shape and contained eosinophilic
granular cytoplasm. The nuclear chromatin was granular, and the
nucleoli were not clearly visible. Small foci of coagulation
necrosis were also observed (Fig.
1B). The average mitotic count was high (30/10 high-power
fields; Fig. 1C), and the Ki-67
indices ranged from 20 to 30%, according to MIB-1 staining.
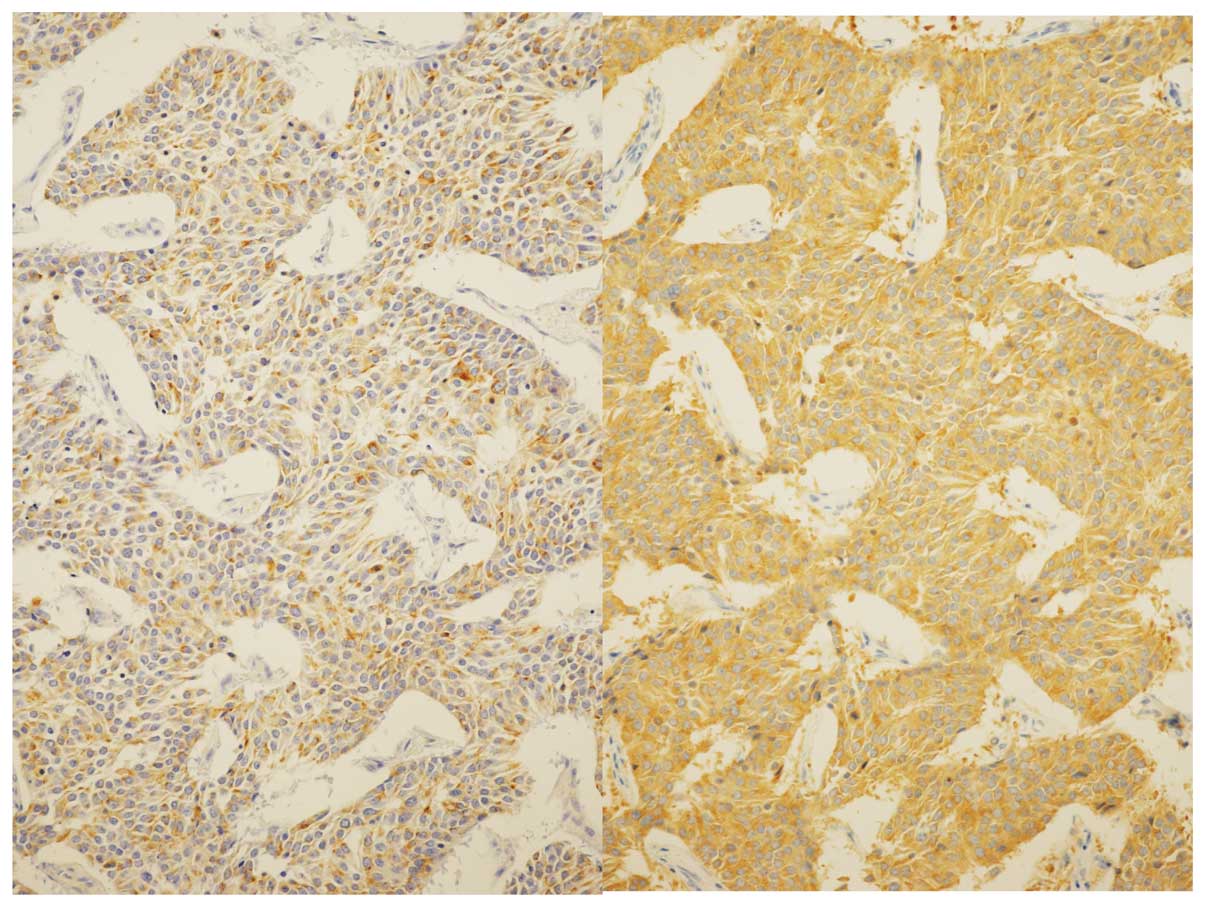
Immunohistochemically, the tumor cells were diffusely positive for
chromogranin A, synaptophysin and neural cell adhesion molecule
(Fig. 2), confirming their
neuroendocrine nature. These pathological findings were consistent
with thymic LCNEC.
The patient was treated with 3 courses (4-week
cycles) of adjuvant chemotherapy, based on a platinum doublet using
a cisplatin (60 mg/m2, day 1) and irinotecan (IP; 60
mg/m2, days1, 8 and 15) regimen. The patient survived
without recurrence for 3 years following total thymectomy. However,
computed tomography (CT) of the chest 4 years later revealed right
pleural dissemination and metastasis in a right mediastinal and a
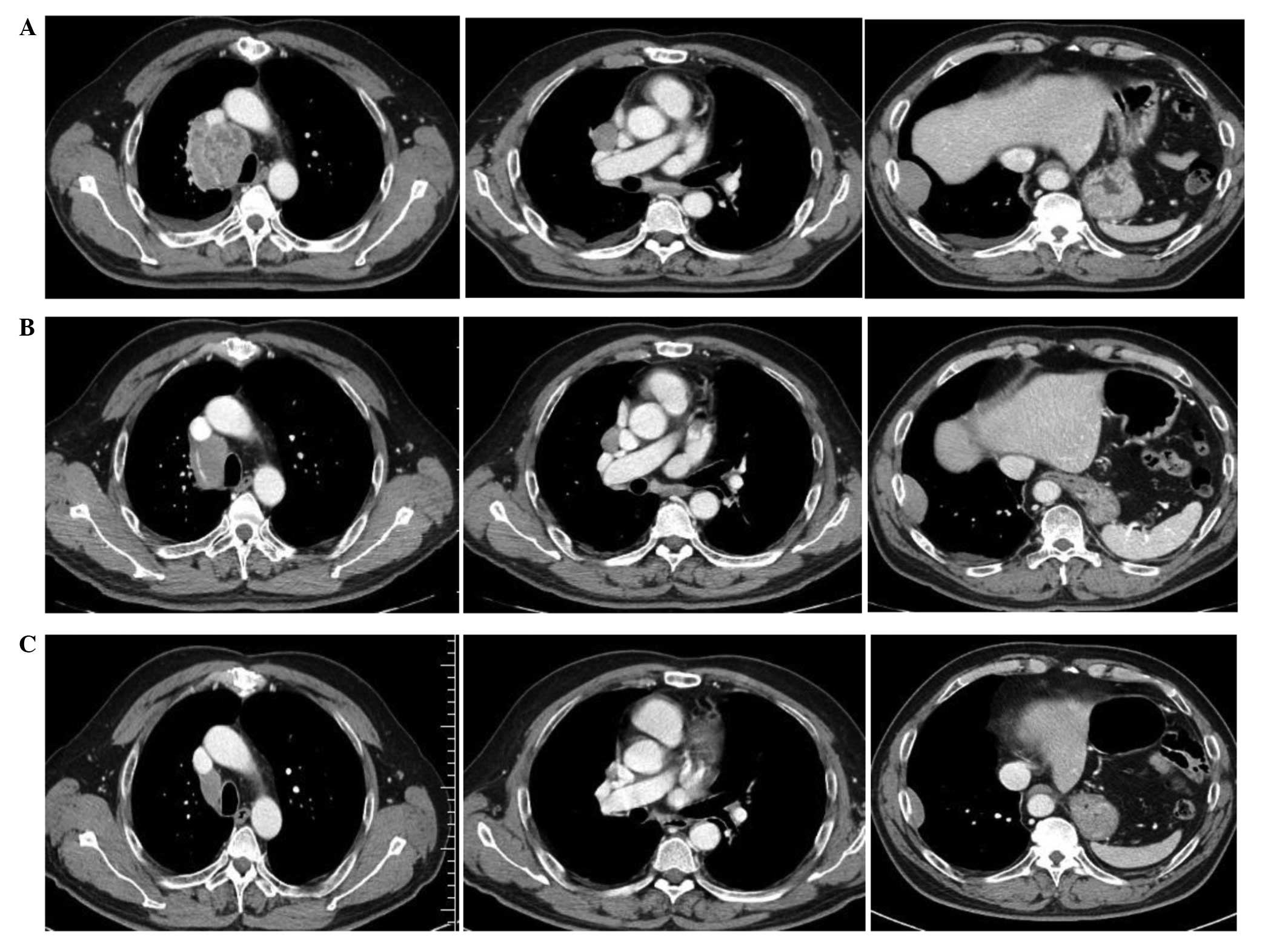
right hilar lymph node. The patient was treated with 2 courses
(3-week cycles) of amrubicin (AMR; 40 mg/m2, days 1–3)
monotherapy, and subsequently re-challenged with 2 courses of the
aforementioned IP regimen, but control of the disease was not
achieved (Fig. 3A).
Since the performance status of the patient and the
function of the major organs were good in June 2014, it was
possible to treat the patient with a salvage chemotherapy regimen
consisting of weekly nab-paclitaxel infusion (100 mg/m2)
plus carboplatin, at an area under the curve of 6, every 4 weeks.
CT scans of the chest following 2 cycles of this regimen revealed a
32% reduction in the sum of the diameters of the target lesions
compared with the baseline, indicating a partial response (Fig. 3B). A reduction in the size of each of
the target lesions was confirmed following 4 cycles of this regimen
in October 2014 (Fig. 3C). The
response was evaluated according to the Response Evaluation
Criteria in Solid Tumors, version 1.1 (7). Additionally, the levels of serum NSE,
which had increased to 21.2 ng/ml (exceeding the institutional
upper limit of the normal values, <16.3 ng/ml) prior to the
treatment, were reduced to 7.0 ng/ml following 4 cycles of this
regimen.
The toxicity profile, reported as the highest
toxicity grades during all the cycles of this regimen, was as
follows: Hematological toxicity in the form of grade 4 neutropenia,
grade 2 leukopenia and grade 1 thrombocytopenia; and
non-hematological toxicity in the form of grade 1 sensory
neuropathy, arthralgia, nausea and alopecia. Due to neutropenia,
the patient was unable to receive nab-paclitaxel on day 15 of the
second and fourth cycles of the regimen, although no dose reduction
was required. Follow-up examinations are performed every 8 weeks
and at present, the patient remains well with a partial response
status.
Discussion
Thymic LCNECs are rare, and their optimal treatment
remains unclear. The results obtained in the present case suggest
that nab-paclitaxel combined with carboplatin may be an effective
treatment for thymic LCNEC. To the best of our knowledge, the
present study is the first case demonstrating the efficacy of the
aforementioned regimen as a treatment for thymic LCNEC. A previous
global phase III study observed that weekly administration of
nab-paclitaxel plus carboplatin yielded a significantly higher
overall response rate compared with solvent-based paclitaxel plus
carboplatin in patients with non-small cell lung cancer (NSCLC)
(8). Nab-paclitaxel, a 130-nm
albumin-bound paclitaxel formulation, is a promising novel agent
for the treatment of NSCLC, and breast and gastric cancer (9,10). A
previous preclinical study reported that nab-paclitaxel exhibited
greater antitumor activity than equitoxic doses of Cremophor-based
paclitaxel in xenograft models of lung (H522), breast (MX-1),
ovarian (SK-OV-3), prostate (PC-3) and colon (HT29) human tumors
(11). The same study reported that
the intratumor concentration of paclitaxel in the MX-1 xenograft
model was 33% higher following administration of nab-paclitaxel
compared with after administration of equal doses of
Cremophor-based paclitaxel. These findings were supported by the
9.9- and 4.2-fold increases observed in endothelial cell binding
and transcytosis, respectively, for nab-paclitaxel compared with
Cremophor-based paclitaxel (11).
Previous studies have indicated that solvent-based
paclitaxel plus carboplatin and carboplatin plus AMR are effective
treatments for unresectable thymic carcinoma. Therefore,
carboplatin-based, cisplatin, doxorubicin, vincristine and
cyclophosphamide, and cisplatin, vincristine, doxorubicin and
etoposide regimens may be suitable treatment options for patients
with thymic LCNECs (12–17). However, the optimal regimen for second
or subsequent lines of chemotherapy for the treatment of thymic
carcinoma remains unclear. Etoposide plus cisplatin, IP and AMR
monotherapy have been demonstrated to be particularly effective in
SCLC (18–20). A previous study indicated that
solvent-based paclitaxel plus carboplatin may be active in SCLC
that is refractory to the above-based regimens (21). Previous studies have reported that the
clinical behavior and prognosis of LCNEC are similar to those of
SCLC, and that SCLC-based regimens are effective in patients with
LCNEC (22,23). Therefore, it appears to be reasonable
to conclude that nab-paclitaxel combined with carboplatin is a
useful option for the treatment of thymic LCNEC that is refractory
to SCLC-based regimens. Further studies regarding the use of this
regimen for the treatment of thymic LCNEC are required.
References
|
1
|
Shimosato Y, Kameya T, Nagai K and Suemasu
K: Squamous cell carcinoma of the thymus: An analysis of eight
cases. Am J Surg Pathol. 1:109–121. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Suster S and Rosai J: Thymic carcinoma. A
clinicopathologic study of 60 cases. Cancer. 67:1025–1032. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yano M, Sasaki H, Yokoyama T, Yukiue H,
Kawano O, Suzuki S and Fujii Y: Thymic carcinoma 30 cases at a
single institution. J Thorac Oncol. 3:265–269. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Marx A, Shimosato Y, Kuo TT, et al: Thymic
neuroendocrine tumours. In: World Health Organization
Classification of Tumours. Pathology and genetics of tumors of the
Lung, Pleura, Thymus and Heart. Travis WD, Brambilla E,
Muller-Hermelink HK and Harris CC: (Lyon). IARC Press. 188–195.
2004.
|
|
5
|
Wick MR and Rosai J: Neuroendocrine
neoplasms of the mediastinum. Semin Diagn Pathol. 8:35–51.
1991.PubMed/NCBI
|
|
6
|
Ogawa F, Iyoda A, Amano H, Nezu K, Jiang
SX, Okayasu I and Satoh Y: Thymic large cell neuroendocrine
carcinoma: Report of a resected case - a case report. J
Cardiothorac Surg. 5:1152010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumours: Revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Socinski MA, Bondarenko I, Karaseva NA,
Makhson AM, Vynnychenko I, Okamoto I, Hon JK, Hirsh V, Bhar P,
Zhang H, et al: Weekly nab-paclitaxel in combination with
carboplatin versus solvent-based paclitaxel plus carboplatin as
first-line therapy in patients with advanced non-small-cell lung
cancer: Final results of a phase III trial. J Clin Oncol.
30:2055–2062. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Koizumi W, Morita S and Sakata Y: A
randomized phase III trial of weekly or 3-weekly doses of
nab-paclitaxel versus weekly doses of Cremophor-based paclitaxel in
patients with previously treated advanced gastric cancer (ABSOLUTE
Trial). Jpn J Clin Oncol. 45:303–306. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chirgwin J and Chua SL: Management of
breast cancer with nanoparticle albumin-bound (nab)-paclitaxel
combination regimens: A clinical review. Breast. 20:394–406. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Desai N, Trieu V, Yao Z, Louie L, Ci S,
Yang A, Tao C, De T, Beals B, Dykes D, et al: Increased antitumor
activity, intratumor paclitaxel concentrations, and endothelial
cell transport of cremophor-free, albumin-bound paclitaxel,
ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res.
12:1317–1324. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lemma GL, Lee JW, Aisner SC, Langer CJ,
Tester WJ, Johnson DH and Loehrer PJ Sr: Phase II study of
carboplatin and paclitaxel in advanced thymoma and thymic
carcinoma. J Clin Oncol. 29:2060–2065. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Igawa S, Murakami H, Takahashi T, Nakamura
Y, Tsuya A, Naito T, Kaira K, Ono A, Shukuya T, Tamiya A, et al:
Efficacy of chemotherapy with carboplatin and paclitaxel for
unresectable thymic carcinoma. Lung Cancer. 67:194–197. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Takeda K, Hirai F, Yamanaka T, Taguchi K,
Daga H, Shimizu J, Kogure Y, Kimura T, Tanaka K, Iwamoto Y, et al:
A multicenter prospective study of carboplatin and paclitaxel for
advanced thymic carcinoma: West Japan Oncology Group 4207L. ASCO
Annual Meeting Abstracts. J Clin Oncol (Suppl). 31:75292013.
|
|
15
|
Kawashima Y, Inoue A, Sugawara S, Harada
M, Kobayashi K, Kozuki T, Kuyama S, Sakakibara T, Maemondo M,
Asahina H, et al: Phase II study of amrubicin (AMR) and carboplatin
(CBDCA) for invasive thymoma (IT) and thymic carcinoma (TC):
NJLCG0803. ASCO Annual Meeting Abstracts. J Clin Oncol (Suppl).
31:75302013.
|
|
16
|
Yoh K, Goto K, Ishii G, Niho S, Ohmatsu H,
Kubota K, Kakinuma R, Nagai K, Suga M and Nishiwaki Y: Weekly
chemotherapy with cisplatin, vincristine, doxorubicin, and
etoposide is an effective treatment for advanced thymic carcinoma.
Cancer. 98:926–931. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Agatsuma T, Koizumi T, Kanda S, Ito M,
Urushihata K, Yamamoto H, Hanaoka M and Kubo K: Combination
chemotherapy with doxorubicin, vincristine, cyclophosphamide, and
platinum compounds for advanced thymic carcinoma. J Thorac Oncol.
6:2130–2134. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jackman DM and Johnson BE: Small-cell lung
cancer. Lancet. 366:1385–1396. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Onoda S, Masuda N, Seto T, Eguchi K,
Takiguchi Y, Isobe H, Okamoto H, Ogura T, Yokoyama A, Seki N, et
al: Thoracic Oncology Research Group Study 0301: Phase II trial of
amrubicin for treatment of refractory or relapsed small-cell lung
cancer: Thoracic Oncology Research Group Study 0301. J Clin Oncol.
24:5448–5453. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Murakami H, Yamamoto N, Shibata T, Takeda
K, Ichinose Y, Ohe Y, Yamamoto N, Takeda Y, Kudoh S, Atagi S, et
al: A single-arm confirmatory study of amrubicin therapy in
patients with refractory small-cell lung cancer: Japan Clinical
Oncology Group Study (JCOG0901). Lung Cancer. 84:67–72. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Groen HJ, Fokkema E, Biesma B, Kwa B, van
Putten JW, Postmus PE and Smit EF: Paclitaxel and carboplatin in
the treatment of small-cell lung cancer patients resistant to
cyclophosphamide, doxorubicin and etoposide: A non-cross-resistant
schedule. J Clin Oncol. 17:927–932. 1999.PubMed/NCBI
|
|
22
|
Iyoda A, Hiroshima K, Moriya Y, Takiguchi
Y, Sekine Y, Shibuya K, Iizasa T, Kimura H, Nakatani Y and Fujisawa
T: Prospective study of adjuvant chemotherapy for pulmonary large
cell neuroendocrine carcinoma. Ann Thorac Surg. 82:1802–1807. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yamazaki S, Sekine I, Matsuno Y, Takei H,
Yamamoto N, Kunitoh H, Ohe Y, Tamura T, Kodama T, Asamura H, et al:
Clinical responses of large cell neuroendocrine carcinoma of the
lung to cisplatin-based chemotherapy. Lung Cancer. 49:217–223.
2005. View Article : Google Scholar : PubMed/NCBI
|