Introduction
Biliary tract cancer (BTC) is a collective term for
a heterogenous group of tumors, including cancer arising from the
gallbladder and bile ducts, as well as adenocarcinoma of the
ampulla of Vater. Although considered relatively rare in the US
[5,000 new cases diagnosed annually (1)] and European countries (1,200 cases per
annum in the UK) (2,3), it has a much higher prevalence in Latin
America (4) and East Asia. In Japan,
the incidence is 10-fold of that in the West, with 17,311
mortalities from BTC in 2007, making it the sixth leading cause of
cancer mortality in Japan (5).
Furthermore, the incidence, particularly of intrahepatic
cholangiocarcinoma, has been increasing in the US, Japan, UK and
Australia since the 1970s (6–8). Surgical removal of the tumor is the only
curative treatment. However, the majority of patients are diagnosed
when the disease has reached an advanced-stage, making them
ineligible for complete surgical resection. Furthermore, recurrence
is common even following complete resection, and is usually only
amenable to palliative chemotherapy (9). In 2010, a phase III trial found that
cisplatin in combination with gemcitabine is an appropriate option
for the treatment of patients with advanced BTC (10). However, patients with advanced BTC
still have a poor prognosis, with a median survival of <1 year
(10–12). Therefore, future research on BTC must
aim to enhance the effectiveness of chemotherapeutic regimens.
It has been well established increased intracellular
glutathione (GSH) is associated with resistance to chemotherapy and
irradiation and, correspondingly, that the reduction of GSH levels
is associated with sensitization to these two types of therapy
(13). We previously demonstrated
that emodin, a natural anthraquinone isolated from traditional
Chinese herbal medicines, enhances cisplatin-induced apoptosis in
gallbladder cancer cells, in vitro and in vivo, via
depletion of GSH and downregulation of multidrug resistance-related
protein 1 (14). Although emodin
provides a therapeutically feasible approach to overcome
chemoresistance in gallbladder cancer cells, little clinical trial
data regarding emodin is available, and the development of an
emodin-based drug remains in the experimental stages. Oral
ingestion of large amounts of emodin may lead to stomach cramping,
gas production, bloating and diarrhea (15–17).
Therefore, it is considered that emodin tends to exacerbate the
gastrointestinal side effects and contribute to patient intolerance
of chemotherapy. For these reasons, emodin may not be an ideal
chemosensitizer. Other compounds must be tested to develop
effective and safe drugs capable of enhancing the chemosensitivity
of BTC cells.
Buthionine sulfoximine (BSO) is a specific inhibitor
of γ-glutamyl-cysteine synthetase and is thus able to block the
rate-limiting step of GSH biosynthesis. Depletion of GSH by BSO
restores the sensitivity of resistant tumors to drugs in
vitro and in vivo (18). A
number of research groups undertook phase I clinical studies to
determine clinically whether BSO produced the desired biochemical
end point of GSH depletion. In these preliminary studies, it was
revealed that continuous infusion of BSO was relatively non-toxic
and resulted in the depletion of tumor GSH in patients with
advanced cancers (ovarian, lung, breast and colon cancer, and
melanoma) (19–21). These results prompted the current
study, which aimed to investigate the effect of BSO combined with
cisplatin and gemcitabine in BTC cells.
Previous studies have demonstrated that BSO is able
to enhance the cytotoxic effect of certain drugs, including
cisplatin, azathioprine and melphalan, in cancer cells (22–25).
However, the synergistic effect of BSO and cisplatin in BTC cells
remains unknown, and there are no available reports regarding
sensitization to gemcitabine by BSO. Therefore, the purpose of the
present study was to demonstrate whether BSO was capable of
potentiating the anticancer effects of cisplatin or gemcitabine in
BTC cells, and to investigate the possible mechanism.
Materials and methods
Cell culture and reagents
Human gallbladder cancer (GBC-SD) and human
cholangiocarcinoma (RBE) cell lines were obtained from the Cell
Bank of the Shanghai Institutes for Biological Sciences, Chinese
Academy of Sciences (Shanghai, China). GBC-SD and RBE cells were
maintained in RPMI-1640 (GE Healthcare Life Sciences, Logan, UT,
USA) supplemented with 10% fetal bovine serum (Gibco; Thermo Fisher
Scientific, Inc., Waltham, MA, USA). Cells were cultured in a
humidified atmosphere of 5% CO2 at 37°C.
BSO was purchased from Sigma-Aldrich (St. Louis, MO,
USA). Gemcitabine was purchased from Jiangsu Hansoh Pharmaceutical
Co., Ltd. (Lianyungang, China), and cisplatin was obtained from
Qilu Pharmaceutical Co., Ltd. (Jinan, China).
Human GBC-SD and RBE cells were pretreated with 50
µM BSO for 24 h before exposure to 4 or 8 µg/ml cisplatin or 0.5
mg/ml gemcitabine for 24 h. The cells were then collected and the
cytotoxic effects examined.
Cell viability and apoptosis
analysis
Cell viability was assayed using a
3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT)
assay (Sigma-Aldrich), as previously described (26). Briefly, the cells were seeded in a
96-well plate at a density of 10,000 cells/well. Following
overnight incubation in a humidified atmosphere of 5%
CO2 at 37°C, each well was refreshed with 0.2 ml
serum-free medium (SFM) containing 50 µM BSO for a further day. The
cells were then pretreated with 0.2 ml SFM containing 50 µM BSO for
24 h. Gemcitabine (500 µg/ml) or cisplatin (4 or 8 µg/ml) were
subsequently added to the medium for an additional 24 h. Cells were
not washed between treatments. Finally, cell viability was assessed
with an MTT reagent and by measuring the absorbance at a wavelength
of 570 nm using a VersaMax™ ELISA Microplate Reader (Molecular
Devices, LLC, Sunnyvale, CA, USA). Relative viability was obtained
from the absorbance of the drug-treated cells divided by that of
the untreated cells. The same experiment was repeated three
times.
Cell apoptosis was assessed using an Annexin
V-fluorescein isothiocyanate (FITC)/propidium iodide (PI) kit (BD
Pharmingen, San Diego, CA, USA) and analyzed using a FACSCalibur
flow cytometer (BD Biosciences, Franklin Lakes, NJ, USA) (27). Briefly, the cells were seeded into
6-well plates and treated with BSO, gemcitabine, cisplatin,
BSO/gemcitabine or BSO/cisplatin. The cells were collected 24 h
later and washed twice using cold phosphate-buffered saline (Gibco;
Thermo Fisher Scientific, Inc.). The cells were then stained using
an Annexin V/PI double staining solution at room temperature. After
15 min, the Annexin V/PI-stained cells were analyzed by flow
cytometry, and the percentage of apoptotic and necrotic cells was
calculated. Cells that were positively stained by Annexin V-FITC
only (early apoptosis), or positive for Annexin V-FITC and PI (late
apoptosis/necrosis) were quantitated, and these two sub-populations
were considered as the overall population of apoptotic cells.
GSH/oxidized GSH (GSSG) ratio
assay
GSH is a tripeptide with a free thiol group that
functions as a major antioxidant in cells. Usually, cellular GSH
exists predominantly in its reduced form, whereas GSSG is present
in small amounts (28). The GSH/GSSG
ratio is often used as an indicator of cellular redox status
(28). Total GSH and GSSG levels were
determined by colorimetric microplate assay kit (Beyotime Institute
of Biotechnology, Haimen, China) as previously described (29,30).
Following treatment with 50 µM BSO, cells were collected by
centrifugation at 10,000 × g for 10 min at 4°C and re-suspended in
20 µl cell culture medium. Cells (10 µl) were mixed with 30 µl 5%
metaphosphoric acid (Beyotime Institute of Biotechnology), then
frozen and thawed twice in liquid nitrogen and 37°C water
respectively. The samples were centrifuged again (using the same
conditions) and the supernatant was used for GSH and GSSG assays.
The total GSH level was measured by performing a DTNB-GSSG
recycling assay (29). The GSSG level
was quantified by the same method as for total GSH after the
supernatant was treated with 1 mol/l 2-vinylpyridine solution to
remove the reduced GSH. The quantity of reduced GSH was obtained by
subtracting the quantity of GSSG from that of total GSH. The
GSH/GSSG ratio was calculated using the following formula: Ratio =
(total GSH − 2GSSG) / GSSG.
Assays of antiapoptotic protein
expression
Myeloid cell leukemia 1 (Mcl-1), B-cell
lymphoma-extra large (Bcl-xL) and B-cell lymphoma 2 (Bcl-2) protein
expression was determined by western blot analysis as previously
described (31). Cells were lysed in
sample solution. Proteins were separated with 10% SDS-PAGE gels
(Sangon Biotech, Shanghai, China) run at 80 V for 30 min, then 120
V for 60 min at room temperature, and transferred to nitrocellulose
membranes (EMD Millipore, Billerica, MA, USA). After blocking with
5% milk in Tris-buffered saline in Tween 20 buffer (TBST; Gibco;
Thermo Fisher Scientific, Inc.), the membrane was incubated
overnight at 4°C with polyclonal rabbit anti-human Bcl-2 (1:200
dilution; cat no. sc-492) and Bcl-xl (1:200 dilution; cat no.
sc-7195; Santa Cruz Biotechnology, Inc., Dallas, TX, USA)
antibodies, and monoclonal rabbit anti-human Mcl-1 antibody (1:800
dilution; cat no. ab32087; Abcam, Cambridge, UK). The membranes
were also incubated with monoclonal mouse anti-human β-actin
antibody (1:1,000 dilution; cat no. sc-47778; Santa Cruz
Biotechnology, Inc.) as the loading control. Following incubation,
the membranes were washed three times with TBST. The membranes were
subsequently incubated with goat anti-rabbit or anti-mouse
peroxidase-conjugated secondary antibodies (cat nos. 111-035-003
and 115-035-003; Jackson Immunoresearch Laboratories, Inc., West
Grove, PA, USA) for 2 h at 37°C, prior to detection using ECL
system (cat no. WBKLS0500; EMD Millipore).
Statistical analysis
Data are presented as the mean value ± standard
deviation. SPSS software version 17.0 (SPSS, Inc., Chicago, IL,
USA) was used for statistical analysis. Analysis of variance was
applied for comparison of the means of two or multiple groups. A
value of P<0.05 was considered to indicate statistically
significant differences.
Results
BSO enhances cisplatin-induced
inhibition of cell viability in BTC cells by increasing
apoptosis
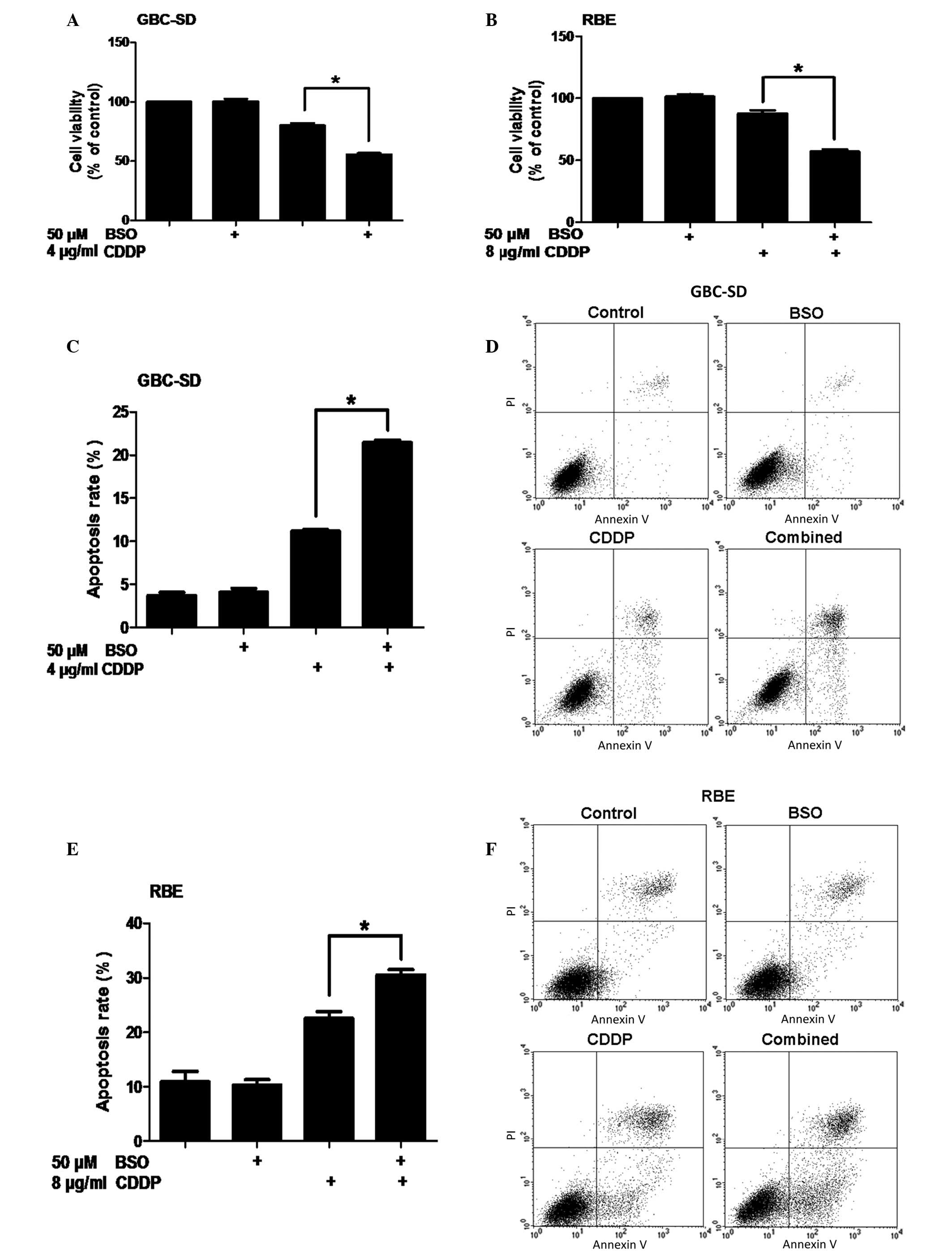
To examine the synergistic effect of BSO on the
inhibition of cell viability by cisplatin, GBC-SD human gallbladder
cancer cells and RBE cholangiocarcinoma cells were pretreated with
50 µM BSO for 24 h before exposure to cisplatin for 24 h. Cell
metabolic activity was measured using an MTT assay. No significant
difference in cell viability was detected between untreated cells
and cells treated only with BSO (P>0.05). However, compared with
the control, GBC-SD and RBE cells that were not pretreated with BSO
experienced 20 and 12% decreases in viability, respectively,
following 24-h exposure to cisplatin (P<0.0001 and P=0.0029,
respectively). In addition, pretreatment of BTC cells with BSO
followed by treatment with cisplatin resulted in reductions in cell
viability of 44% and 43% in the GBC-SD and RBE cell lines,
respectively (Fig. 1A and B).
To determine whether the reduction in cell viability
could be attributed to an increase in apoptosis, Annexin V-FITC/PI
double-labeling flow cytometry was conducted. Compared with
cisplatin alone, pretreatment with BSO followed by cisplatin
treatment resulted in an increase in apoptosis in GBC-SD cells
(P=0.0013; Fig. 1C and D). Similarly,
the BSO/cisplatin co-treatment also led to an increase in apoptosis
in RBE cells (P=0.0374; Fig. 1E and
F). Together, these data demonstrate that BSO is capable of
enhancing cisplatin-induced apoptosis in BTC cells.
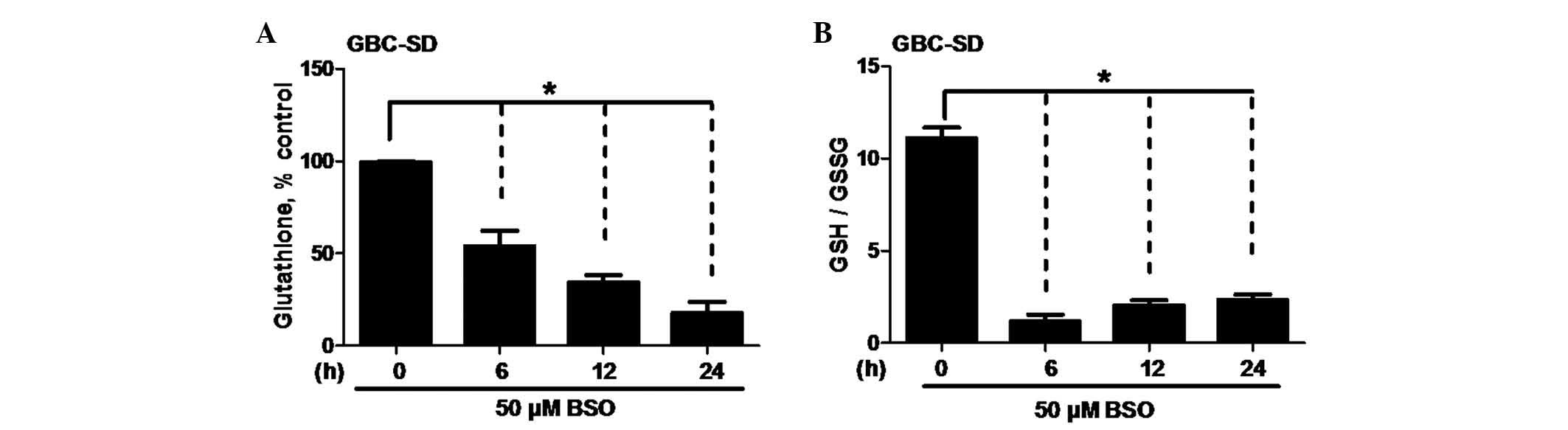
BSO depletes GSH and decreases the
GSH/GSSG ratio in BTC cells
BSO has been demonstrated to deplete intracellular
GSH and induce oxidative stress (19–27,29–32),
and this may sensitize various types of cancer cells to certain
drugs (33–36). To study the oxidative impact of BSO on
the cellular redox state of BTC cells, intracellular GSH levels and
the GSH/GSSG ratio were measured in GBC-SD cells treated with 50 µM
BSO. Notably, BSO reduced the intracellular GSH levels in a
time-dependent manner (P=0.0321; Fig.
2A). Furthermore, BSO decreased the GSH/GSSG ratio, a
reflection of the cellular redox state (P=0.0016; Fig. 2B). These data provide evidence that
the enhancement of BSO on cisplatin-induced apoptosis in BTC cells
is associated with the depletion of GSH.
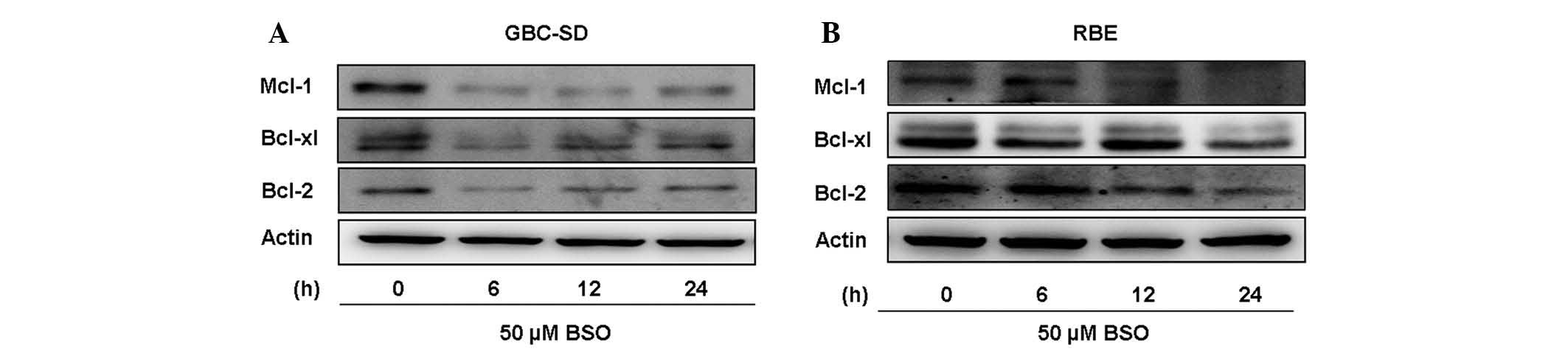
BSO downregulates antiapoptotic
protein expression in BTC cells
Antiapoptotic proteins, including Bcl-2, Bcl-xL and
Mcl-1, are overexpressed in numerous types of cancer cells and
contribute to tumor drug resistance (37). Therefore, inhibition of their
expression may lead to an increased sensitivity to anticancer
drugs. To better understand the mechanism responsible for the
ability of BSO to overcome cisplatin resistance, the expression of
these antiapoptotic proteins was analyzed in lysates from BTC cells
treated with 50 µM BSO for 24 h. Results from western blot analyses
revealed that BSO effectively downregulated Mcl-1, Bcl-2 and Bcl-xL
expression (Fig. 3). The observation
that BSO increases the cytotoxicity of cisplatin may be explained,
at least partially, by downregulation of antiapoptotic proteins in
BTC cells.
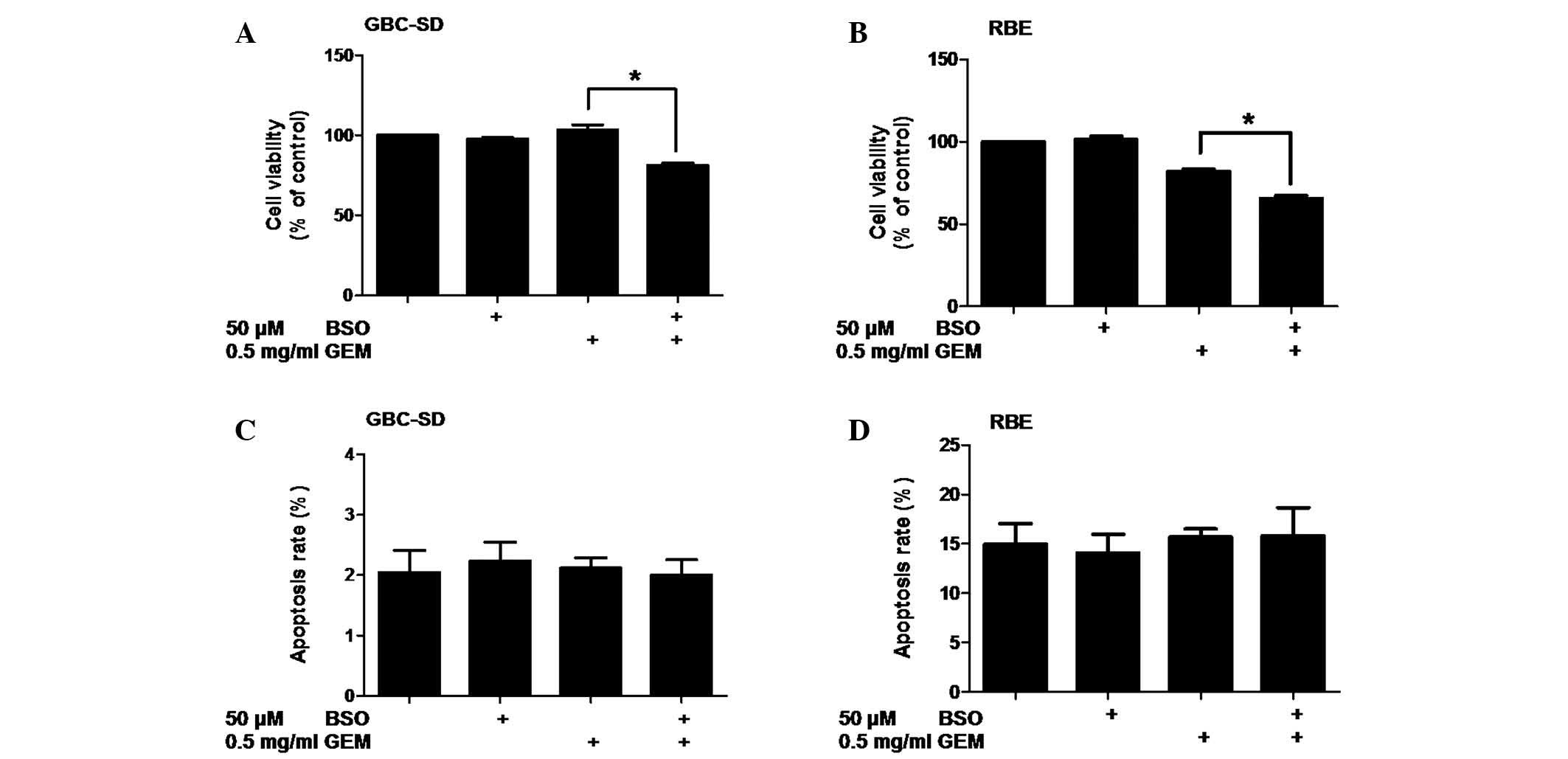
BSO enhances the antiproliferative
effect of gemcitabine on BTC cells
Patients with advanced BTC are currently being
treated with a combination of cisplatin and gemcitabine (10). Therefore, the potential synergistic
effect of BSO with gemcitabine was also examined. Cell viability
was assessed following the treatment of BTC cells with BSO and/or
gemcitabine. The results revealed that a dose of 500 µg/ml
gemcitabine was significantly more effective at reducing cell
viability when it was combined with 50 µM BSO in GBC-SD (P=0.0020)
and RBE (P=0.0005) cells (Fig. 4A and
B). These results suggest that the effects of BSO are not
specific to cisplatin and that it may also enhance the
antiproliferative effect of gemcitabine in BTC cells.
To determine whether BSO enhances the induction of
apoptosis by gemcitabine, the induction of apoptosis in BTC cells
treated with BSO and/or gemcitabine was investigated by Annexin
V-FITC/PI flow cytometry. No increase in apoptosis was detected in
the two cell lines following treatment with gemcitabine alone or
treatment with BSO and gemcitabine (P>0.05; Fig. 4C and D).
Discussion
Chemoresistance remains a major obstacle in
improving responses to BTC treatment, and new drug combinations
offer promising innovations to BTC patients. The present data
suggest that BSO may sensitize BTC cells to the standard first-line
chemotherapeutic agents cisplatin and gemcitabine. This conclusion
is supported by multiple lines of evidence: (i) Cisplatin-induced
apoptosis in BTC cells was significantly enhanced by a sub-toxic
concentration of BSO; (ii) BSO sensitized BTC cells to cisplatin
through GSH depletion and downregulation of antiapoptotic proteins
(Mcl-1, Bcl-2 and Bcl-xL); iii) BSO also enhanced the
antiproliferative effect of gemcitabine in BTC cells.
The therapeutic effect of cisplatin is considered to
be due to the formation of covalent adducts with DNA, which prompt
DNA damage signals to induce apoptosis in a number of types of
solid tumor (14). Cancer cells may
become resistant to platinum-based drugs through multiple
mechanisms, including an increased ability to repair
platinum-induced DNA damage, neutralization of platinum toxicity,
and an increase in drug export (38).
GSH, the most abundant cellular antioxidant, is important in the
promotion of cell survival. GSH is able to confer resistance to
platinum drugs, owing to its ability to form conjugates with
platinum compounds and thus neutralize drug toxicity and promote
the export of the drug (39). In the
present study, a marked reduction of intracellular GSH was detected
following treatment with BSO. Consistently, an increase of
cisplatin-induced cytotoxicity following combined treatment with
BSO and cisplatin was observed, which may be attributed to a
reduction in GSH availability to form platinum conjugates and
thereby the reduction of cellular efflux of the drug. This
hypothesized mechanism may be further tested by examining the total
intracellular platinum and DNA-bound platinum in BTC cells
following treatment with BSO in combination with cisplatin.
Besides reduced drug accumulation, cisplatin
resistance develops through an increased ability to avoid
drug-induced cell damage, cell shrinkage and, therefore, initiation
of apoptosis (40). Apoptosis is
regulated in part by the Bcl-2 family of proteins, which consist of
both proapoptotic [Bcl-2-associated X and Bcl-2-antagonist/killer]
and antiapoptotic (Bcl-2, Bcl-xL and Mcl-l) proteins (41). Thus, downregulation of antiapoptotic
protein expression may negate cisplatin resistance in BTC cells.
The current study provided evidence that Mcl-1, Bcl-2 and Bcl-xL
expression in BTC cells was significantly downregulated by BSO
treatment, indicating that BSO may exert synergistic anticancer
actions through antiapoptotic protein downregulation. As shown in
Fig. 3, BSO induced more significant
downregulation of antiapoptotic proteins in GBC-SD cells than in
RBE cells, which may explain the fact that BSO in combination with
cisplatin increased cell apoptosis to a greater extent in GBC-SD
cells than in RBE cells. However, it remains unclear how BSO
actually suppresses the expression of antiapoptotic proteins.
Previous work has revealed that mild oxidative stress may induce
S-glutathionylation of signal transducer and activator of
transcription 3 (STAT3), leading to the suppression of the STAT3
pathway, downregulation of STAT3-dependent gene expression and
chemosensitization of tumor cells to chemotherapy (42). It has also been established that Mcl-1
and Bcl-2 are regulated by STAT3 (43,44). The
present results indicated that BSO treatment was capable of
inducing oxidative stress in BTC cells (Fig. 2B), suggesting that BSO may also affect
the STAT3 pathway. Thus, further studies are required to test
whether BSO is able to downregulate the expression of antiapoptotic
proteins through S-glutathionylation of STAT3.
In addition, the present findings revealed that BSO
was able to enhance gemcitabine-induced inhibition of cell
viability, but did not affect apoptosis in gemcitabine-treated
cells. This result indicates that the reduction in BTC cell
viability could not be attributed to an increase in apoptosis. BSO
in combination with gemcitabine may decrease cell viability through
induction of cell cycle arrest or other mechanisms. The exact
mechanism of growth inhibition under these conditions, however,
requires further investigation.
In conclusion, the current results indicate that BSO
may significantly enhance the anticancer effects of cisplatin and
gemcitabine in BTC cells in vitro. In phase I trials, the
concentration of BSO in blood has been reported to reach 0.5–1 mM
(19,21). Thus the concentration of BSO used in
the present investigation is clinically achievable. In addition, it
is notable that phase I studies of BSO administered with the
anticancer drug melphalan demonstrated that continuous infusion of
BSO was relatively non-toxic and resulted in depletion of tumor GSH
(16,17). This study adds to a growing body of
evidence that BSO may be a highly effective sensitizer for
chemotherapeutic treatment of BTC patients. Further research is
necessary to evaluate the feasibility of using this therapeutic
strategy in vivo and in clinical trials.
Acknowledgements
This work was supported by grants from the National
Natural Science Foundation of China (grant no. 81072011 awarded to
Dr Jian Wang).
Glossary
Abbreviations
Abbreviations:
|
BTC
|
biliary tract cancer
|
|
BSO
|
buthionine sulfoximine
|
|
GSH
|
glutathione
|
|
FITC
|
fluorescein isothiocyanate
|
|
PI
|
propidium iodide
|
|
GSSG
|
oxidized glutathione
|
|
Mcl-1
|
myeloid cell leukemia 1
|
|
Bcl-xL
|
B-cell lymphoma-extra large
|
|
Bcl-2
|
B-cell lymphoma 2
|
|
STAT3
|
signal transducer and activator of
transcription 3
|
|
MTT
|
3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide
|
References
|
1
|
Lazaridis KN and Gores GJ:
Cholangiocarcinoma. Gastroenterology. 128:1655–1667. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Keane MG, Horsfall L, Rait G and Pereira
SP: A case-control study comparing the incidence of early symptoms
in pancreatic and biliary tract cancer. BMJ Open. 4:e0057202014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Khan SA, Emadossadaty S, Ladep NG, Thomas
HC, Elliott P, Taylor-Robinson SD and Toledano MB: Rising trends in
cholangiocarcinoma: Is the ICD classification system misleading us?
J Hepatol. 56:848–854. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Randi G, Malvezzi M, Levi F, Ferlay J,
Negri E, Franceschi S and La Vecchia C: Epidemiology of biliary
tract cancers: An update. Ann Oncol. 20:146–159. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matsuda T and Marugame T: International
comparisons of cumulative risk of gallbladder cancer and other
biliary tract cancer, from Cancer Incidence in Five Continents Vol.
VIII. Jpn J Clin Oncol. 37:74–75. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Taylor-Robinson SD, Toledano MB, Arora S,
Keegan TJ, Hargreaves S, Beck A, Khan SA, Elliott P and Thomas HC:
Increase in mortality rates from intrahepatic cholangiocarcinoma in
England and Wales 1968–1998. Gut. 48:816–820. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Patel T: Increasing incidence and
mortality of primary intrahepatic cholangiocarcinoma in the United
States. Hepatology. 33:1353–1357. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khan SA, Taylor-Robinson SD, Toledano MB,
Beck A, Elliott P and Thomas HC: Changing international trends in
mortality rates for liver, biliary and pancreatic tumours. J
Hepatol. 37:806–813. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Malka D, Cervera P, Foulon S, Trarbach T,
de la Fouchardière C, Boucher E, Fartoux L, Faivre S, Blanc JF,
Viret F, et al: Gemcitabine and oxaliplatin with or without
cetuximab in advanced biliary-tract cancer (BINGO): A randomised,
open-label, non-comparative phase 2 trial. Lancet Oncol.
15:819–828. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: Cisplatin plus gemcitabine versus gemcitabine for
biliary tract cancer. N Engl J Med. 362:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eckel F and Schmid RM: Chemotherapy in
advanced biliary tract carcinoma: A pooled analysis of clinical
trials. Br J Cancer. 96:896–902. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sharma A, Dwary AD, Mohanti BK, Deo SV,
Pal S, Sreenivas V, Raina V, Shukla NK, Thulkar S, Garg P and
Chaudhary SP: Best supportive care compared with chemotherapy for
unresectable gall bladder cancer: A randomized controlled study. J
Clin Oncol. 28:4581–4586. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Awasthi YC, Chaudhary P, Vatsyayan R,
Sharma A, Awasthi S and Sharma R: Physiological and pharmacological
significance of glutathione-conjugate transport. J Toxicol Environ
Health B Crit Rev. 12:540–551. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang W, Sun YP, Huang XZ, He M, Chen YY,
Shi GY, Li H, Yi J and Wang J: Emodin enhances sensitivity of
gallbladder cancer cells to platinum drugs via glutathion depletion
and MRP1 downregulation. Biochem Pharmacol. 79:1134–1140. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Omar JM, Yang H, Li S, Marquardt RR and
Jones PJ: Development of an improved reverse-phase high-performance
liquid chromatography method for the simultaneous analyses of
trans-/cis-resveratrol, quercetin and emodin in commercial
resveratrol supplements. J Agric Food Chem. 62:5812–5817. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Srinivas G, Babykutty S, Sathiadevan PP
and Srinivas P: Molecular mechanism of emodin action: Transition
from laxative ingredient to an antitumor agent. Med Res Rev.
27:591–608. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu JD, Wang W, Li LS, Chen X and Zhu JX:
Involvement of endogenous prostaglandin in emodin-evoked rat
colonic anion secretion. Biol Pharm Bull. 30:2058–2062. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Anderson CP, Tsai JM, Meek WE, Liu RM,
Tang Y, Forman HJ and Reynolds CP: Depletion of glutathione by
buthionine sulfoxine is cytotoxic for human neuroblastoma cell
lines via apoptosis. Exp Cell Res. 246:183–192. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bailey HH, Ripple G, Tutsch KD,
Arzoomanian RZ, Alberti D, Feierabend C, Mahvi D, Schink J, Pomplun
M, Mulcahy RT and Wilding G: Phase I study of continuous-infusion
L-S,R-buthionine sulfoximine with intravenous melphalan. J Natl
Cancer Inst. 89:1789–1796. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bailey HH, Mulcahy RT, Tutsch KD,
Arzoomanian RZ, Alberti D, Tombes MB, Wilding G, Pomplun M and
Spriggs DR: Phase I clinical trial of intravenous L-buthionine
sulfoximine and melphalan: An attempt at modulation of glutathione.
J Clin Oncol. 12:194–205. 1994.PubMed/NCBI
|
|
21
|
O'Dwyer PJ, Hamilton TC, LaCreta FP, Gallo
JM, Kilpatrick D, Halbherr T, Brennan J, Bookman MA, Hoffman J,
Young RC, et al: Phase I trial of buthionine sulfoximine in
combination with melphalan in patients with cancer. J Clin Oncol.
14:249–256. 1996.PubMed/NCBI
|
|
22
|
Jia Y, Zhang W, Liu H, Peng L, Yang Z and
Lou J: Inhibition of glutathione synthesis reverses Krüppel-like
factor 4-mediated cisplatin resistance. Cancer Chemother Pharmacol.
69:377–385. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tagde A, Singh H, Kang MH and Reynolds CP:
The glutathione synthesis inhibitor buthionine sulfoximine
synergistically enhanced melphalan activity against preclinical
models of multiple myeloma. Blood Cancer J. 4:e2292014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hernandez-Breijo B, Monserrat J,
Ramirez-Rubio S, Cuevas EP, Vara D, Díaz-Laviada I,
Fernández-Moreno MD, Román ID, Gisbert JP and Guijarro LG:
Preclinical evaluation of azathioprine plus buthionine sulfoximine
in the treatment of human hepatocarcinoma and colon carcinoma.
World J Gastroenterol. 17:3899–3911. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chowdhury AA, Chaudhuri J, Biswas N, Manna
A, Chatterjee S, Mahato SK, Chaudhuri U, Jaisankar P and
Bandyopadhyay S: Synergistic apoptosis of CML cells by buthionine
sulfoximine and hydroxychavicol correlates with activation of AIF
and GSH-ROS-JNK-ERK-iNOS pathway. PloS one. 8:e736722013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yi J, Yang J, He R, Gao F, Sang H, Tang X
and Ye RD: Emodin enhances arsenic trioxide-induced apoptosis via
generation of reactive oxygen species and inhibition of survival
signaling. Cancer Res. 64:108–116. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jing Y, Yang J, Wang Y, Li H, Chen Y, Hu
Q, Shi G, Tang X and Yi J: Alteration of subcellular redox
equilibrium and the consequent oxidative modification of nuclear
factor kappaB are critical for anticancer cytotoxicity by emodin, a
reactive oxygen species-producing agent. Free Radic Biol Med.
40:2183–2197. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zitka O, Skalickova S, Gumulec J, Masarik
M, Adam V, Hubalek J, Trnkova L, Kruseova J, Eckschlager T and
Kizek R: Redox status expressed as GSH:GSSG ratio as a marker for
oxidative stress in paediatric tumour patients. Oncol Lett.
4:1247–1253. 2012.PubMed/NCBI
|
|
29
|
Rahman I, Kode A and Biswas SK: Assay for
quantitative determination of glutathione and glutathione disulfide
levels using enzymatic recycling method. Nat Protoc. 1:3159–3165.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Fan J, Cai H, Yang S, Yan L and Tan W:
Comparison between the effects of normoxia and hypoxia on
antioxidant enzymes and glutathione redox state in ex vivo culture
of CD34(+) cells. Comp Biochem Physiol B Biochem Mol Biol.
151:153–158. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Han Y, Huang C, Sun X, Xiang B, Wang M,
Yeh ET, Chen Y, Li H, Shi G, Cang H, et al: SENP3-mediated
de-conjugation of SUMO2/3 from promyelocytic leukemia is correlated
with accelerated cell proliferation under mild oxidative stress. J
Biol Chem. 285:12906–12915. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Liaudat AC, Bohl LP, de Talamoni Tolosa
NG, Maletto B, Pistoresi-Palencia MC and Picotto G: Oxidative
stress, cell cycle arrest and differentiation contribute toward the
antiproliferative action of BSO and calcitriol on Caco-2 cells.
Anticancer Drugs. 25:810–818. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hadzic T, Aykin-Burns N, Zhu Y, Coleman
MC, Leick K, Jacobson GM and Spitz DR: Paclitaxel combined with
inhibitors of glucose and hydroperoxide metabolism enhances breast
cancer cell killing via H2O2-mediated oxidative stress. Free Radic
Biol Med. 48:1024–1033. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Schnelldorfer T, Gansauge S, Gansauge F,
Schlosser S, Beger HG and Nussler AK: Glutathione depletion causes
cell growth inhibition and enhanced apoptosis in pancreatic cancer
cells. Cancer. 89:1440–1447. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rudin CM, Yang Z, Schumaker LM,
VanderWeele DJ, Newkirk K, Egorin MJ, Zuhowski EG and Cullen KJ:
Inhibition of glutathione synthesis reverses Bcl-2-mediated
cisplatin resistance. Cancer Res. 63:312–318. 2003.PubMed/NCBI
|
|
36
|
Meurette O, Lefeuvre-Orfila L, Rebillard
A, Lagadic-Gossmann D and Dimanche-Boitrel MT: Role of
intracellular glutathione in cell sensitivity to the apoptosis
induced by tumor necrosis factor {alpha}-related apoptosis-inducing
ligand/anticancer drug combinations. Clin Cancer Res. 11:3075–3083.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Buolamwini JK: Novel anticancer drug
discovery. Curr Opin Chem Biol. 3:500–509. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wu WJ, Zhang Y, Zeng ZL, Li XB, Hu KS, Luo
HY, Yang J, Huang P and Xu RH: β-phenylethyl isothiocyanate
reverses platinum resistance by a GSH-dependent mechanism in cancer
cells with epithelial-mesenchymal transition phenotype. Biochem
Pharmacol. 85:486–496. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ishikawa T and Ali-Osman F:
Glutathione-associated cis-diamminedichloroplatinum (II) metabolism
and ATP-dependent efflux from leukemia cells. Molecular
characterization of glutathione-platinum complex and its biological
significance. J Biol Chem. 268:20116–20125. 1993.PubMed/NCBI
|
|
40
|
Sorensen BH, Thorsteinsdottir UA and
Lambert IH: Acquired cisplatin resistance in humane ovarian cancer
A2780 cells correlates with shift in taurine homeostasis and
ability to volume regulate. Am J Physiol Cell Physiol.
307:C1071–C1080. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Heiser D, Labi V, Erlacher M and Villunger
A: The Bcl-2 protein family and its role in the development of
neoplastic disease. Exp Gerontol. 39:1125–1135. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Butturini E, de Prati Carcereri A,
Chiavegato G, Rigo A, Cavalieri E, Darra E and Mariotto S: Mild
oxidative stress induces S-glutathionylation of STAT3 and enhances
chemosensitivity of tumoural cells to chemotherapeutic drugs. Free
Radic Biol Med. 65:1322–1330. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lu Z, Wang J, Zheng T, Liang Y, Yin D,
Song R, Pei T, Pan S, Jiang H and Liu L: FTY720 inhibits
proliferation and epithelial-mesenchymal transition in
cholangiocarcinoma by inactivating STAT3 signaling. BMC Cancer.
14:7832014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Deng H, Zhou Z, Tu W, Xia Y, Huang H and
Tian D: Knockdown of astrocyte elevated gene-1 inhibits growth
through suppression of IL-6 secretion in HepG2 human hepatoma
cells. Oncol Lett. 7:101–106. 2014.PubMed/NCBI
|