Introduction
Isolated cortical vein thrombosis (ICoVT) is a rare
form of cerebral venous thrombosis (CVT). CVT is usually diagnosed
based on clinical manifestations, and magnetic resonance venography
(MRV) showing the vessel(s) with non-visualization thrombosis
(1). However, ICoVT is difficult to
diagnose because of the variation in numbers and locations of
cortical veins. Until recently, only a few cases or small series
with ICoVT have been reported (2–5),
suggesting the common misdiagnosis (2).
In the present study, 4 patients who were initially
diagnosed with glioma based on clinical presentations and
neuroimaging are reported. However, the pathological results of
subsequent biopsies supported a diagnosis of ICoVT. The clinical
and neuroimaging manifestations as well as the results of
pathological studies of these patients were retrospectively
analyzed to further differentiate ICoVT from brain tumors
clinically.
Case reports
Case 1
The patient was a 36-year-old Chinese man with
symptoms of progressive numbness and weakness of the right limbs in
the previous 6 months. The weakness was initially experienced in
the right toes. Subsequently, the weakness progressed, and the
right lower limb was inflicted 2 months later. At 5 months later
after the onset, the right upper extremity was also affected with
weakness and numbness. The patient did not suffer from fever,
nausea, vomiting, photophobia, headache, seizure or loss of
consciousness. He had no history of diabetes, hypertension or
autoimmune disorders. Prior physical examinations revealed his
blood pressure as 154/95 mmHg. No papilledema was observed
following fundoscopic examination. Right side of central facial and
lingual paralysis was experienced, as well as hypertonia and grade
4 muscle strength in the right limbs, with increased muscle stretch
reflexes and inducible myoclonus as well as positive Babinski's and
Chaddock's signs.
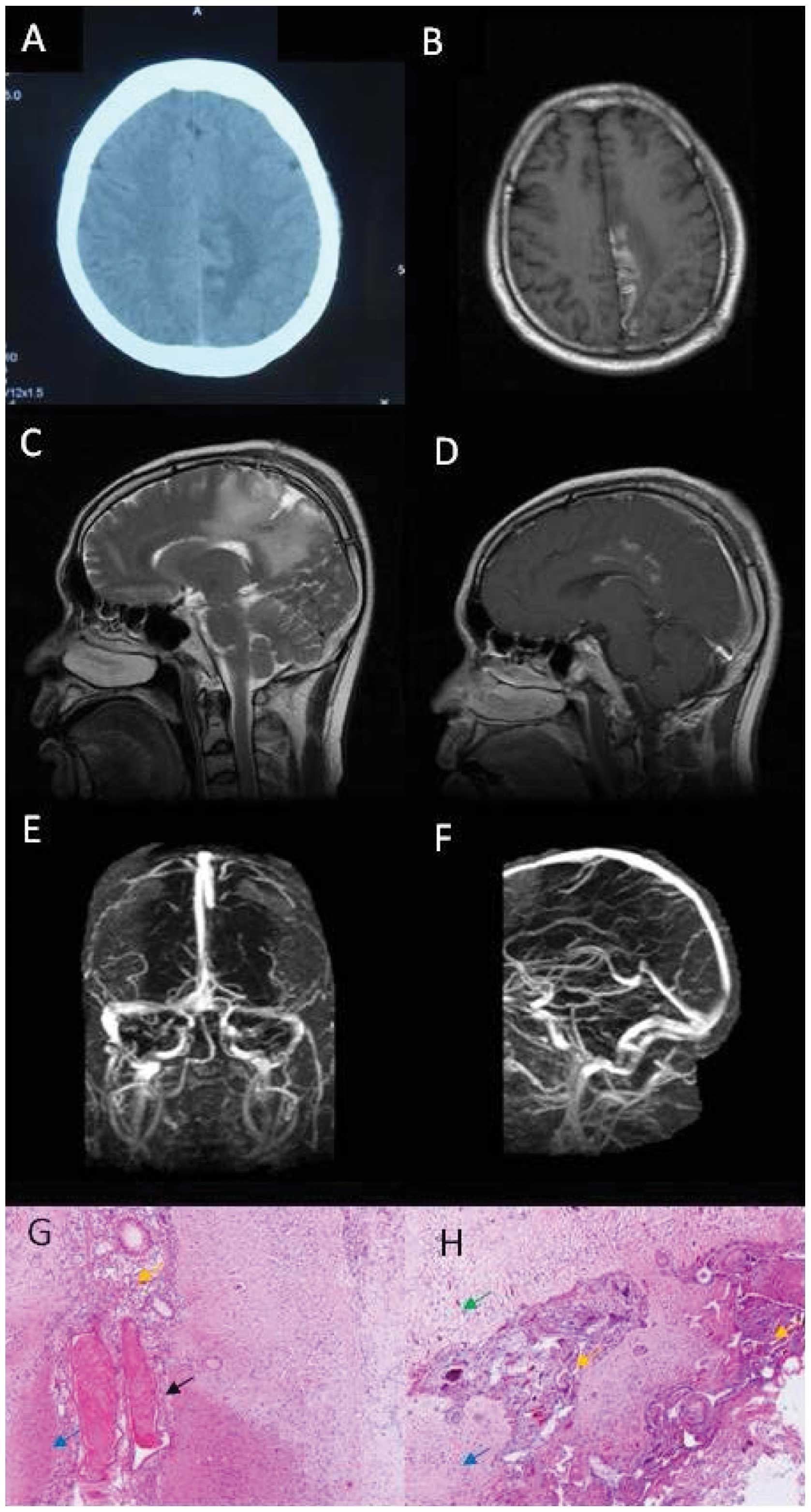
Brain computed tomography (CT) scan showed lesions
of hyperdensity mixed with hypodensity in the left parietal lobe
(Fig. 1A). Magnetic resonance imaging
(MRI) of the brain was performed including axial
T1-weighted image, T2-weighted image,
fluid-attenuated inversion recovery, apparent diffusion
coefficient, diffusion weighted imaging, sagittal
T2-weighted image and sagittal gadolinium
contrast-enhanced images and showed long T1 and
T2 signals, mixed with short T1 signal
(Fig. 1B and C) within the lesion,
with focal enhancement in contrast-enhanced MRI (Fig. 1D). The lumbar puncture revealed
cerebrospinal fluid (CSF) pressure was 143 mmH2O.
Cytological and chemical studies of CSF were normal. Other routine
laboratory tests including complete blood count (CBC) was normal.
Folic acid was 2.77 ng/ml and the triglyceride level was 2.99
mmol/l. Biomarkers for tumors were negative. Anti-neutrophil
cytoplasmic antibody (ANCA) and extractable nuclear antigen (ENA)
were negative. Antithrombin III deficiency, protein C and S
deficiency, and homocysteinemia were within normal limits.
Activated partial thromboplastin time (APTT) and D-dimer were
normal. Electroencephalography (EEG) was normal. In brain MRV,
major venous sinuses were patent without abnormality (Fig. 1E and F). Results of brain digital
subtraction angiography were normal. Brain biopsy was performed
because of suspected glioma. However, the pathological results
showed focal necrosis and degeneration of neurons, dilated small
veins with congestion or thrombosis, phagocytosis and gliosis, and
proliferation of small vessels and fibrous tissues, without tumor
cells or characteristics of inflammatory diseases (Fig. 1G and H).
The patient was consulted by a pathologist and
neurologist in the Navy General Hospital, and finally diagnosed
with ICoVT. The patient was then admitted to the Department of
Neurology for further management. The repeated lumbar puncture
showed that the pressure of CSF was >330 mmH2O. The
results of the cytological and chemical studies of CSF were normal.
Treatment commenced with intravenous (IV) heparin for 7 days,
followed by 6 days of oral Coumadin. The patient was discharged
with a grade 5− muscle strength in the right upper limb
and a grade 4 muscle strength in the right lower limb. Coumadin was
continued following discharge. Grade 5 muscle strength in the right
limbs was observed in a follow up 3 months after discharge, and
repeat brain MRI revealed long T1 and T2
signals, mixed with short T1 signal in the right
cingulate gyrus, with focal enhancement in contrast-enhanced MRI.
Routine laboratory tests including CBC, comprehensive metabolic
panel (CMP) and D-dimer were within normal limits. Oral Coumadin
was continued for an additional month, and then discontinued by the
patient. Full recovery was confirmed in a follow up 2 years later
as an outpatient. At this time, the patient refused to undergo a
brain MRI study.
Case 2
A 19-year-old Chinese woman presented with headache,
dizziness for 2 days and two episodes of seizures. Her headache was
constant dull pain in the left temporal region accompanied by
nausea and vomiting, but without fever or photophobia. The patient
experienced complex partial seizures, and each episode lasted ~1
min. She had no history of notable illness. The neurologic
examination was normal. Routine laboratory workups including CBC
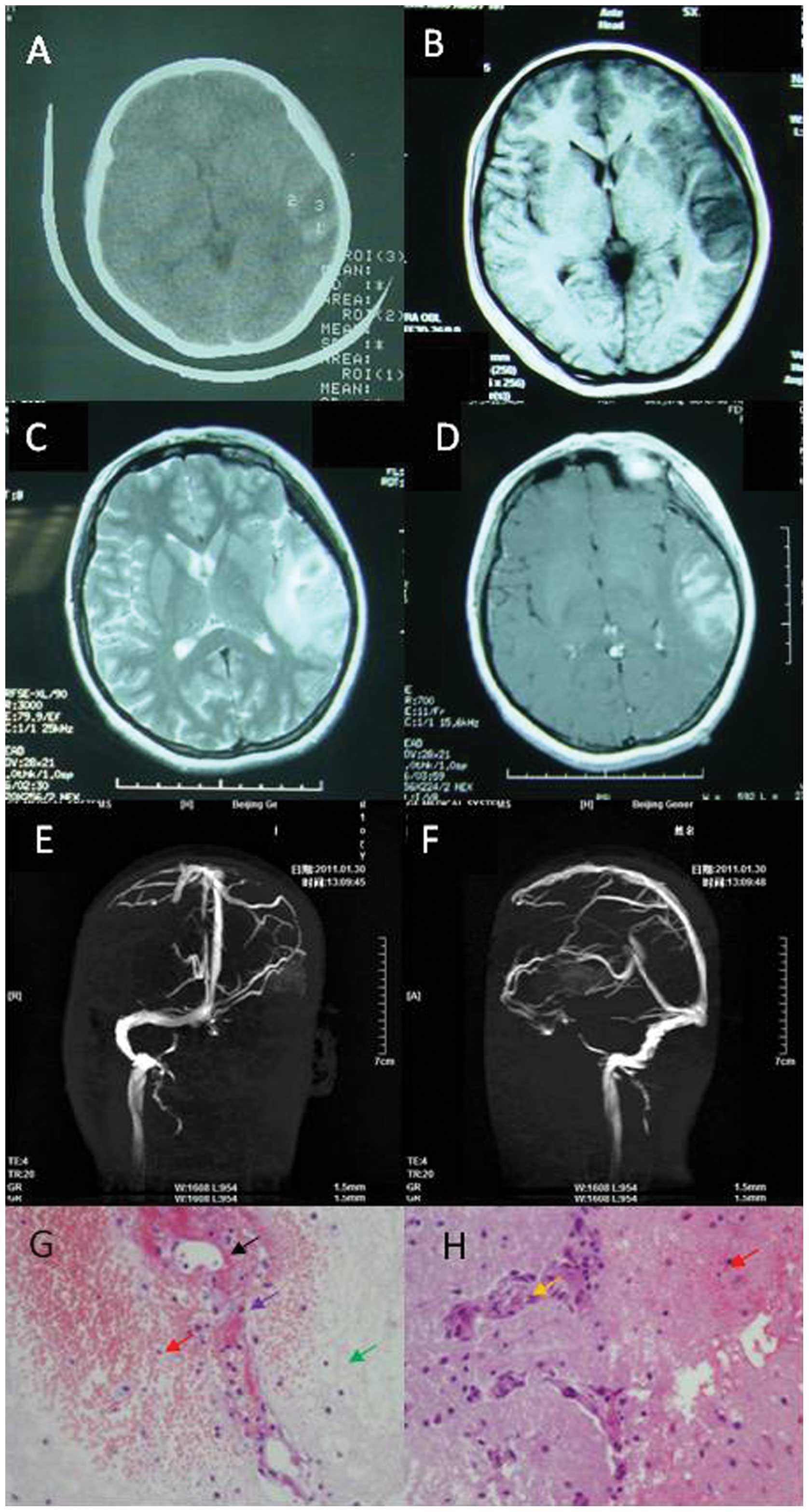
and CMP showed mild iron deficiency anemia. Brain CT showed lesions
of hypodensity mixed with hyperdensity in the left temporal lobe
(Fig. 2A). Brain MRI showed long
T1 and T2 signals surrounding the short
T1 signal in the left temporal lobe (Fig. 2B and C). No short T1 signal
or long T2 signal was identified in the sinus for venous
thrombus. Some focal enhancement was evident in the
contrast-enhanced MRI (Fig. 2D).
Lumbar puncture was completed, showing CSF pressure
of 220 mmH2O, and normal cytology and chemistry.
Homocysteinemia was 32.2 µmol/l, and folic acid was 3.3 nmol/l.
APTT and D-dimers were within the normal limits. Protein S was
decreased to 33% and protein C was normal. ANCA, ENA,
antiphospholipid, anticardiolipin antibodies and antithrombin III
were negative. Tumor biomarkers were also negative. EEG showed
asymmetrical slow-waves in the right frontal lobe, with a mean
frequency of ~1–3.5 Hz and a mean voltage of 30 mV. In the brain
MRI, left transverse and sigmoid sinus were not patent (Fig. 2E and F). Brain biopsy was performed
because of suspected glioma. However, the pathological analysis
revealed areolar tissue with focal necrosis, hemorrhage, necrosis
of vessel wall, phagocytosis, and proliferation in small vessels
(Fig. 2G and H). Based on the above
observations, the patient was diagnosed with ICoVT, and was treated
for 3 months with anticoagulant (initially with IV heparin for 7
days followed by oral Coumadin) for thrombosis and antiepileptics
for seizure. She was hospitalized for 16 days and did not report
any headache, dizziness or seizure during the 3 years of follow
up.
Case 3
A 32-year-old Chinese man presented with numbness
and weakness in the left limbs for 2 months. The patient
experienced numbness in the fingers of the left hand for 2 months
prior to admission. One month after admission, the patient felt
weak and numb on the left side of the face and upper limbs. The
weakness and numbness was not alleviated after taking oral
vitamins. The patient did not exhibit fever, seizure or headache.
He had no previous history of illness. The neurological examination
demonstrated hypertonia in the left limbs with grade 4 muscle
strength. The patient exhibited left hyperreflexia, and positive
Babinski's and Chaddock's signs. No papilledema was observed
following the fundoscopic examination. Routine laboratory tests
including CBC, CMP were normal. APTT and D-dimer were normal. Brain
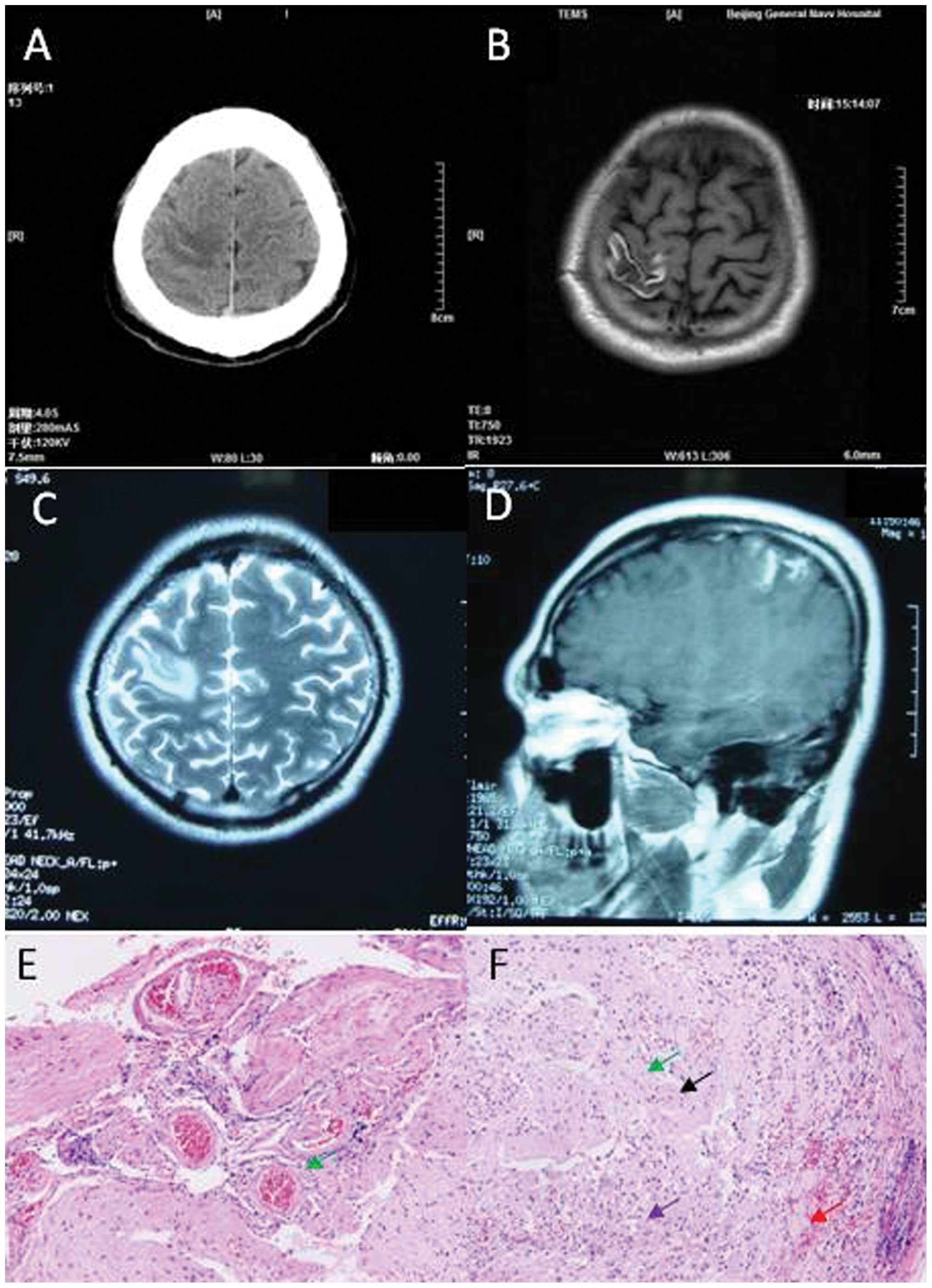
CT scan revealed hypodense lesions, within which there were
hyperdense lesions, in the right parietal lobe (Fig. 3A). Brain MRI revealed long signal in
the T1-weighted image and T2 weighed image,
with short signal in the T1-weighted image in the right
parietal lobe (Fig. 3B and C), and
focal enhancement was detected in the contrast-enhanced MRI
(Fig. 3D).
Lumbar puncture revealed CSF pressure of 160
mmH2O, protein level of 0.557 g/l. ANCA and ENA were
negative. Biomarkers for tumors were also negative.
Antiphospholipid and anticardiolipin antibodies, antithrombin III
deficiency, protein C and S deficiency, and homocysteinemia were
normal. EEG was normal. Brain biopsy was performed because glioma
was suspected. The pathological study showed sporadic hemorrhage,
tissue structure disappearance, astrocytic reaction, and microglia,
proliferation of small vessels, and perivascular cuffing (Fig. 3E and F). The patient was diagnosed
with ICoVT based on the comprehensive studies, and was treated with
anticoagulant, initially heparin for 7 days, followed by oral
Coumadin for 3 months. The patient was fully recovered, and was
able to walk normally without any numbness or weakness during the 4
years of follow up.
Case 4
A 23-year-old Chinese parturient visited clinic
following headache for 6 days and 1 episode of seizure. She
exhibited headache, which was persistent dull pain in the right
frontal lobe accompanied with vomiting and dizziness. She had a
cold without fever prior to the delivery of the baby. The one-time
seizure lasted for several minutes, with loss of consciousness,
lockjaw, tonic and clonic in limbs, and urinary and fecal
incontinence. The patient did not have a history of major illness.
The neurologic examination was normal. Her D-dimer was normal. The
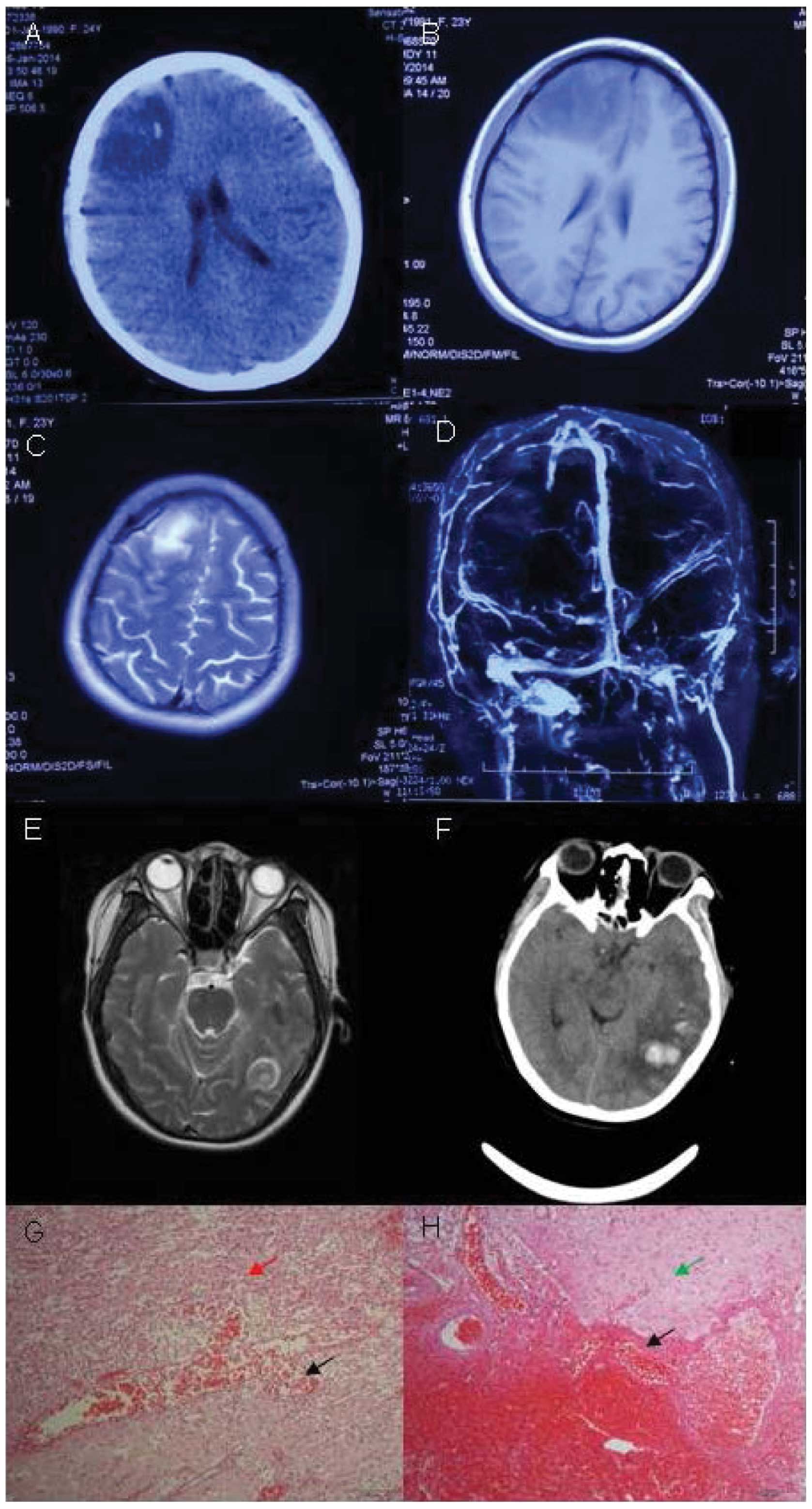
brain CT scan revealed hypodense mixed with hyperdense lesions in
the right frontal lobe (Fig. 4A). The
brain MRI revealed long signal in the T1-weighted image
and the T2-weighted image, mixed with short
T1 signal in the right frontal lobe (Fig. 4B and C). Contrast-enhanced MRI showed
focal enhancement within the lesion. In the brain MRV, the major
venous sinuses were patent without abnormalities (Fig. 4D). The pressure CSF was 240
mmH2O, and red blood cell (RBC) count was
290×106/l in CSF. CBC, CMP and APTT were normal. D-dimer
was 1,949 ng/ml (<429 ng/ml). Protein S activity was 53% and
protein C activity was 52%. ANCA, ENA, antiphospholipid,
anticardiolipin antibodies and antithrombin III were negative. The
tumor biomarkers were also negative. Brain tumor was suspected and
the patient was hospitalized. Right frontal brain biopsy was
performed. Her conditions deteriorated and she became comatose 2
days after the surgery. Bilateral papilledemas were observed with
blurry border of discus opticus. Her left limbs had grade 2 muscle
strength and her right limbs had grade 4 muscle strength.
Repeat brain MRI revealed large cerebral hemorrhage
in the left temporal and occipital lobes (Fig. 4E). Pathological results showed focal
necrosis, hemorrhage with lots of gitter cells, astrocytic
reaction, degeneration of neurons and endothelial proliferation in
small vessels, and a focal vascular mass with vasodilatation and
congestion (Fig. 4G and H). The
pathological study did not support the diagnosis of brain tumor and
ICoVT was considered the final diagnosis. The patient was
administered an anticoagulant and antiepileptic. On the first day
of anticoagulant treatment with IV heparin, her conditions did not
improve and she remained in the coma. The left limbs had grade 1
muscle strength and the right limbs had grade 3 muscle strength.
Another brain CT was performed, which showed cerebral hemorrhage in
the left temporal and occipital lobes with mass effect (Fig. 4F). The treatment of anticoagulant was
suspended for two days, and then restarted. During the
anticoagulant treatment for the following 2 days, her conditions
improved and the patient regained consciousness. The left limbs
showed grade 3 muscle strength, and the right limbs had grade 4
muscle strength.
After 12 days of treatment with heparin followed by
15 days of oral Coumadin, the patient was able to walk
independently. At 20 days after admission, the patient received a
repeat brain MRI which showed that cerebral hemorrhage in the left
temporal and occipital lobes was reduced. At 21 days after
admission, lumbar puncture showed that the pressure of CSF was 270
mmH2O, and RBC Count was 3×106/l. CBC and CMP
were normal. The patient remained in the hospital for 46 days, and
was then discharged with grade 5− muscle strength in the
left extremities and normal strength in the right limbs. She was
able to speak fluently and clearly, and open-close eyes freely when
leaving the hospital. Repeat brain CT scan showed mixed density of
lesions in the left temporal and occipital lobes, and hypodense
lesions in the right frontal lobe. The patient continued oral
Coumadin and was under rehabilitaion for mild paralysis.
Discussion
CVT is a relatively uncommon but potentially
life-threatening condition, accounting for 1–2% of strokes in young
adults (6). CVT includes dural sinus
thrombosis, deep venous thrombosis and ICoVT. As previously
reported, the mortality rate of CVT ranged between 5 and 30%
(7). ICoVT is even less common,
accounting for 17% of CVT (8), and
its prognosis is good with early diagnosis and appropriate
management. However, early diagnosis of ICoVT is difficult both
clinically and radiologically (5).
Patients undergo brain biopsy as they are initially diagnosed with
brain tumors. and are then diagnosed with ICoVT following
comprehensive workups including pathological examinations.
It has been reported that usage of oral
contraceptive, pregnancy or puerperium, infection, genetic
thrombophilia, lumbar puncture, malignancy, sinusitis, trauma and
surgery, intracranial hypotension, history of lumbar puncture, and
medications constitute risk factors for ICoVT (8). Of the 4 patients presented in the
current study, decreased protein S activity was detected in 1
patient, and another patient was postpartum.
The neuroimaging features of ICoVT include the
primary changes of the affected superficial cortical vein, which
can be directly visualized and the secondary changes of venous
outflow obstruction in brain MRI. Venous congestion was evident as
swollen gyri (5). Imaging of ICoVT
revealed focal hemorrhage venous infarction and edema. Parenchymal
changes were usually subcortical (2).
Intracranial vascular malformations, hemorrhage transformation in
ischemic infarctions, aneurysm rupture and bleeding within the
brain due to a tumor were among the deferential diagnoses.
For our patients, the primary pathological findings
were focal necrosis, hemorrhage, and dilated small vein with
congestion or thrombosis. Degeneration of neuron, phagocytosis,
gliosis and endothelial proliferation in small vessels were also
observed. Although a pathological study is not recommended
routinely for ICoVT, it is valuable for some patients when they do
not present with typical T2* imagings, or especially
when the differentiation with brain tumor is difficult. Early
diagnosis is important for patients with ICoVT since early
management is associated with favorable outcome.
In the present study, the 4 cases were initially
misdiagnosed as brain tumors because of atypical clinical
presentations and neuroimaging studies. However, the final
diagnoses of ICoVT were made based on the comprehensive workups
including the pathological studies. According to the guidelines of
‘Diagnosis and management of cerebral venous thrombosis’ (8), patients who exhibit CVT are required to
receive neuroimaging studies including
T2-weighted-gradient-echo image, which may have high
accuracy of diagnosis. However, whether
T2-weighted-gradient-echo image was useful for the
patients of the present study was unclear. The accuracy of the
misdiagnosis of ICoVT with brain tumors in the patients who
underwent brain biopsy also remains unclear. For difficult
patients, a pathological examination would be useful in determining
the diagnosis, and the subsequent treatment such as
anticoagulation.
In summary, ICoVT is an uncommon disease that is
often difficult to diagnose because of non-specific clinical
presentations and atypical CT and MRI imaging findings. Brain
biopsy is probably the last resort for making the diagnosis. For
difficult cases, such as those examined in the present study,
earlier diagnosis even with brain biopsy is important for improved
prognosis and treatment.
References
|
1
|
Hinman JM and Provenzale JM: Hypointense
thrombus on T2-weighted MR imaging: a potential pitfall in the
diagnosis of dural sinus thrombosis. Eur J Radiol. 41:147–152.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Coutinho JM, Gerritsma JJ, Zuurbier SM and
Stam J: Isolated cortical vein thrombosis: systematic review of
case reports and case series. Stroke. 45:1836–1838. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rathakrishnan R, Sharma VK, Luen TH and
Chan BP: The clinico-radiological spectrum of isolated cortical
vein thrombosis. J Clin Neurosci. 18:1408–1411. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Xue SF, Ma QF, Ma X and Jia JP: Isolated
cortical vein thrombosis: a widely variable clinicoradiological
spectrum. Eur Neurol. 69:331–335. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sharma VK and Teoh HL: Isolated cortical
vein thrombosis - the cord sign. J Radiol Case Rep. 3:21–24.
2009.PubMed/NCBI
|
|
6
|
Cohen JE, Duck M, Gomori JM, Itshayek E
and Leker RR: Isolated cortical vein thrombosis: a rare cause of
venous stroke with good prognosis after timely diagnosis and
treatment. Neurol Res. 35:127–130. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Khealani BA, Wasay M, Saadah M, Sultana E,
Mustafa S, Khan FS and Kamal AK: Cerebral venous thrombosis: a
descriptive multicenter study of patients in Pakistan and Middle
East. Stroke. 39:2707–2711. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saposnik G, Barinagarrementeria F, Brown
RDJ Jr, Bushnell CD, Cucchiara B, Cushman M, deVeber G, Ferro JM
and Tsai FY: American Heart Association Stroke Council and the
Council on Epidemiology and Prevention: Diagnosis and management of
cerebral venous thrombosis: a statement for healthcare
professionals from the American Heart Association/American Stroke
Association. Stroke. 42:1158–1192. 2011. View Article : Google Scholar : PubMed/NCBI
|