Introduction
Prostatic cancer (PCa) is currently being viewed as
one of the most significant health problems experienced by the male
population. PCa is the most frequently occurring solid neoplasm in
men in Europe. With an incidence rate of 214 cases per 1,000
individuals, PCa cases outnumber lung and colorectal cancer cases.
PCa accounts for 11% of all male cancers and 9% of
cancer-associated mortalities, meaning that it ranks second in the
cause of cancer-associated mortalities (1,2). The
standard reference for the detection of PCa is the digital rectal
examination (DRE). The common histology for PCa is adenocarcinoma.
In 2005, the International Society of Urological Pathology (ISUP)
determined applicable criteria for the Gleason score in the
classification of PCa through core biopsy and surgical specimens
for diagnosis of PCa. Ranging between 2 and 10, with a score of 2
being the least aggressive and 10 being the most aggressive, the
Gleason score is calculated as the sum of the two most typical
patterns (grades 1–5) of tumor growth observed. Furthermore, any
pattern forming the score should be present at a rate of at least
5% in order to score the tumor specimen (3). The factors determining the risk of the
development of clinical PCa are not known exactly. The clearest
risk factor appears to be inheritance (4). The rate of autopsy-detected PCa is
almost the same all over the world (4). Besides genetic risk factor, it is
believed that external factors are also effective in the
progression of latent PCa to clinical PCa and that they may be
among the risk factors. These external factors are considered to
include foods, sexual behavior patterns, consumption of alcohol,
ultraviolet light exposure and chronic inflammation, and are
believed to be significant in the disease etiology (5). The mortality trends of PCa differ widely
between countries in the industrialized World (6). There is no evidence to suggest that
prostate-specific antigen (PSA) screening reduces disease-specific
mortality, although the disease-specific mortality rate has
decreased (7). The age limit
recommended for the first PSA screening is 40 years old.
Re-screening is not recommended for 8 years if the PSA value
detected in the first screening is <1 ng/ml. Furthermore, PSA
screening is not recommended after the age of 75, as it has no
clinical efficiency after that age (8). PSA is a serine protease of the
kallikrein group, and is produced only by prostatic epithelial
cells. PSA is organ-specific, but not disease-specific. A diagnosis
of PCa is made in 34% of patients with PSA values ranging between 3
and 6 ng/ml in their 7-year cumulative follow-up, while this value
has been found to be 44 and 71% for those individuals with PSA
values of 6–10 ng/ml and >10 ng/ml, respectively. The disease is
diagnosed by transrectal ultrasound (US)-guided biopsy and staged
by DRE, PSA and bone scanning. The role of magnetic resonance
imaging (MRI) and computed tomography (CT) in staging is
controversial. The diagnostic tool of choice for the locally
advanced stage of PCa is MRI (9). Men
with localized PCa are treated with curative intent, however, a
number will eventually develop biochemical recurrence and disease
metastasis (10).
There is axial bone metastases in 85% of patients
who succumb to PCa. Bone scanning is used for detection of patients
with bone metastases, but its false-positive rate is high. Bone
metastases are very common in PCa, with th majority being sclerotic
in nature. Lytic bone metastases are extremely rare in PCa.
18F-fluorodeoxyglucose (18F-FDG) positron
emission tomography (PET)/CT has low sensitivity in the detection
of the sclerotic metastatic lesions of PCa. However, in the
detection of lytic PCa metastasis, 18F-FDG PET/CT is
useful (11). 18F- or
11C-choline, 18F- or 11C-acetate,
the synthetic L-leucine analog
anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid,
16β-18F-fluoro-5α-dihydrotestosterone targeted to the
androgen receptor, and prostate-specific membrane antigen-based PET
radiotracers are used for detecting PSA elevations following
definitive treatment of metastatic PCa and hormone-refractory
disease (12,13). An accumulation of evidence currently
strongly suggests that 18F-FDG PET/CT may aid in the
evaluation of imaging for men with metastatic PCa (14).
The main objective of the present study was to
determine the role of 18F-FDG PET/CT in the re-staging
of patients who received external beam radiation therapy (EBRT) or
underwent radical prostatectomy (RP) for local-stage PCa (T1c,
T2a-b or T3) with PSA relapse. Conventional methods are
insufficient, as bone scanning has a high false-positivity rate in
detecting the location of the metastases and bone metastases.
18F-FDG PET/CT may be useful due to the high sensitivity
in the lytic bone lesions, the association of the biochemical
recurrence with clinical disease and the possibility of early
diagnosis. This increases the importance of 18F-FDG
PET/CT in the verification of PSA relapse. Histology of the lesions
(if available), or the clinical, laboratory and radiological
investigations (PSA, bone scanning and MRI) were all used as
reference standards.
Patients and methods
Patients
A total of 7,938 patients were assessed in the
Department of Nuclear Medicine, School of Medicine, Sifa University
(Izmir, Turkey) between July 2007 and April 2013, and a total of
10,553 18F-FDG PET/CT investigations were performed.
From these patients, 28 who received RP or EBRT as definitive
treatment for the diagnosis of local-stage prostatic adenocarcinoma
were included in the present study. In this group of patients,
18F-FDG PET/CT was performed for re-staging upon
development of PSA relapse following RP in 23 (82.1%) patients and
following definitive EBRT in 5 (17.9%).
The mean age of the patients was 65.07 years and the
standard deviation was 7.51 years (range, 51–82 years). The
patients were in stages T1c, T2 and T3, defined as local stages
according to the European Association of Urology's prostate cancer
classification system (15). Based on
Gleason's prostatic adenocarcinoma scoring system of the European
Association of Urology and the ISUP (3), the Gleason score was <7 in 17 (60.7%)
patients and ≥7 in 11 patients (39.3%). All patients underwent
18F-FDG PET/CT scanning for re-staging due to the
suspicion of disease recurrence or biochemical recurrence during
routine follow-ups. These patients were reviewed retrospectively
and their pathology and 18F-FDG PET/CT results were
recorded. Exclusion criteria included a history of any cancer other
than PCa, active infection, active inflammatory conditions, poorly
controlled diabetes mellitus, a recent or complicated non-healing
fracture, and hip or knee arthroplasty.
Definition of PSA relapse
Treatment-specific definitions of PSA relapse by the
American Urological Association and the American Society for
Therapeutic Radiology and Oncology consensus were applied in those
patients who had undergone either RP or EBRT, respectively. The
definition by the American Urological Association classifies
biochemical failure as an initial serum PSA level of ≥0.2 ng/ml,
followed by a second confirmed rise in PSA (16). The definition by the American Society
for Therapeutic Radiology and Oncology classifies biochemical
failure as a rise in PSA level by ≥2 ng/ml above the nadir.
Imaging and interpretation of
data
18F-FDG PET/CT scans were obtained after
at least 6 h of fasting and when the blood glucose level was
<150 mg/dl. Combined FDG PET/CT was performed using a Siemens
HI-REZ biograph 6 (Siemens AG, Munich, Germany), which provides an
in-plane spatial resolution of 4.8 mm, an axial field view of 16.2
cm and three-dimensional image acquisition. Prior to scanning, 6 h
of fasting was required. At ~1 h after the intravenous injection of
555 MBq 18F-FDG, a whole-body PET scan from the skull
base to the upper thighs was performed. The whole-body CT scan was
performed in the craniocaudal direction, without intravenous
contrast. Immediately after this, PET data were collected in the
craniocaudal direction with the arms down. FDG PET images were
reconstructed using CT data for attenuation correction.
A visual analysis of the PET scans and a
semi-quantitative analysis using the maximum standard uptake value
(SUVmax) were performed. The SUV was expressed in terms
of body weight (g/ml). All recorded parameters, including the
patient's weight (kg), height (cm), radioactivity during injection
(MBq), injection start time, residual radioactivity (MBq)
post-injection and radioisotope half-life (used as the standard
109.8 min for 18F-FDG), were automatically calculated by
the software.
Two physicians who were experienced in nuclear
medicine and were blinded to the study independently reviewed the
hybrid 18F-FDG PET/CT scans and decided upon a positive
or negative result for a primary tumor site. Each area of focal
tracer uptake deviating from the normal physiological distribution
was indicative of the disease. Background deviations and activity
differences in the tissues surrounding the suspicious lesion were
used to discriminate the benign lesions from the malignant lesions.
For the patients receiving EBRT, an SUV value of 5.8 in the
prostate was taken as the reference. The patients with an SUV value
of >5.8 were considered as positive. No specific SUV value was
used for the patients undergoing RP.
Statistical analysis
All statistical data analyses were calculated using
SPSS statistics software (version 16.0; SPSS, Inc., Chicago, IL,
USA). All statistical data analyses were calculated using Fisher's
Exact test. P<0.05 was considered to indicate a statistically
significant difference.
Ethics
All procedures followed were in accordance with the
ethical standards of the responsible Committee on Human
Experimentation and with the Helsinki Declaration of 1975, as
revised in 2000.
Results
18F-FDG PET/CT imaging was negative in 16
(57.1%) patients and positive in 12 (42.9%). Local recurrence and
bone metastases were found in 2 (7.1%) patients, bone metastases
only in 7 (25.0%) patients (mean SUVmax, 9.8), local
recurrence only in 1 (3.6%) patient, local recurrence and bone or
lymph node metastasis in 1 (3.6%) patient, and recurrence in the
prostate in 1 (3.6%) patient. The last patient had received
definitive EBRT and the SUVmax value was 21.8. The
patients were divided in two groups based on their Gleason scores
of <7 or ≥7. The 18F-FDG PET/CT results of the
patients with Gleason scores of <7 and ≥7 are shown in Table I. Patients with Gleason scores of
>7 on PET/CT exhibit increased visualization. Increased
visualization may be a result of increased glucose metabolism,
which is associated with cancer tissues. A total of 4 (14.3%) and 7
(28.6%) patients with Gleason scores of <7 and ≥7, respectively,
were positive on PET/CT.
 | Table I.PET/CT results by Gleason score of
the primary tumor. |
Table I.
PET/CT results by Gleason score of
the primary tumor.
| Gleason score | Positive on PET/CT,
n (%) | Negative on PET/CT,
n (%) |
|---|
| <7 | 4 (14.3) | 13 (46.4) |
| ≥7 | 8 (28.6) | 3
(10.7) |
18F-FDG PET/CT results correlated with
histological subtype in probability charts (P=0.0189). The
sensitivity, specificity, positive predictive value, negative
predictive value and accuracy of 18F-FDG PET/CT were
61.6%, 75.0%, 61.6%, 75.0% and 71.4%, respectively.
Discussion
Definitive therapeutic modalities of local-stage PCa
have been standardized as RP and EBRT, and the strategy to follow
patients treated with RP or EBRT is based on PSA relapse. PSA
relapse does not always mean clinical recurrence, as the condition
may occasionally be diagnosed as biochemical relapse and the
disease will not manifest. Thus, correctly diagnosing patients and
monitoring their response to the treatment is of vital importance
(16).
Re-staging of the disease, minimizing the
false-positive and false-negative results, and diagnosing the local
recurrences and metastatic disease are the most important and most
realistic focuses of the entire therapeutic strategy (16). For the patients with PSA relapse, it
is not always possible to know the anatomical location and volume
of the disease, further increasing the importance of anatomical and
functional imaging. PET is an ideal non-invasive tool for imaging
of the underlying tumor biology. 18F-FDG PET/CT is one
of the most important diagnostic tools in which particularly
anatomical and functional images are processed. PSA relapse,
transrectal US-guided re-biopsy, contrast-enhanced CT, MRI, bone
scanning and 18F-FDG PET/CT may be used to detect
metastatic disease following RP or EBRT, and to monitor the
response to treatment (16).
PSA is an independent prognostic factor in the early
diagnosis of PCa, and in determining recurrences and metastases.
Locally recurrent cancer is ultimately detected in 25–35% of men
with biochemical failure, while metastatic disease is only found in
20-25%, and local recurrence and metastatic disease together is
detected in 45–55% (17). When
18F- and 11C-choline were used in patients
with PCa with biochemical recurrences in the screening series of
patients of European and Japanese origin, a sensitivity ranging
between 38 and 98% was found in the detection of local recurrences
and metastatic disease.
One of the most significant features of cancer is
that the metabolic utilization of glucose in higher in the cancer
compared to the normal tissues (Warburg's effect) (18). PET imaging with 18F-FDG, an
analog of glucose, tracks the glucose metabolism of tissues. The
use of 18F-FDG PET is therefore fundamental to oncology
studies (19). Elevated glucose
metabolism in malignant tissues due to increased of cellular
membrane glucose transporter (GLUT) expression, mainly GLUT-1, and
enhanced hexokinase (HK-II) enzymatic activity in tumors, is the
basis of cancer detection by 18F-FDG PET (20). The uptake of 18F-FDG in PCa
is dependent on the differentiation of the tumor, with low uptake
found in well-differentiated tumors and high uptake found in
aggressive poorly-differentiated tumors (14). Patients with advanced disease may be
evaluated by 18F-FDG PET/CT through the detection of
active osseous and soft-tissue metastases. The technique may also
be useful for evaluating the hormonal treatment response (16). In an evaluation of the mRNA expression
of GLUT1 in hormone-dependent and hormone-independent tissues of
PCa, Effert et al found that the hormone-resistant cells
with poor prognosis exhibited a much higher level of GLUT1 compared
with the well-differentiated hormone-sensitive cells (21). Considering these findings as the basic
principle for the use of 18F-FDG PET in PCa, there are
other studies in the literature supporting these results. The most
important factor in commenting on the activity of FDG in PCa is
that the tissue of benign prostatic hyperplasia (BPH) has also
measurable FDG activity. Stewart et al (22), however, found that the gene expression
of GLUT1 was higher in PCa than in BPH. Kukuk et al
(23) demonstrated that there was a
large amount of FDG accumulation in the xenograft mouse models of
hormone-resistant PCa, and that this FDG activity decreased
following androgen ablation. Primarily staging PCa with
18F-FDG PET is quite difficult due to the physiological
urinary activity of FDG. False-positive FDG activity in the
residual urine, and in the bladder and urethra due to the
anatomical neighborhood of these anatomical structures limits the
value of this method. Additionally, the false-positive FDG activity
of the normal prostatic tissues and BPH also limits the procedure;
it also fails in distinguishing low-volume foci of PCa. Thus,
18F-FDG PET/CT has a limited role in the primary staging
of PCa. Nonetheless, FDG-PET application has not yet been full
developed for PCa (24).
A recent study from Japan used a time-of-flight
PET/CT scanner to assess for the visual identification of primary
PCa with FDG (25). For the
differentiation between biopsy specimens with a summed Gleason
score of ≤5 and those specimens with a summed Gleason score of ≤6,
the cut-off SUVmax, sensitivity and specificity were
2.8, 61.7 and 80%, respectively. In a study by Minamimoto et
al (26), patients with Gleason
scores of ≥7 exhibited sensitivity and positive predictive values
of 80 and 87%, respectively (26).
18F-FDG PET/CT may be useful in the imaging evaluation
of men with biochemical failure following definitive therapy for
primary PCa. The main objective of the present study was to assess
the efficiency of 18F-FDG PET/CT in re-staging following
definitive treatment.
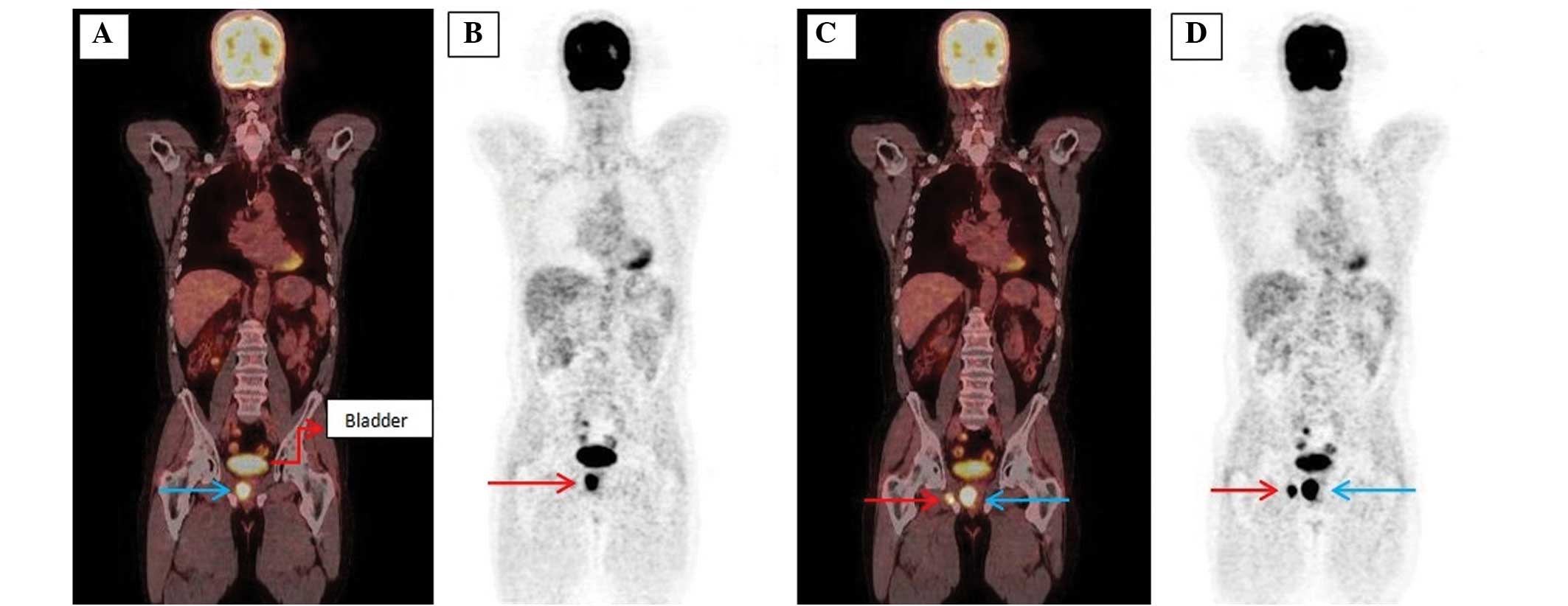
The present study showed that this method was able
to detect biochemical recurrence and recurrence at the prostatic
location despite its anatomical and physiological disadvantages
(Fig. 1). However, we believe that
this was due to the high SUVmax value (21.8). The fact
that the Gleason score was >7 and the PSA value was 28 ng/ml may
have increased the visualization due to the high activity of
glucose metabolism. The detection of recurrence in the prostate
remains a big problem for 18F-FDG PET/CT in cases of
low-volume disease, relapses with low PSA levels and Gleason scores
of <6.
In a study by Schöder et al (27) on 91 men with PSA relapse following
prostatectomy, the mean PSA levels were higher in the FDG
PET-positive patients than in the FDG PET-negative patients
(9.5±2.2 ng/ml vs. 2.1±3.3 ng/ml). In the study, either local
recurrence or systemic metastases were found in 31% of the patients
undergoing FDG-PET due to PSA recurrence. In another study on 24
patients with verification of the pelvic lymph nodes, Chang et
al (28) found a sensitivity,
specificity, positive predictive value and negative predictive
value of 75, 100, 100 and 67.7%, respectively. In the study, it was
demonstrated that FDG-PET could detect metastatic disease in ~31%
of the patients with PSA recurrence following RP. It was stated
that the technique would be more useful when it was used in
patients with a PSA level of >2.4 ng/ml or a PSA doubling time
of >1.3 ng/ml/year, but that this had to be supported by
prospective studies. Jadvar et al found that the method gave
usable data in a study which evaluated 18F-NaF and
18F-FDG PET/CT for the detection of occult metastases in
patients with the biochemical recurrence of PCa (14). The study consisted of 37 patients (26
undergoing RP and 11 receiving EBRT). A sensitivity, specificity,
positive predictive value, negative predictive value and accuracy
rate of 50, 82, 64, 73 and 70%, respectively, were found. Combined
imaging using simultaneous 18F-FDG and
18F-NaF injection has also been reported. However, there
is currently a lack of evidence to support its use in routine
clinical practice.
In the current study, a sensitivity and positive
predictive value of 61%, a specificity and negative predictive
value of 75%, and an accuracy of 71% were found, all being
consistent with the values reported in the literature. Within the
limitations of the present observational study, these data indicate
that PET/CT may be useful for the process of making clinical
decisions. PET and PET/CT studies from the literature are
summarized in the Table II.
| Table II.Diagnostic performance of PET and
PET/CT studies in the literature. |
Table II.
Diagnostic performance of PET and
PET/CT studies in the literature.
| First author
(ref.) | Modality | n | Sensitivity, % | Specifity, % | PPV, % | NPV, % | Accurary, % |
|---|
| Chang et al
(28) | FDG-PET | 24 | 75 | 100 | 100 | 68 | – |
| Schöder et
al (27) | FDG-PET | 91 |
|
|
|
|
|
|
|
PSA>2.4a |
| 80 | 73 | – | – | – |
|
|
PSA-DT>1.3b |
| 71 | 77 | – | – | – |
| Jadvar et al
(29) | FDG-PET/CT | 37 | 50 | 82 | 64 | 73 | 70 |
| Present study | FDG-PET/CT | 28 | 61 | 75 | 61 | 75 | 71 |
18F-FDG PET/CT may be particularly useful
in the treatment response evaluation of metastatic PCa. FDG
accumulation at metastatic sites tends to decrease with successful
chemohormonal therapy (29). There
may be differences in imaging-based assessment using various
response criteria [e.g., Response Evaluation Criteria in Solid
Tumors (RECIST) (30), European
Organization for Research and Treatment of Cancer, PET Response
Criteria in Solid Tumors and National Oncology PET Registry
(31)] and the PSA-based response
criteria (32). Hwang et al
(33) performed an analysis of
18F-FDG PET/CT images in 12,037 subjects who showed
abnormal hypermetabolism in the prostate. While 120 patients
exhibited abnormal 18F-FDG PET/CT signaling, 38 of these
subsequently underwent investigation by prostate biopsy as a result
of an abnormal total PSA serum level and/or the clinical suspicion
of cancer upon DRE. Minamimoto et al (34) found positive results indicating the
possibility of cancer in 16,955 cases (10.9%). Although only 1,912
cancers were actually detected, PCa was found in 165 patients, with
a FDG-PET sensitivity of 37.0%. From this it may be concluded that
altered PSA levels may be exhibited in approximately one-third of
PCa patients with positive FDG-PET findings. Confounding factors
for a decreased PSA level in patients with PCa may include the
concomitant use of medical therapies, such as statins,
non-steroidal anti-inflammatory drugs and hormones, and/or a higher
body mass index (BMI). In the current study, the BMIs of the
patients were not known. So, no comparison was made with the
literature on this basis. In the study by Wright et al
(35), obese males exhibited lower
age-adjusted PSA levels compared with those of normal weight.
Koochekpour et al (36) also
recently demonstrated a possible characterization of PCa cells in
association with their metabolism. Glutamate receptor 1 antagonists
may alter the metabolism of aggressive cancers, with the subsequent
development of the Warburg effect in cases where hypoxia is induced
by the tumor. In the study, a significant difference was found in
the serum levels of glutamate between the patients with a Gleason
score of <7 and those with a score of >8. In the future, an
increased and altered glutamate metabolism is being considered as a
biological marker for patients with a Gleason score >8, i.e.,
for those with aggressive PCa. In aggressive PCa, increased
glutamate metabolism increases the rate of positive subjects and
also affects sensitivity due to increased FDG-PET activity
(36). A strong correlation exists
between the Warburg effect and the mitochondrial metabolism of the
tumor cells, even in the patients with normal PSA values,
suggesting that 18F-FDG PET/CT may be used in such
patients (37).
Bone metastasis is a potential consequence of
progressive PCa. Accurate detection of the bone metastases through
imaging-based analysis is absolutely required for effective
treatment. Moreover, even though novel bone-targeted therapies are
being developed, the current standard diagnostic imaging
techniques, including 99mTc-based bone scintigraphy and
CT, are not adequate for the accurate measurement of tumor burden.
One study has reported an attempt to semi-quantitatively measure
bone metastases on 99mTc-based bone scintigraphy (bone
scan index). However, the fundamental limitations of bone
scintigraphy, including indirect imaging of tumor presence, low
specificity (false-positives with benign conditions), and low
sensitivity (gross underestimation of the true prevalence of bone
metastases), are restrictive, and this technique has not been
widely used (38). When considering
the inclination of PCa to metastasize to the bones and the
limitations of current imaging tools for assessing these bone
metastases, the quantitative evaluation a response has proved
difficult. Obstacles include the inability to use response
criteria, such as RECIST, for bone metastasis assessment by CT, the
confounding effect of the flare phenomenon on standard bone
scintigraphy, and the ambiguity associated with the clinical
significance of serum PSA level changes (39,40).
18F-FDG PET/CT will be particularly useful in PCa
patients with lytic skeletal metastasis (11). Although bone metastases are extremely
common in PCa, lytic metastases are rare. This type of metastasis
probably results from the overproduction of parathyroid
hormone-related peptide by PCa cells in vivo (41). 18F-FDG PET is less
sensitive than bone scanning for defining sclerotic bone
metastases. By contrast, 18F-FDG PET-CT is superior to
bone scintigraphy for the detection of lytic PCa metastases. In the
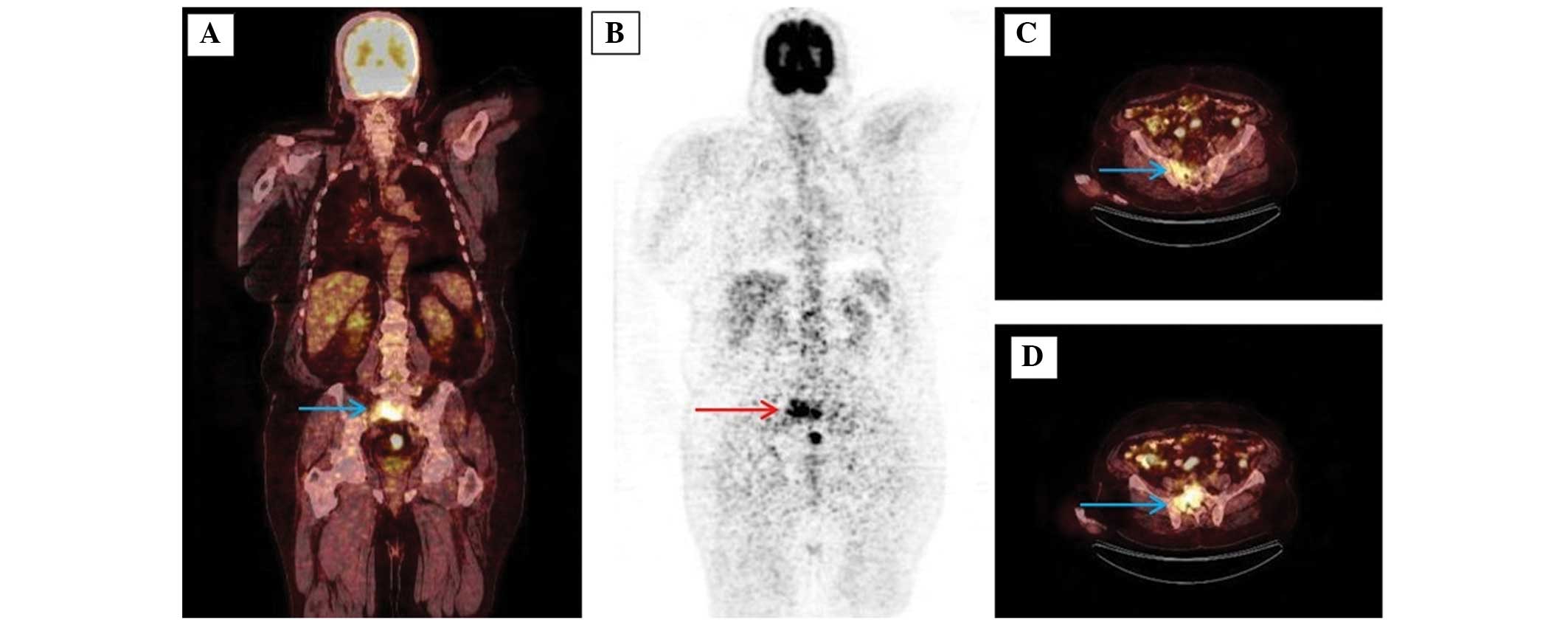
present study, osteoblastic bone metastases could be detected by
18F-FDG PET-CT. We believe that this apparent activity
could be detected due to an increased Warburg's effect as a result
of a high level of PSA, a high tumor volume and a high Gleason
score creating a high SUV on the detector (Fig. 2).
Other studies have also shown a potential prognostic
utility for FDG PET, with generally higher tumor SUVs indicating a
poorer prognosis than lower SUVs, which is similar to the general
experience with other cancer types (42). The prognostic utility of bone
scintigraphy and 18F-FDG PET was analyzed in a study by
Meirelles et al (43), which
evaluated 39 patients with castration-resistant disease and 12
patients that did not require medical or surgical castration. These
patients were followed up for a minimum of 5 years or until they
succumbed. The SUVmax of the most active bone lesion was
used as the outcome measure for the 18F-FDG PET studies.
An inverse association was determined between bone scan index and
SUVmax. The median survival time of 32.8 months for an
SUVmax of <6.10 was significantly longer than the
14.4 months for an SUVmax of >6.10. Moreover, upon
multivariate analysis, the SUVmax was found to be an
independent prognostic factor (41).
In the present study, bone metastases were found in 25.0% (n=7) of
the patients. The mean SUVmax of these metastases was
9.8, but no statistical correlation was made as the survival data
were inadequate. The 18F-FDG uptake in PCa cells is
modulated by androgens (44). The
benefits of 18F-FDG PET/CT in monitoring the response to
anti-androgen treatment remains controversial. The technique is,
however, usually useful in distinguishing the healed lesions from
the active metastases (45). It has
been demonstrated that PET/CT with 18F-FDG may aid in
the direct imaging of metastatic PCa (13). Recently, a study by Jadvar et
al indicated the utilization of 18F-FDG PET/CT in
castration-resistant metastatic PCa. In the series of 87 patients,
a negative correlation was found between the SUV value and
disease-specific survival. 18F-FDG PET/CT is a useful
imaging biomarker for the prediction of overall survival in men
with castration-resistant metastatic PCa (46).
The metabolic rate of PCa with a low Gleason score
is similar to that of normal tissues. The increased glucose
metabolism in PCa patients with a high PSA level and a high Gleason
score allows visualization of the lesions due to an increase in FDG
uptake.
False-positive or false-negative FDG uptake results
cannot be explained solely by the glucose metabolism of tumor
tissue. Studies have demonstrated that 18F-FDG PET/CT
scans can provide information only in the presence of a certain
increased number of tumor cells with abnormal glucose metabolism
(104-107 cells). Such diagnostic failures are
particularly significant in metastases of solid organs, such as the
lungs and liver. Generally, 18F-FDG PET/CT is unable to
accurately evaluate metastases that are <5 mm in diameter. It is
not known why high SUVs are not produced in lung lesions below this
threshold. Inaccurate evaluation can be caused by motion artifacts
and the low metabolic activity of metastatic lesions. Certain
techniques can result in a reduction of motion artifacts, which
achieves better spatial resolution and determines higher cut-off
SUV values for such lesions, thus increasing the accuracy of the
diagnostic process (47).
It is essential that the PET/CT findings be verified
by histopathological work-up so that disease recurrence can be
confirmed. Theoretically, this technique remains the gold standard.
Unfortunately, in daily practice, clinical reasons, procedure
feasibility and the effective advantages of this approach in the
absence of radical surgical intent mean that this is seldom
possible. In the present study, confirmation by histological
examination was possible in 9 patients, while all others were
compared using clinical plus radiological findings.
The main limitation of the present study is its
retrospective nature. A certain amount of selection bias may have
been present, as it is likely that only those PCa patients with
metastatic disease in biochemical recurrence who were suspected to
have recurrence were referred for PET/CT.
In the current study, the contribution of
18F-FDG PET/CT in detecting local recurrences and
metastases in the patients with biochemical recurrence following RP
or EBRT treatment for the diagnosis of local-stage PCa was reviewed
retrospectively and found to be consistent with the literature
findings. A possible limitation of the study was the lack of
histological verification for the lesions in view of constraints
imposed by practical, economic and ethical issues. It may be
indicated that 18F-FDG PET/CT would be useful in
diagnosing biochemical recurrence with a high accuracy (70%) in
patients with PCa.
References
|
1
|
Boyle P and Ferlay J: Cancer incidence and
mortality in Europe 2004. Ann Oncol. 16:481–488. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J,
Murray T and Thun MJ: Cancer statistics, 2008. CA Cancer J Clin.
58:71–96. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Epstein JI, Allsbrook WC Jr, Amin MB and
Egevad LL: ISUP grading committee. The 2005 International Society
of Urologic Pathology (ISUP) consensus conference on Gleason
grading of prostatic carcinoma. Am J Surg Pathol. 29:1228–1242.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hemminki K: Familial risk and familial
survival in prostate cancer. World J Urol. 30:143–148. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Leitzmann MF and Rohrmann S: Risk factors
for the onset of prostatic cancer: Age, location and behavioral
correlates. Clin Epidemiol. 4:1–11. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Oliver SE, May MT and Gunnell D:
International trends in prostate-cancer mortality in the ‘PSA-ERA’.
Int J Cancer. 92:893–898. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ilic D, O'Connor D, Green S and Wilt T:
Screening for prostate cancer: A Cochrane systematic review. Cancer
Causes Control. 18:279–285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Roobol MJ, Roobol DW and Schröder FH: Is
additional testing necessary in men with prostate-specific antigen
levels of 1.0 ng/ml or less in a population-based screening
setting? (ERSPC, section Rotterdam). Urology. 65:343–346. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Heenan SD: Magnetic resonance imaging in
prostate cancer. Prostate Cancer Prostatic Dis. 7:282–288. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Scher HI, Halabi S, Tannock I, et al:
Design and end points of clinical trials for patients with
progressive prostate cancer and castrate levels of testosterone:
Recommendations of the Prostate Cancer Clinical Trials Working
Group. J Clin Oncol. 26:1148–1159. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sharma P, Karunanithi S, Singh Dhull V, et
al: Prostate cancer with lytic bone metastases:
18F-fluorodeoxyglucose positron emission tomography-computed
tomography for diagnosis and monitoring response to medical
castration therapy. Indian J Nucl Med. 28:178–179. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Apolo AB, Pandit-Taskar N and Morris MJ:
Novel tracers and their development for the imaging of metastatic
prostate cancer. J Nucl Med. 49:2031–2041. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jadvar H: Molecular imaging of prostate
cancer: PET radiotracers. AJR Am J Roentgenol. 199:278–291. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jadvar H: Molecular imaging of prostate
cancer with 18F-fluorodeoxyglucose PET. Nat Rev Urol. 6:317–323.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
European Association of Urology.
Guidelines on Prostate Cancer. http://uroweb.org/wp-content/uploads/09-Prostate-Cancer_LR.pdfAccessed.
June 15–2015
|
|
16
|
Cookson MS, Aus G, Burnett AL, et al:
Variation in the definition of biochemical recurrence in patients
treated for localized prostate cancer: The American urological
association prostate guidelines for localized prostate cancer
update panel report and recommendations for a standard in the
reporting of surgical outcomes. J Urol. 177:540–545. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Howlader N, Noone AM, Krapcho M, Garshell
J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,
et al: SEER Cancer Statistics Review, 1975–2012. Bethesda, MD:
National Cancer Institute. http://seer.cancer.gov/csr/1975_2012/Accessed.
December 02–2013
|
|
18
|
Jadvar H, Desai B, Ji L, et al:
Prospective evaluation of 18F-NaF and 18F-FDG PET/CT in detection
of occult metastatic disease in biochemical recurrence of prostate
cancer. Clin Nucl Med. 37:637–643. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gillies RJ, Robey I and Gatenby RA: Causes
and consequences of increased glucose metabolism of cancers. J Nucl
Med. 49(Suppl 2): 24S–42S. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Smith TA: Mammalian hexokinases and their
abnormal expression in cancer. Br J Biomed Sci. 57:170–178.
2000.PubMed/NCBI
|
|
21
|
Effert P, Beniers AJ, Tamimi Y, Handt S
and Jakse G: Expression of glucose transporter 1 (GLUT-1) in cell
lines and clinical specimen from human prostate adenocarcinoma.
Anticancer Res. 24:3057–3063. 2004.PubMed/NCBI
|
|
22
|
Stewart GD, Gray K, Pennington CJ, et al:
Analysis of hypoxia-associated gene expression in prostate cancer:
Lysyl oxidase and glucose transporter-1 expression correlate with
Gleason score. Oncol Rep. 20:1561–1567. 2008.PubMed/NCBI
|
|
23
|
Kukuk D, Reischl G, Raguin O, et al:
Assessment of PET tracer uptake in hormone-independent and
hormone-dependent xenograft prostate cancer mouse models. J Nucl
Med. 52:1654–1663. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jadvar H, Ye W, Groshen S and Conti PS:
[F-18]-fl [F-18]-Fluorodeoxyglucose PET-CT of the normal prostate
gland. Ann Nucl Med. 22:787–793. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shiiba M, Ishihara K, Kimura G, et al:
Evaluation of primary prostate cancer using 11C-methionine-PET/CT
and 18F-FDG-PET/CT. Ann Nucl Med. 26:138–145. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Minamimoto R, Uemura H, Sano F, Terao H,
Nagashima Y, Yamanaka S, Shizukuishi K, Tateishi U, Kubota Y and
Inoue T: The potential of FDG PET/CT for detecting prostate cancer
in patients with an elevated serum PSA level. Ann Nucl Med.
25:21–27. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schöder H, Hermann K, Gönen M, Hricak H,
Eberhard S, Scardino P, Scher HI and Larson SM: 2-[18F]
fluoro-2-deoxyglucose positron emission tomography for detection of
disease in patients with prostate-specific antigen relapse after
radical prostatectomy. Clin Cancer Res. 11:4761–4769. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chang CH, Wu HC, Tsai JJ, et al: Detecting
metastatic pelvic lymph nodes by 18F-2-deoxyglucose positron
emission tomography in patients with prostate specific antigen
relapse after treatment for localized prostate cancer. Urol Int.
70:311–315. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jadvar H, Desai B and Quinn D: Treatment
response assessment of metastatic prostate cancer with FDG PET/CT.
J Nucl Med. 52(Suppl 1): 431P2011.
|
|
30
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumours: revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wahl RL, Jacene H, Kasamon Y and Lodge MA:
From RECIST to PERCIST: Evolving Considerations for PET response
criteria in solid tumors. J Nucl Med. 50:122S–150S. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hillner BE, Siegel BA, Shields AF, et al:
Relationship between cancer type and impact of PET and PET/CT on
intended management: Findings of the national oncologic PET
registry. J Nucl Med. 49:1928–1935. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hwang I, Chong A, Jung SI, et al: Is
further evaluation needed for incidental focal uptake in the
prostate in 18-fluoro-2-deoxyglucose positron emission
tomography-computed tomography images? Ann Nucl Med. 27:140–145.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Minamimoto R, Senda M, Jinnouchi S, et al:
The current status of an FDG-PET cancer screening program in Japan,
based on a 4-year (2006–2009) nationwide survey. Ann Nucl Med.
27:46–57. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wright JL, Lin DW and Stanford JL: The
effect of demographic and clinical factors on the relationship
between BMI and PSA levels. Prostate. 71:1631–1637. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Koochekpour S, Majumdar S, Azabdaftari G,
et al: Serum glutamate levels correlate with Gleason score and
glutamate blockade decreases proliferation, migration and invasion
and induces apoptosis in prostate cancer cells. Clin Cancer Res.
18:5888–5901. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bartoletti R, Meliani E, Bongini A, Magno
C and Cai T: Fluorodeoxyglucose positron emission tomography may
aid the diagnosis of aggressive primary prostate cancer: A case
series study. Oncol Lett. 7:381–386. 2014.PubMed/NCBI
|
|
38
|
Tombal B and Lecouvet F: Modern detection
of prostate cancer's bone metastasis: Is the Bone Scan Era Over?
Adv Urol. 2012:8931932012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mulders PF and Schalken JA: Measuring
therapeutic efficacy in the changing paradigm of castrate-resistant
prostate cancer. Prostate Cancer Prostatic Dis. 12:241–246. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ryan CJ, Shah S, Efstathiou E, et al:
Phase II study of abiraterone acetate in chemotherapy-naive
metastatic castration-resistant prostate cancer displaying bone
flare discordant with serologic response. Clin Cancer Res.
17:4854–4861. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Rabbani SA, Gladu J, Harakidas P, Jamison
B and Goltzman D: Over-production of parathyroid hormone-related
peptide results in increased osteolytic skeletal metastasis by
prostate cancer cells in vivo. Int J Cancer. 80:257–264. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Oyama N, Akino H, Suzuki Y, et al:
Prognostic value of 2-deoxy-2-[F-18] fluoro-D-glucose positron
emission tomography imaging for patients with prostate cancer. Mol
Imaging Biol. 4:99–104. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Meirelles GS, Schöder H, Ravizzini GC, et
al: Prognostic value of baseline [18F] fluorodeoxyglucose positron
emission tomography and 99mTc-MDP bone scan in progressing prostate
cancer. Clin Cancer Res. 16:6093–6099. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Jadvar H, Xiankui L, Shahinian A, et al:
Glucose metabolism of human prostate cancer mouse xenografts. Mol
Imaging. 4:91–97. 2005.PubMed/NCBI
|
|
45
|
Morris MJ, Akhurst T, Osman I, et al:
Fluorinated deoxyglucose positron emission tomography imaging in
progressive metastatic prostate cancer. Urology. 59:913–918. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Jadvar H, Desai B, Ji L, Conti PS, Dorff
TB, Groshen SG, Pinski JK and Quinn DI: Baseline 18F-FDG PET/CT
parameters as imaging biomarkers of overall survival in
castrate-resistant metastatic prostate cancer. J Nucl Med.
54:1195–1201. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
El Fakhri G, Surti S, Trott CM,
Scheuermann J and Karp JS: Improvement in lesion detection with
whole-body oncologic time-of-flight PET. J Nucl Med. 52:347–353.
2011. View Article : Google Scholar : PubMed/NCBI
|