Introduction
Teratomas are a common tumor type that mainly occur
in children and infants. The majority of cases are benignant,
arising arise from the ovaries, retroperitoneum or sacrococcygeal
region. However, a few cases are malignant and occur in middle age.
Teratomas of the posterior mediastinum are uncommon tumors with a
slow growth rate and a low incidence rate, accounting for only
8–13% of all tumors of the posterior mediastinum (1). They are mainly incidentally detected by
chest imaging since there are no marked clinical symptoms.
Treatment by surgical excision can achieve satisfactory
results.
Situs inversus is a rare autosomal recessive
disorder in which the organs are transposed from their normal
location to the opposite side of the body (2). In India, the reported incidence of situs
inversus is one case per 6,000–35,000 live births (3). The first known human case was reported
by Fabricius in 1600 (2). The
condition is termed situs inversus totalis when both the abdominal
and thoracic viscera, including the dextrocardia, are involved.
When present, it may be associated with several other
abnormalities, including bronchiectasis, sinusitis and deficient
tracheobronchial cilia, which is then known as Kartagener's
syndrome. To the best of our knowledge, at present, the association
between situs inversus totalis and teratoma has not been reported
in the literature.
The present study describes the case of a
23-year-old woman who presented with situs inversus totalis and a
mature teratoma in the posterior mediastinum.
Case report
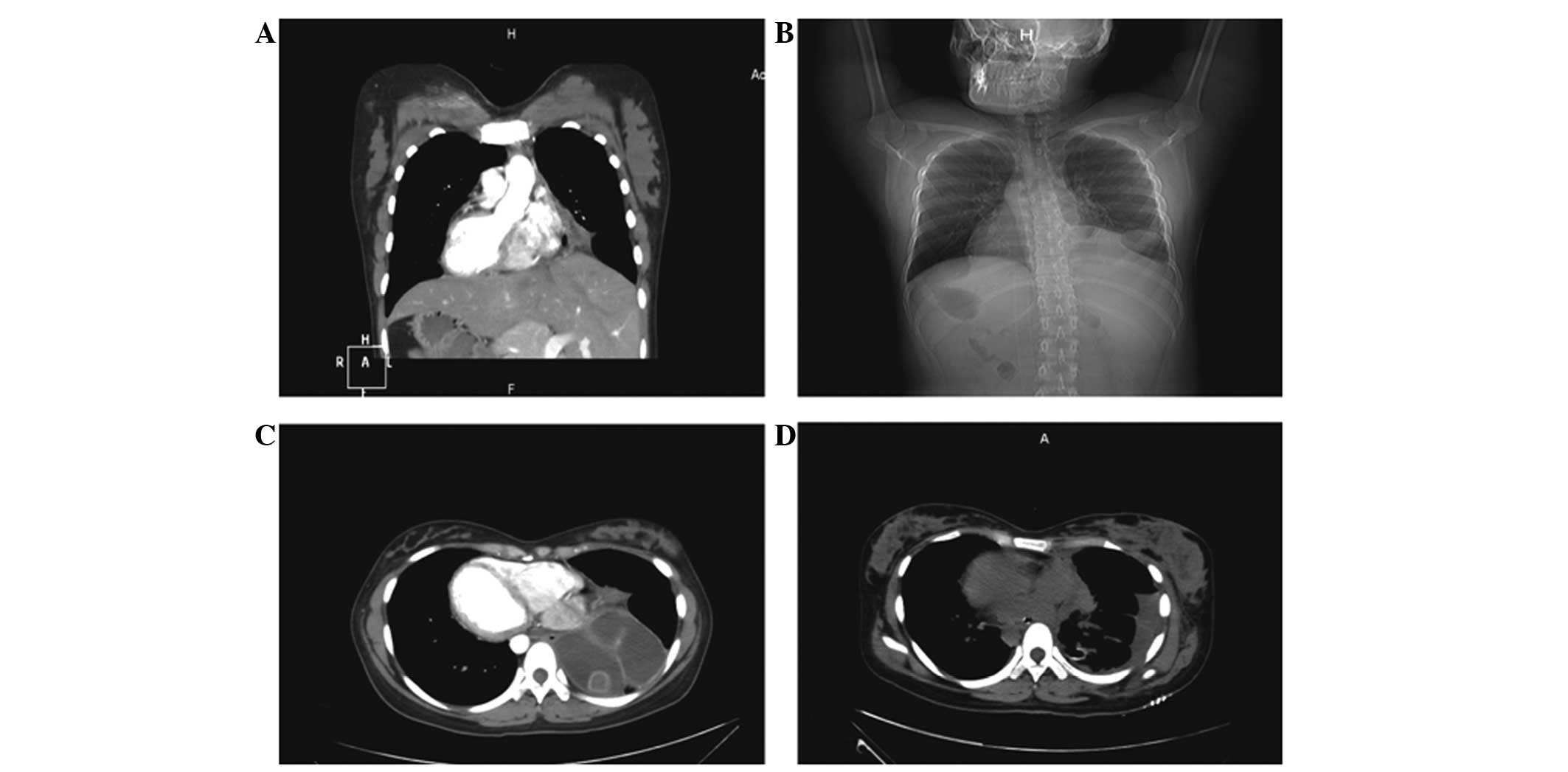
In July 2014, a 23-year-old woman presented to The
First Affiliated Hospital of Zhengzhou University with a 3-year
history of intermittent chest tightness. A chest computed
tomography (CT) scan and X-ray showed a mediastinal mass. The X-ray
also revealed dextrocardia with a fundic gas shadow on the right
side and a liver shadow on the left side (Fig. 1A and B). Contrast-enhanced CT was
performed to obtain further information and revealed a posterior
mediastinal complex cystic mass that was 10 cm in diameter
(Fig. 1C). Following the radiological
examination, a teratoma and situs inversus totalis were diagnosed.
The physical examination showed that the patient was healthy with
normal functional capacity since there was no fever, hypertension
or abnormal respiration.
Surgery was performed to resect the teratoma. CT
showed the presence of pleural effusion subsequent to the surgery
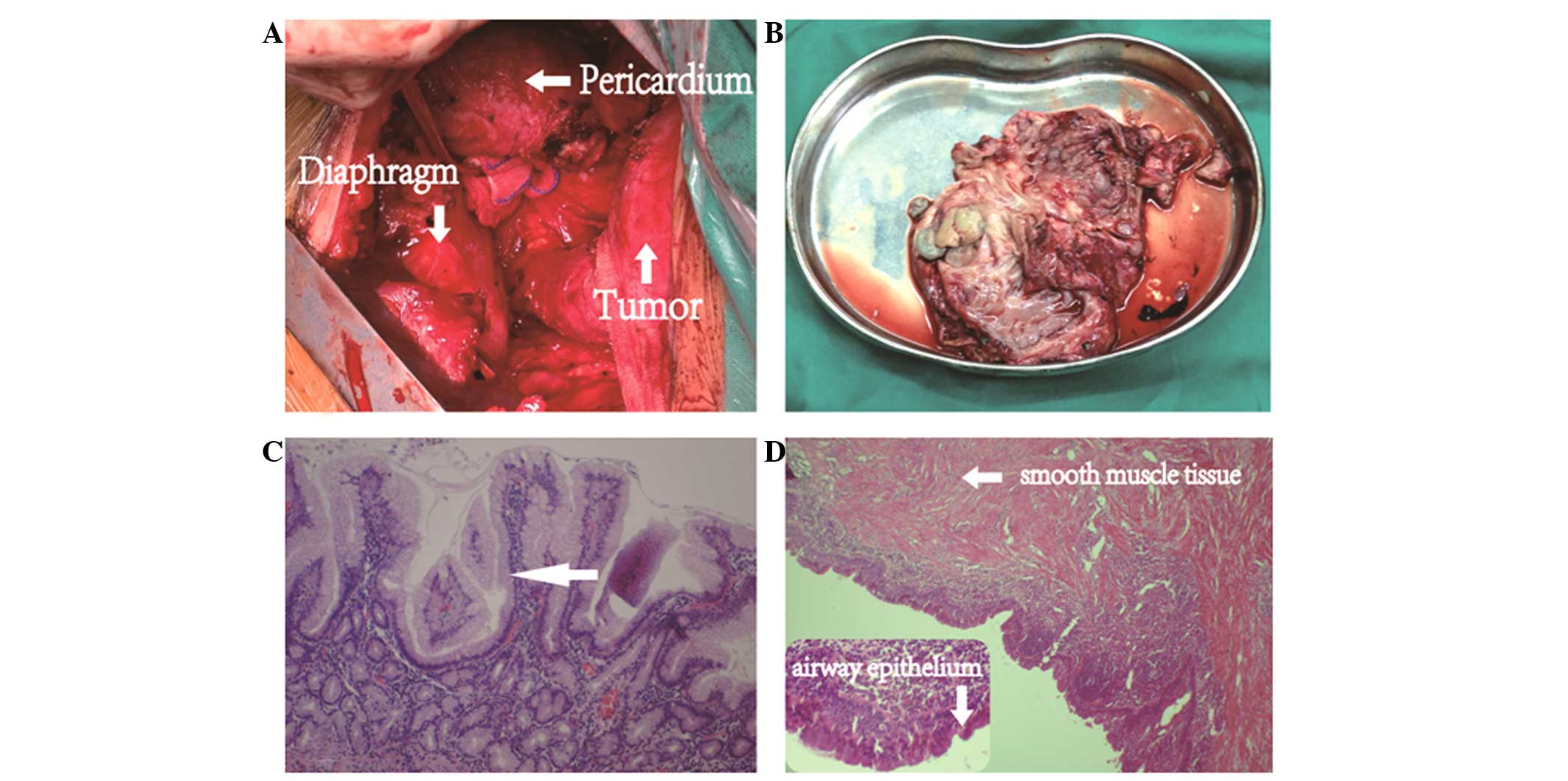
(Fig. 1D). Grossly, the resected
surgical specimen was a 9×6.5×3.5-cm cystic mass, full of yellow
pultaceous material and clear liquid (Fig. 2A and B). The wall of the cystic mass
was observed to be divided by stratified squamous epithelium with
an underlying simple ciliated columnar epithelium and sebaceous
glands upon microscopy. Additionally, smooth muscle cells and
adipose tissues were observed in the wall (Fig. 2C and D). A mature teratoma was
diagnosed histologically since there was no evidence of malignancy.
The patient exhibited a normal recovery after surgery and was
discharged from hospital 9 days later. Follow-up was performed 6
months after surgery; X-ray examination and computed tomography
scans revealed no residual mass or disease recurrence.
Discussion
Teratomas are a type of neoplasm arising from the
pluripotent embryonic cells and containing three germ layers. No
evident clinical symptoms of mediastinal teratomas exist until
terminal stages. Teratomas in the mediastinum are often detected
incidentally by chest X-ray. Pectoralgia, expiratory dyspnea and
coughing are symptoms that may be caused by the compression of
nearby structures. A rupture of the teratoma may cause superior
vena cava syndrome or pneumonia, but occurs rarely (4). To the best of our knowledge, the current
study represents the first case of a teratoma in the mediastinum in
a patient with situs inversus totalis.
Surgical resection is the main choice for the
treatment of a mediastinal teratoma since it aids in confirming the
correct diagnosis and preventing complications. The majority of
teratomas in the mediastinum are benign, while only 1–5% are
malignant (5,6). There are a number of indicators of
malignancy in teratomas, such as invasion of the myocardium and
great vessels (6). These indicators
attest to the requirement for extensive surgery. The associated
regions of the adherent mediastinal pleura and pericardium can be
removed during the surgery. Since the majority of teratomas in the
mediastinum are benign, a subtotal excision could achieve
satisfactory results. With the progression of medical technology,
optimal surgical results have been obtained (7).
Data on patients with situs inversus and peptic
conditions, ulcer perforation, amoebic liver abscesses, acute
cholecystitis, cholelithiasis, acute appendicitis or intestinal
obstructions have been reported (8).
However, with the exception of the present study, there have been
no reports with regard to teratoma associated with situs inversus
totalis. Establishment of a detailed and precise assessment prior
to surgery is important in such cases.
In conclusion, this study is the first to report a
patient with situs inversus totalis and posterior mediastinal
teratoma. The patient was diagnosed via radiological methods and
surgery was performed. The patient made a full recovery after
surgical resection, and continues to attend follow-up examinations.
We hypothesize that the occurrence of situs inversus totalis
accompanied with posterior mediastinal mature teratoma in this
patient may have been a coincidence, however, it may present a rare
syndrome. To the best of our knowledge, no data regarding the
association between situs inversus totalis and teratoma has been
reported in the literature to date. Thus, similar cases must be
reported in the future.
References
|
1
|
Anushree CN and Shanti V: Mature
mediastinal teratoma. J Clin Diagn Res. 9:ED05–ED06.
2015.PubMed/NCBI
|
|
2
|
Pitiakoudis M, Tsaroucha AK,
Katotomichelakis M, Polychronidis A and Simopoulos C: Laparoscopic
cholecystectomy in a patient with situs inversus using
ultrasonically activated coagulating scissors. Histopathology. Acta
Chir Belg. 105:114–117. 2005.PubMed/NCBI
|
|
3
|
Patel RB, Bhadreshwara K and Hukkeri S:
Laparoscopic appendicectomy in a patient with situs inversus
totalis. Indian J Surg. 75((Suppl 1)): S41–S43. 2013. View Article : Google Scholar
|
|
4
|
Nichols CR: Mediastinal germ cell tumors.
Histopathology. Chest. 99:472–479. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ousehal A, Skalli A, Nejjar M, Belaabidia
B and Kadiri R: Malignant bilateral mediastinal teratoma, A case
report. J Radiol. 82:174–176. 2001.(In French). PubMed/NCBI
|
|
6
|
Levitt RG, Husband JE and Glazer HS: CT of
primary germ-cell tumors of the mediastinum. AJR Am J Roentgenol.
142:73–78. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tsubochi H, Endo S, Nakano T, Minegishi K,
Tetsuka K and Hasegawa T: Extraction of mediastinal teratoma
contents for complete thoracoscopic resection. Asian Cardiovasc
Thorac Ann. 23:42–45. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Agarwal G and Kar DK: Teratoma of the
anterior mediastinum presenting as a cystic neck mass: A case
report. J Med Case Rep. 2:232008. View Article : Google Scholar : PubMed/NCBI
|