Introduction
Giant cell tumors (GCTs) are rare bone tumors that
account for ~5% of all primary bone tumors (1). GCT cells have osteoclast-like
properties, and tend to invade and dissolve healthy bone, become
highly vascularized and develop further calcifications around the
periphery of the tumor, but they rarely metastasize. GCTs are most
frequently identified in the long bones, such as the distal femur
or proximal tibia, and 2–5% of GCTs occur in the spine (1). Spinal lesions often involve the body of
the vertebra and may be accompanied by soft tissue swelling
(1). Patients with GCTs usually
present with localized pain and neurological symptoms, such as
radiating pain or hyperesthesia. Si et al (2) presented the characteristic imaging
findings of a series of 30 pathologically confirmed GCTs, of which
5 cases were located in the cervical spine, 15 in the thoracic
spine and 10 in the lumbar spine. A total of 12 cases were located
in the epidural space, causing spinal cord and/or nerve root
compression. Characteristic X-ray and computed tomography (CT)
imaging findings included an osteolytic and expansile lesion with a
‘soap bubble’ or purely lytic appearance. Furthermore, magnetic
resonance imaging (MRI) findings included a well-defined and
expansile mass with heterogeneous low-to-iso signal intensity on
T2-weighted images. In a similar study, Kwon et al (3) reported the MRI findings in 10 cases of
GCTs of the spine, which included 1 lesion at C7 and 3 lesions of
the thoracic, lumbar and cervical spine, respectively. On MRI
examination, 10 cases exhibited an expansile mass with
heterogeneous low to intermediate signal intensity on the
T2-weighted images, 9 cases exhibited a curvilinear area of signal
void on T1- and T2-weighted images and 4 cases exhibited cystic
changes within the mass. Martin et al (4) reported a series of 23 cases of GCTs of
the sacrum and spine. The mean age at diagnosis was ~35 years, and
the typical symptoms on presentation included pain and neurological
deficits at the site of tumor involvement, with symptoms which had
been present for a number of months prior to diagnosis. Treatments
included arterial embolization, intralesional surgical resection
and/or en bloc resection, and it was found that en
bloc resection was associated with the lowest recurrence
rate.
Surgery is the primary treatment strategy for GCTs;
however, the recurrence rates range between 15 and 45% (5,6). En bloc
wide resection is associated with lower recurrence rates than
intralesional curettage (5 vs. 25%), however, it carries a higher
risk of morbidity (7). Treatment by
intralesional curettage is typically accompanied by the application
of phenol, polymethylmethacrylate, liquid nitrogen and bone
grafting (8). Furthermore, radiation
therapy may improve local control, but may also increase the risk
of sarcomatous transformation (9,10). No
adequate medical therapies have been reported, although positive
effects have been described in response to bisphosphonates
(11), interferon α (12) and denosumab (13).
The current report describes an unusual case of a
GCT of the thoracic spine in a middle-aged male in which
obstructive hydrocephalus and alteration in consciousness developed
6 months after onset of the initial symptoms. The patient was
treated with a ventriculoperitoneal shunt, however, surgery was not
performed due to the size and location of the lesion. During 30
months of follow-up the size of the tumor remained unchanged. To
the best of our knowledge, spinal GCTs have not been previously
reported in association with hydrocephalus.
Case report
A 48-year-old male presented to the Department of
Emergency Medicine, Wan Fang Hospital (Taipei, Taiwan) on September
17, 2007 with bilateral lower limb weakness. Over 1 week, the
symptoms progressed rapidly, from loss of sensation below the
thoracic level and urinary retention to bilateral lower limb
weakness and the inability to walk. No history of major systemic
diseases was recorded. Physical examination disclosed increased
lower limb deep tendon reflexes, spastic gait with difficulty
walking, sensory loss below the thoracic level and urinary
retention, requiring the placement of a Foley catheter. Brain
computed tomography (CT) without contrast, performed to discard
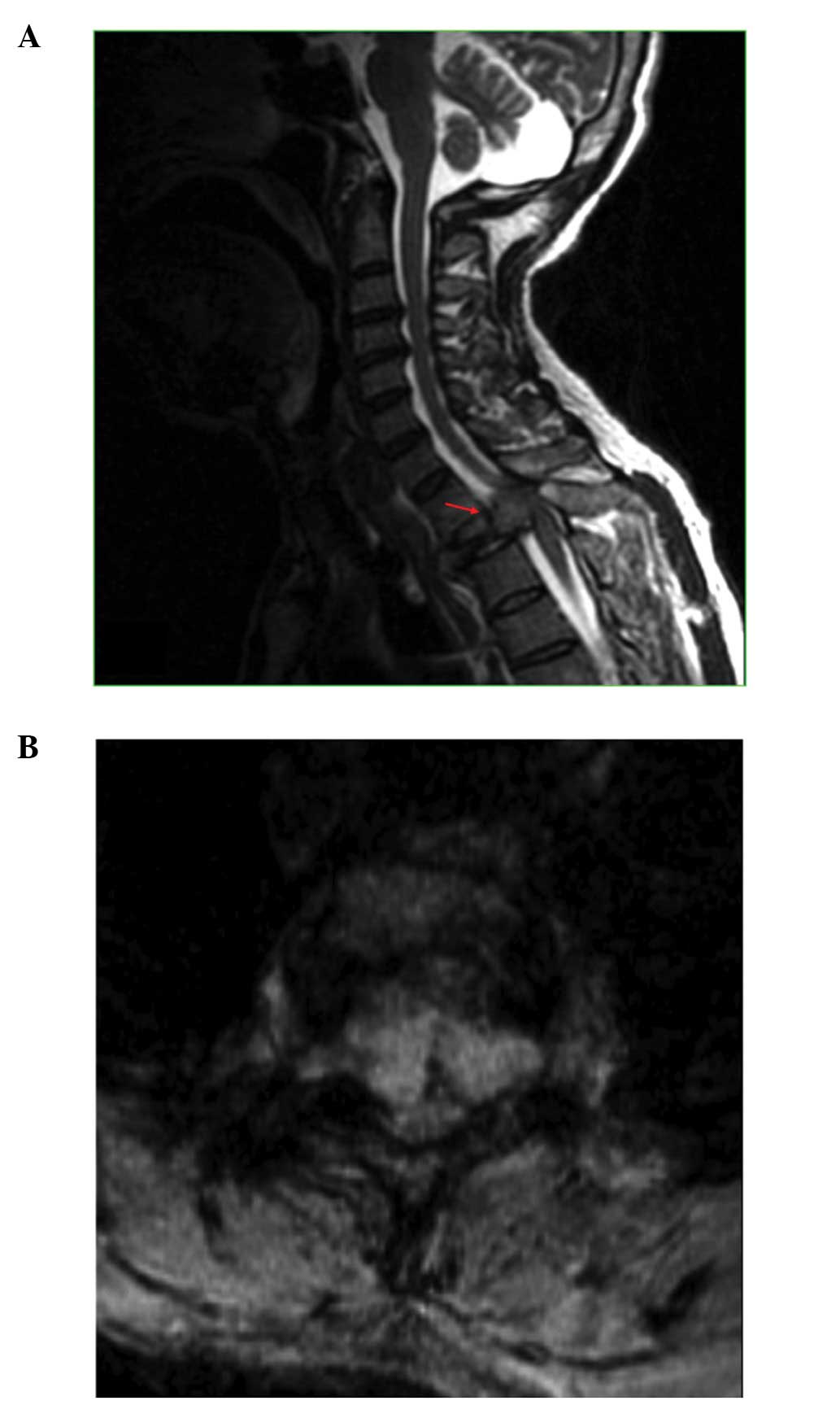
intracranial conditions, indicated no abnormalities. A whole-spine
magnetic resonance (MR) analysis indicated a compression fracture
at T2 and a soft tissue mass with epidural invasion and central
spinal stenosis (Fig. 1A). The soft
tissue lesion was visible around the anterior-, para- and
retro-vertebral regions (Fig. 1B). A
gadolinium-enhanced MR analysis demonstrated iso-to-low T1- and
T2-weighted images of the soft tissue mass. The symptoms were
hypothesized to be a result of a T2 compression fracture possibly
due to a bone tumor, metastasis or infection. Next, a T2
decompressive laminectomy was performed, and biopsy of the T2
vertebra under C-arm fluoroscopy was attempted through the
pedicles. However, no specific pathological findings were observed
during the histological examination of the tissue, which revealed
degenerated bony tissue, fibrocartilage and ligamentous tissues and
marrow elements with normal maturation of hematopoietic cells, but
no malignant tissue. Consequently, the patient was discharged 1
month later, and was able to ambulate using a walker. The patient
and his family then decided to consult with a traditional healer,
which is a common practice in Asian countries.
After ~6 months, the patient was readmitted to the
Department of Emergency Medicine with a sudden onset of alteration
in consciousness for an extended period of time in which the
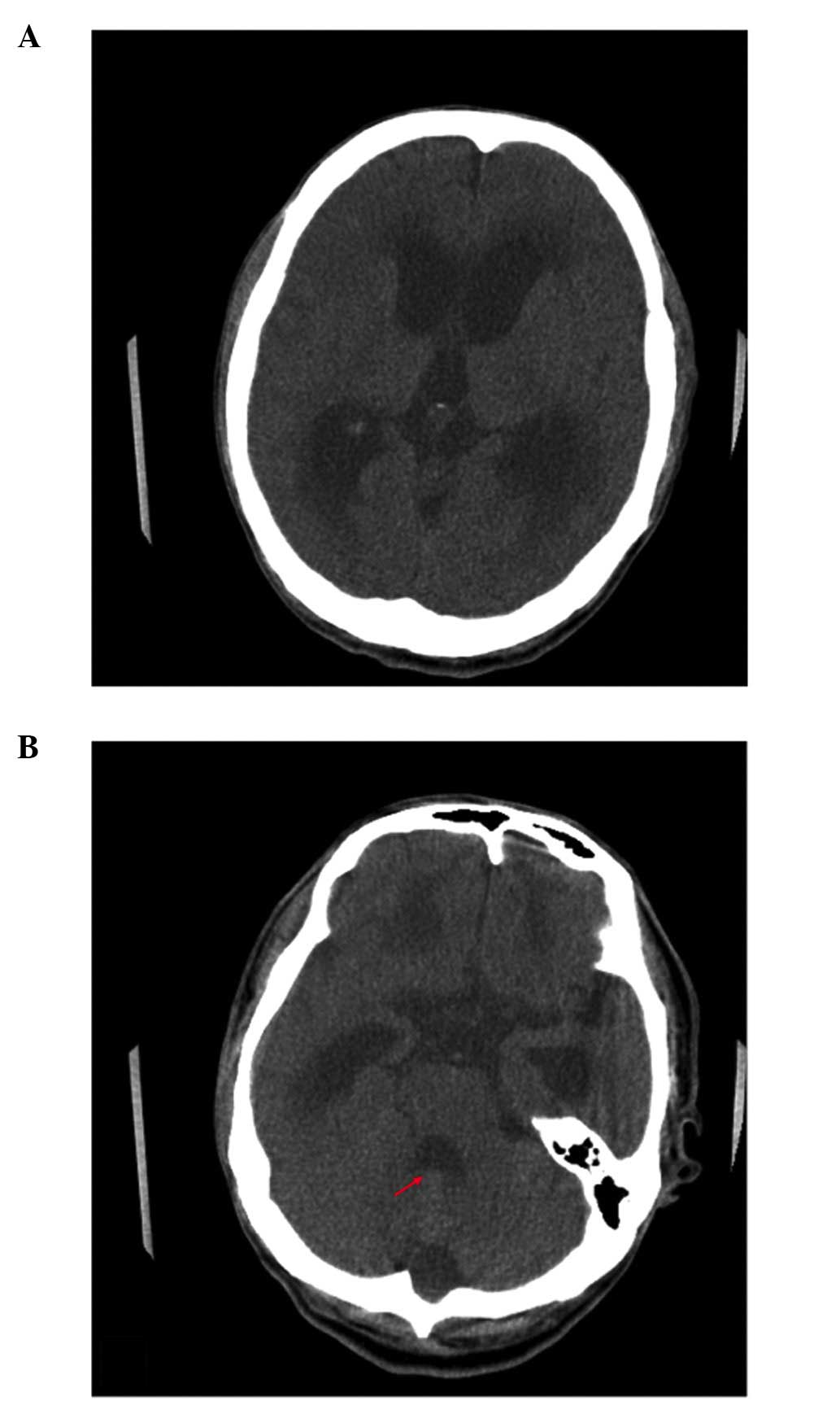
patient was unable to follow simple commands. Brain CT indicated
marked dilatation of the ventricles, suggesting hydrocephalus
(Fig. 2A). Low density of the
periventricular area, possibly due to transependymal cerebrospinal
fluid (CSF) resorption, was also noted. A gadolinium-enhanced MR
analysis was performed to rule out distant metastasis of the tumor
from the thoracic spine to the brain. However, no evidence of brain
tumor was noted in the brain parenchyma. Marked dilatation of the
ventricles, including the fourth ventricle, with transependymal CSF
resorption, which is consistent with hydrocephalus, was observed
(Fig. 2B). No evidence of acute
infarction was detected in the diffusion-weighted image. An
abnormally high-intensity T2-weighted signal was observed in the
lower medulla and cervical cord, accompanied by swelling. CSF flow
studies were quantitatively evaluated by measuring the peak
velocity in the cerebral aqueduct using cine-phase contrast MR
imaging. The maximum CSF velocity at the cerebral aqueduct of the
patient was 12.3 cm/sec (normal range, 4–5 cm/sec) (14), demonstrating abnormal hyperdynamic CSF
motion.
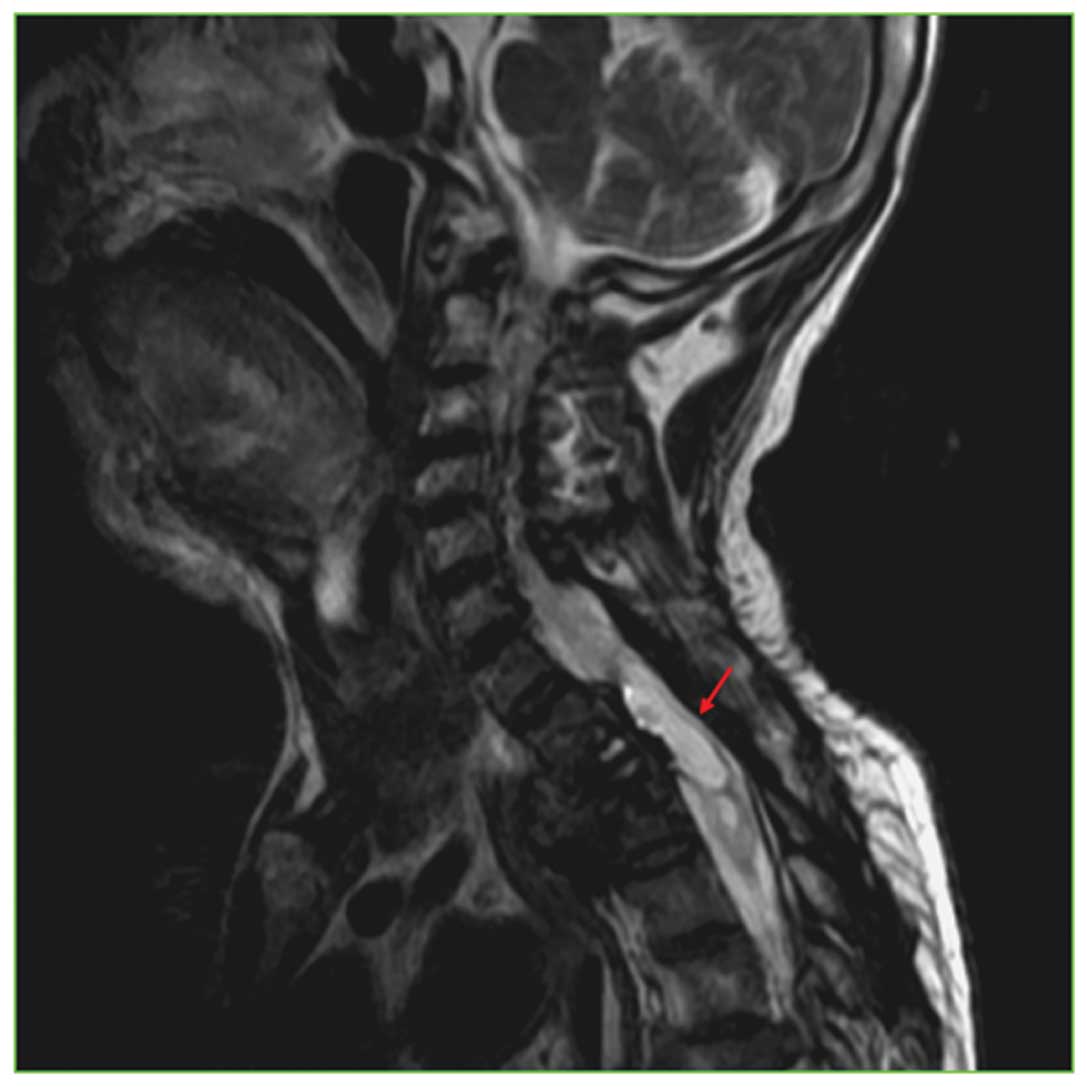
Accordingly, the patient was diagnosed with marked
hydrocephalus, possibly due to a lesion below the level of the
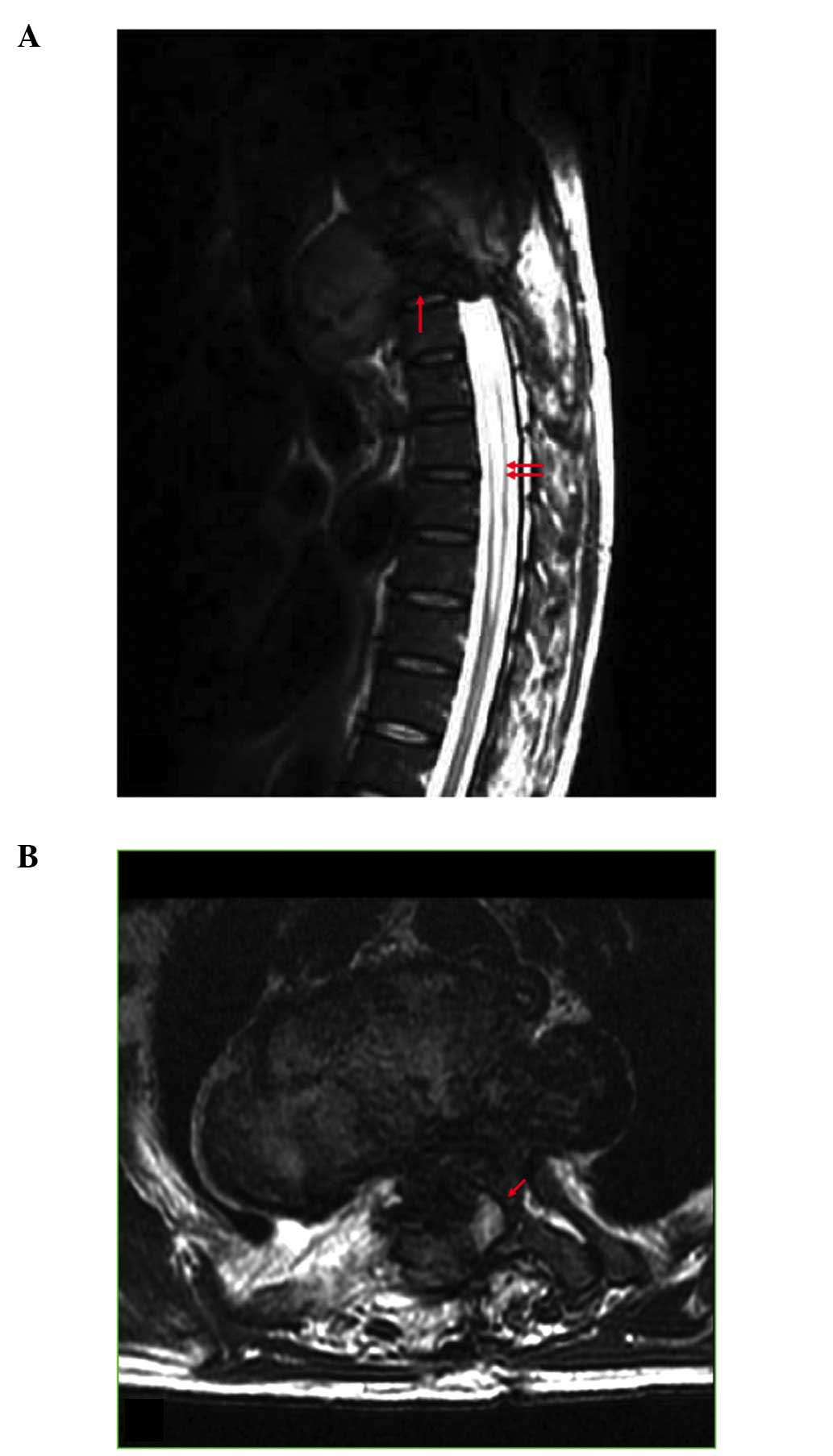
cervical spinal cord. In order to confirm this hypothesis, MR
imaging of the thoracic spine, with and without contrast
enhancement, was performed (Fig. 3A and
B). The study detected compression fractures at T2 and T3, and
indicated that the previously identified soft tissue lesion had
increased in size, extending from the anterior vertebral body
towards the spinal canal. In addition, the formation of
syringomyelia was observed.
Due to the progressive alteration in the spinal
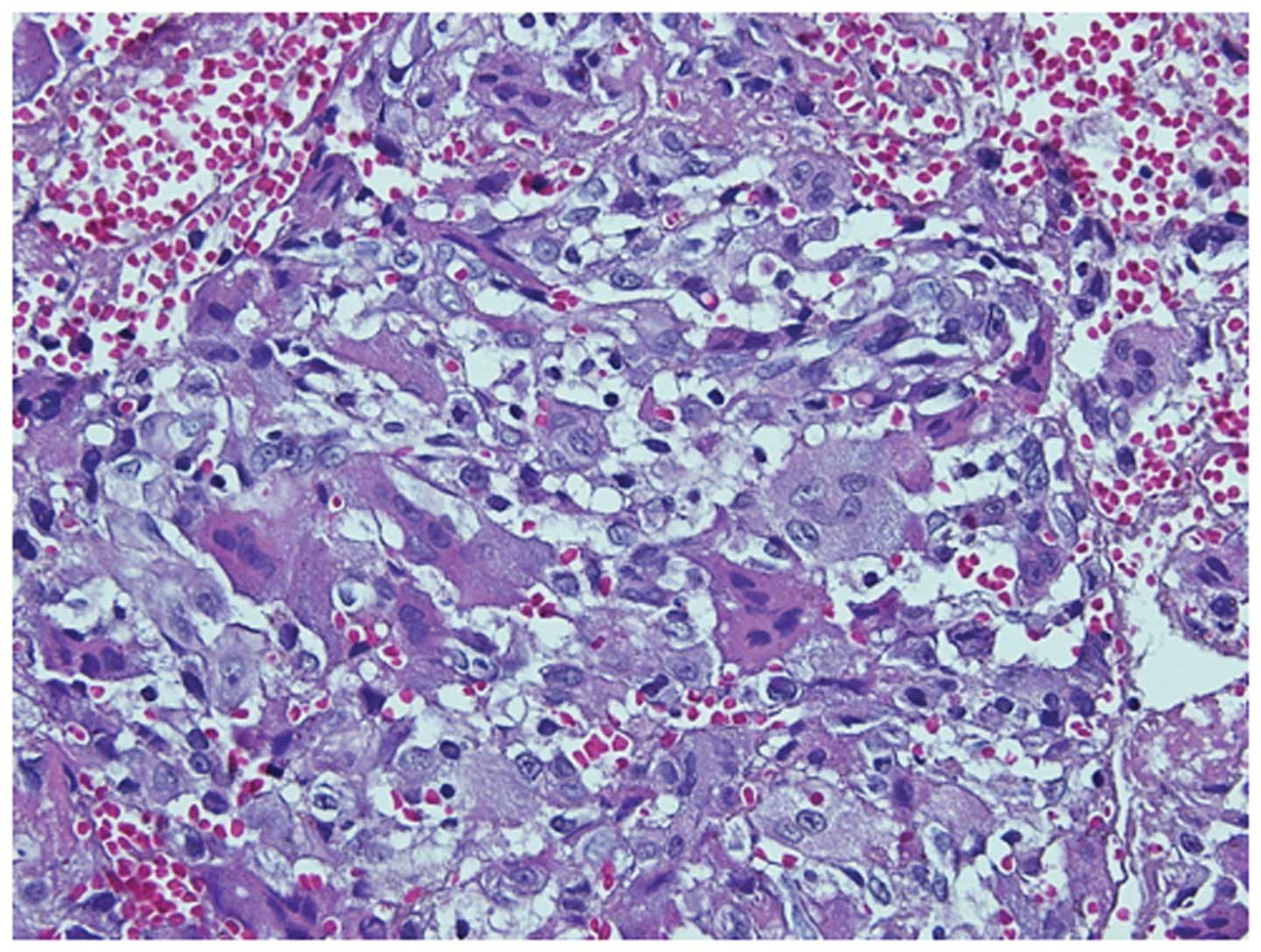
lesion, a CT-guided biopsy of the suspected thoracic spine tumor
was performed. Macroscopically, the tissue was a soft, brown mass;
microscopically, it was observed to contain numerous
osteoclast-like multinucleated giant cells (that were evenly
distributed) mixed with mononuclear ovoid stromal cells (Fig. 4). Neither cell type displayed nuclear
atypia or mitosis, and minimal hemosiderin and lymphocyte
infiltration were noted. Additionally, a small area of new bone
formation was observed at ×100 magnification. Immunohistochemical
staining revealed the giant cells to be strongly positive for CD68,
and the mononuclear cells to be focally positive for CD68 and
smooth muscle actin. No cells were observed to be positive for
cytokeratin or S-100. Histological and immunohistochemical studies
were consistent with GCT.
Consultation with a chest surgeon eliminated the
possibility of primary resection of the tumor due to the high
surgical risk, secondary to the size and location of the lesion.
Radiotherapy was suggested for management of the tumor, but the
family hesitated due to the high risk of radiation myelitis.
A ventriculoperitoneal shunting procedure was
performed to treat the hydrocephalus. CSF analysis was conducted
intraoperatively during the shunting procedure. Visually, the CSF
content appeared to have a clear color and non-viscous fluid flow.
Microscopic examinations, including routine cell counts and
biochemistry, were normal. No pleocytosis or high protein content
were observed in the CSF, indicating no evidence of an inflammatory
process.
Although the patient regained normal consciousness,
the paraplegia persisted. The patient and his family declined
further treatment due to religious beliefs; and the patient was
discharged in order to consult with a traditional healer. The
patient received a regular follow-up with MR examination of the
spine 30 months subsequent to the initial surgery. The results
demonstrated that the size of the tumor was stable (Fig. 5), which is compatible with the slow
growth characteristic of GCTs.
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Discussion
The majority of the spinal tumors reported in the
literature are of neural lineage, including neurofibromas (15), schwannomas (15), oligodendrogliomas (15), astrocytomas (16), ependymomas (17), gliomas (18) and mixed glioneuronal neoplasms
(19). GCTs are rare primary bone
tumors that comprise ~5% of all primary bone tumors (20). GCTs may occur in the vertebrae above
the sacrum and in the sacrum (2.9 vs. 2.5%, respectively) (21). Spinal lesions often involve the body
of the vertebra, and patients with GCTs of the spine usually
present with pain (22,23). A subset of these patients may also
report radiculopathic symptoms, varying degrees of myelopathy or
other neurological symptoms, due to the compression of the spinal
cord (1).
Diagnosis of GCTs of the spine may be challenging,
and relies on diagnostic imaging and histopathological examination
of tissue (24). When lesions occur
in the thoracic spine and extend into the paraspinal soft tissue,
they may be mistaken for a mediastinal mass (25). CT, MR imaging, scintigraphy and
positron emission tomography are all valuable tools for the
diagnosis of GCTs (25).
Histologically, GCTs typically appear as uniformly distributed
multinucleated giant cells against a background of round-to-spindle
shaped mononuclear stromal cells (1).
GCTs are typically slow growing, non-metastasizing
tumors, however, if left untreated after the initial onset of
symptoms, spinal GCTs have been reported to metastasize (26–28). Thus,
spinal GCTs are best treated promptly to avoid later metastasis or
hydrocephalus. Treatment strategies for spinal GCTs include
embolization, resection and radiation (1,27).
The association of hydrocephalus with mass lesions
affecting the spinal cord is unusual, but well-documented (25,29–31). To
the best of our knowledge, the present case is the sole example of
a non-neural spinal tumor associated with hydrocephalus, with the
exception of 1 case involving an intramedullary lipoma (28). In the reports of hydrocephalus
associated with neural tumors, hydrocephalus was usually the
initial finding, and the spinal tumors were detected secondarily,
often being identified by back pain that became evident following
the resolution of the hydrocephalus (15). By contrast, spinal GCTs, including the
present case, are initially detected due to sensory complaints and
neurological impairments associated with the compression of the
spinal cord (32). Thus,
hydrocephalus should be considered a potential complication of
spinal GCTs.
The majority of the explanations for the cause of
hydrocephalus focus on the commonly observed elevation of CSF
protein content, which may lead to occlusion of the arachnoid
granulations or to retardation of the CSF flow by increased
viscosity (29,31). This increased concentration of protein
has been attributed to tumor breakdown, hemorrhage and transudation
through abnormal tumor vessels (31).
Kudo et al (15) reviewed 67
cases of intraspinal tumors associated with hydrocephalus, and
concluded that hydrocephalus is likely due to elevated protein
content in the CSF, which decreases its absorption, and/or leads to
mechanical blocking of the pores whereby the CSF is absorbed by the
protein molecules. Schwartz et al (33) described a patient with severe
communicating hydrocephalus due to a lumbar myxopapillary
ependymoma. Kordás et al (34)
presented 3 cases of hydrocephalus associated with spinal tumors,
and postulated that the high protein content of the CSF resulted in
malabsorption.
Although protein elevation in the CSF may be a
possible cause for acute hydrocephalus with obstruction, this
hypothesis remains controversial. Cinalli et al (35) analyzed 38 case reports of
intramedullary low-grade glioma associated with hydrocephalus, and
concluded that while an increase in the protein content in the CSF
may be the cause of the hydrocephalus, the available evidence in
the literature was not sufficient to support this theory. An
alternative theory is that the hydrocephalus is caused by direct
obstruction of CSF outflow by the large tumor bulk (36). In the present case, this obstruction
occurred at the central canal of the spinal cord at the T2 level,
due to the tumor. Obstructive hydrocephalus is occasionally
observed with spinal tumors of neural origin, but is rarely
observed with non-neural tumors (15,31,36), such
as the present case.
In the present case, CSF analysis was performed
intraoperatively during the shunting procedure. Visually, the CSF
content appeared to have a clear color and non-viscous fluid flow.
Microscopic examinations of the CSF content, including routine cell
counts and biochemistry, were normal. No pleocytosis or high
protein content were observed in the CSF. Therefore ‘elevated CSF
protein’ should not be problematic with the shunt in the present
case report. However, postoperative long-term follow-up is required
for the observation of the shunt function.
Kordás et al (34) proposed that other causes of
hydrocephalus may include the presence of fibrinogen in the CSF,
which may arise from the following events: i) A chronic
inflammatory reaction; ii) loss of integrity of the blood-brain
barrier; iii) acute or chronic subarachnoid bleeding from the tumor
vessels; or iv) communication of the tumor and subarachnoid
pathways. The presence of fibrinogen in the CSF may lead to
deposition of fibrin and intracranial seeding of tumor cells that
may block the CSF flow.
Spinal cord tumors may cause syringomyelia, as
discussed by Lin et al (37)
in a review of idiopathic syringomyelia. Based on the data in the
present case, it was hypothesized that the hydrocephalus observed
in the patient was the result of the thoracic spine giant cell
tumor combined with syringomyelia. As the tumor increased in size,
syringomyelia developed, leading to direct CSF outflow obstruction
at the central canal of the cord. Management of symptoms includes
the resection of the obstructing tumor, if possible, and the use of
a shunt to reduce the intracranial pressure.
Characteristic symptoms of acute hydrocephalus
include altered mental status, nausea/vomiting, headache and
up-gaze palsy (Parinaud's syndrome) (38,39). The
diagnosis factors of acute hydrocephalus include a detailed history
of the patient, physical and neurological examination (such as the
level of consciousness and the cranial nerve function),
radiographic studies that may include brain CT and/or MRI, CSF flow
studies by cine-phase contrast MR imaging and CSF analysis
(14,40). Treatments for acute hydrocephalus
include medical therapy and surgical management (for example,
placement of a CSF shunt) (38,40,41).
Medical therapy is usually a temporary treatment strategy in
transient conditions where CSF shunting is not suitable, such as
central nervous system infections (38,40,41). The
use of medications as the final treatment for hydrocephalus is
controversial, since they do not appear to be effective in the
long-term treatment of chronic hydrocephalus (40,41). A CSF
shunt is the primary treatment for the majority of the etiologies
of hydrocephalus in the adult and pediatric populations, and a
ventriculoperitoneal shunt is the most commonly utilized procedure
among all the shunting methods (38,40,41). The
current case presented with a sudden onset of alteration in
consciousness, in which he was unable to follow simple commands,
due to acute hydrocephalus as a result of a thoracic GCT, as
confirmed by neuroimaging studies. A ventriculoperitoneal shunting
procedure was immediately performed to treat the hydrocephalus, and
the patient eventually regained normal consciousness, indicating
the marked effectiveness of CSF shunting in the acute hydrocephalus
in the current patient.
In summary, the present case report describes a
unique case of a GCT of the thoracic spine in a middle-aged male
that resulted in hydrocephalus. Diagnosis of GCTs may be
challenging, and relies on radiographic and histopathologic
findings. Although rare, acute hydrocephalus resulting from GCTs
should be considered in the differential diagnosis of
hydrocephalus.
References
|
1
|
Refai D, Dunn GP and Santiago P: Giant
cell tumor of the thoracic spine: Case report and review of the
literature. Surg Neurol. 71:228–233. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Si MJ, Wang CG, Wang CS, Du LJ, Ding XY,
Zhang WB, Lu Y and Zu JY: Giant cell tumours of the mobile spine:
Characteristic imaging features and differential diagnosis. Radiol
Med. 119:681–693. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kwon JW, Chung HW, Cho EY, Hong SH, Choi
SH, Yoon YC and Yi SK: MRI findings of giant cell tumors of the
spine. AJR Am J Roentgenol. 189:246–250. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Martin C and McCarthy EF: Giant cell tumor
of the sacrum and spine: Series of 23 cases and a review of the
literature. Iowa Orthop J. 30:69–75. 2010.PubMed/NCBI
|
|
5
|
Chakarun CJ, Forrester DM, Gottsegen CJ,
Patel DB, White EA and Matcuk GR Jr: Giant cell tumor of bone:
Review, mimics, and new developments in treatment. Radiographics.
33:197–211. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miller G, Bettelli G, Fabbri N and Capanna
R: Curettage of giant cell tumor of bone. Introduction-material and
methods. Chir Organi Mov. 75(Suppl): 2031990.PubMed/NCBI
|
|
7
|
Klenke FM, Wenger DE, Inwards CY, Rose PS
and Sim FH: Giant cell tumor of bone: Risk factors for recurrence.
Clin Orthop Relat Res. 469:591–599. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
van der Heijden L, Dijkstra PD, van de
Sande MA, Kroep JR, Nout RA, van Rijswijk CS, Bovée JV, Hogendoorn
PC and Gelderblom H: The clinical approach toward giant cell tumor
of bone. Oncologist. 19:550–561. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ruka W, Rutkowski P, Morysiński T, Nowecki
Z, Zdzienicki M, Makula D, Ptaszyński K, Bylina E and Grzesiakowska
U: The megavoltage radiation therapy in treatment of patients with
advanced or difficult giant cell tumors of bone. Int J Radiat Oncol
Biol Phys. 78:494–498. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mittal S, Goswami C, Kanoria N and
Bhattacharya A: Post-irradiation angiosarcoma of bone. J Cancer Res
Ther. 3:96–99. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tse LF, Wong KC, Kumta SM, Huang L, Chow
TC and Griffith JF: Bisphosphonates reduce local recurrence in
extremity giant cell tumor of bone: A case - control study. Bone.
42:68–73. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kaban LB, Troulis MJ, Ebb D, August M,
Hornicek FJ and Dodson TB: Antiangiogenic therapy with interferon
alpha for giant cell lesions of the jaws. J Oral Maxillofac Surg.
60:1103–1111. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dufresne A, Derbel O, Cassier P, Vaz G,
Decouvelaere AV and Blay JY: Giant-cell tumor of bone, anti-RANKL
therapy. Bonekey Rep. 1:1492012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Giiang LH, Chen CY, Chen MY, Huang TY and
Chung WH: Normal and abnormal cerebrospinal fluid dynamics
evaluated by optimized cine phase-contract MR imaging. Chin J
Radiol. 25:191–195. 2000.
|
|
15
|
Kudo H, Tamaki N, Kim S, Shirataki K and
Matsumoto S: Intraspinal tumors associated with hydrocephalus.
Neurosurgery. 21:726–731. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gelabert M, Bollar A, Paseiro MJ and Allut
AG: Hydrocephalus and intraspinal tumor in childhood. Childs Nerv
Syst. 6:110–112. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kesler A and Manor RS: Papilloedema and
hydrocephalus in spinal cord ependymoma. Br J Ophthalmol.
78:313–315. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Galarza M, Peretta P, Gazzeri R, Cinalli
G, Forni M, Morra I, Ragazzi P and Sandri S: Spinal cord gliomas
and hydrocephalus: Utility of neuroendoscopy. Minim Invasive
Neurosurg. 49:347–352. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Psarros TG, Swift D, Mulne AF and Burns
DK: Neurocytoma-like neoplasm of the thoracic spine in a
15-month-old child presenting with diffuse leptomeningeal
dissemination and communicating hydrocephalus. Case report. J
Neurosurg. 103(Suppl): 184–190. 2005.PubMed/NCBI
|
|
20
|
Murphey MD, Nomikos GC, Flemming DJ,
Gannon FH, Temple HT and Kransdorf MJ: From the archives of AFIP.
Imaging of giant cell tumor and giant cell reparative granuloma of
bone: Radiologic-pathologic correlation. Radiographics.
21:1283–1309. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Savini R, Gherlinzoni F, Morandi M, Neff
JR and Picci P: Surgical treatment of giant-cell tumor of the
spine. The experience at the Istituto Ortopedico Rizzoli. J Bone
Joint Surg Am. 65:1283–1289. 1983.PubMed/NCBI
|
|
22
|
Bhojraj SY, Nene A, Mohite S and Varma R:
Giant cell tumor of the spine: A review of 9 surgical interventions
in 6 cases. Indian J Orthop. 41:146–150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Biagini R, De Cristofaro R, Ruggieri P and
Boriani S: Giant-cell tumor of the spine. A case report. J Bone
Joint Surg Am. 72:1102–1107. 1990.PubMed/NCBI
|
|
24
|
Tokas ZO, Yilmaz B, Akakin A, Demir MK,
Yapicier O, Onat E, Urgen K and Konya D: Rare solitary primary
osseous lesions of the spine in adults; challenges in CT and MR
imaging diagnosis with pathological correlation. J Neurol Sci Turk.
32:275–283. 2015.
|
|
25
|
Sakurai H, Mitsuhashi N, Hayakawa K and
Niibe H: Giant cell tumor of the thoracic spine simulating
mediastinal neoplasm. AJNR Am J Neuroradiol. 20:1723–1726.
1999.PubMed/NCBI
|
|
26
|
Meyer A, Bastian L and Bruns F: Benign
giant cell tumor of the spine: An unusual indication for
radiotherapy. Arch Orthop Trauma Surg. 126:517–521. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ozaki T, Liljenqvist U, Halm H, Hillmann
A, Gosheger G and Winkelmann W: Giant cell tumor of the spine. Clin
Orthop Relat Res. 401:194–201. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Takahashi T, Katano S, Ishikawa H and
Nakano T: Aggressive clinical course of giant cell tumor arising
from thoracic vertebra after a long latent period. Radiat Med.
24:534–537. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ridsdale L and Moseley I: Thoracolumbar
intraspinal tumours presenting features of raised intracranial
pressure. J Neurol Neurosurg Psychiatry. 41:737–745. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Schijman E, Zúccaro G and Monges JA:
Spinal tumors and hydrocephalus. Childs Brain. 8:401–405.
1981.PubMed/NCBI
|
|
31
|
Zavala LM, Adler JR, Greene CS and Winston
KR: Hydrocephalus and intraspinal tumor. Neurosurgery. 22:751–754.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kim HS, Lee JE, Jung SS, Chon J, Yoon DH,
Park YK and Cho EH: Spinal cord injury due to the giant cell tumor
of the second thoracic vertebra: a case report. Ann Rehabil Med.
37:269–273. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Schwartz NE, Rosenberg S and So YT: Action
at a distance: A lumbar spine tumor presenting as trigeminal
neuralgia. Clin Neurol Neurosurg. 108:806–808. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kordás M, Czirják S and Dóczi T: The
spinal tumour related hydrocephalus. Acta Neurochir (Wien).
139:1049–1054. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cinalli G, Sainte-Rose C, Lellouch-Tubiana
A, Sebag G, Renier D and Pierre-Kahn A: Hydrocephalus associated
with intramedullary low-grade glioma. Illustrative cases and review
of the literature. J Neurosurg. 83:480–485. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sun H and Tian H: Intraspinal tumors
accompanied by hydrocephalus: Case report, systematic review, and
discussion of treatment strategy. Neurologist. 17:342–345. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lin JW, Lin MS, Lin CM, Tseng CH, Tsai SH,
Kan IH and Chiu WT: Idiopathic syringomyelia: Case report and
review of the literature. Acta Neurochir Suppl (Wien). 99:117–120.
2006. View Article : Google Scholar
|
|
38
|
Lee TT, Uribe J, Ragheb J, Morrison G and
Jagid JR: Unique clinical presentation of pediatric shunt
malfunction. Pediatr Neurosurg. 30:122–126. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Koga H, Mori K, Kawano T, Tsutsumi K and
Jinnouchi T: Parinaud's syndrome in hydrocephalus due to a basilar
artery aneurysm. Surg Neurol. 19:548–553. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hamilton MG: Treatment of hydrocephalus in
adults. Semin Pediatr Neurol. 16:34–41. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Bergsneider M, Miller C, Vespa PM and Hu
X: Surgical management of adult hydrocephalus. Neurosurgery.
62(Suppl 2): 643–659, discussion 659–660. 2008.PubMed/NCBI
|