Introduction
Meningiomas account for 34.7% of all primary
intracranial tumors observed in adults, the majority of which are
benign (1). However, these tumors
rarely develop at the intrasellar region; only 12 pathologically
diagnosed cases have been reported previously (2–12), and the
presence of a malignant intrasellar meningioma is even rarer
(2–4).
The current study describes the case of a female patient presenting
with a malignant intrasellar meningioma appearing to mimic a
non-functioning invasive macroadenoma. This particular type of
meningioma demonstrates unique features when compared with
meningiomas in other locations (2,3,5–8,13,14). An
accurate pre-operative diagnosis is necessary in order for the
required treatment to be administered or surgery to be completed.
Due to the high risk of recurrence and cavernous sinus invasion
following an initial surgery, re-operation is often required and
may lead to an increased risk of complications when compared with
similar tumors at other locations. In the present study, the
patient benefited from active treatment, including chemotherapy and
radiotherapy. The findings also presented evidence that malignant
meningiomas closely associated with important adjacent structures
should be treated extensively initially, since reoperation may
cause serious neurological impairment. Written informed consent was
obtained from the patient.
Case report
A 35-year-old woman described a 2-month history of a
persistent, bilateral, parieto-occipital headache combined with 1
week of vomiting. The patient was therefore referred to the
Department of Neurosurgery, West China Hospital (Chengdu, China) in
July 2011, with an initial diagnosis of a non-functioning pituitary
adenoma. The patient noted the onset of right ptosis and diplopia
2-days after hospital admission. Physical examination found mild
right III and VI cranial nerve disturbance. No other abnormal signs
were observed.
Hormone tests prior to surgical intervention
revealed decreased levels of triiodothyronine (T3) (1.01 nmol/l;
normal range, 1.30–3.10 nmol/l) and free T3 (2.92 pmol/l; normal
range, 3.60–7.50 pmol/l), with a slightly elevated prolactin level
(38.47 ng/ml; normal range, 6.0–29.9 ng/ml). Other hormone levels
were all normal. Specific cancer-associated serum markers,
including α-fetoprotein (AFP), carcinoembryonic antigen (CEA),
cancer antigen (CA)15–3, CA19-9, CA-125, CA72-4 and cytokeratin 19
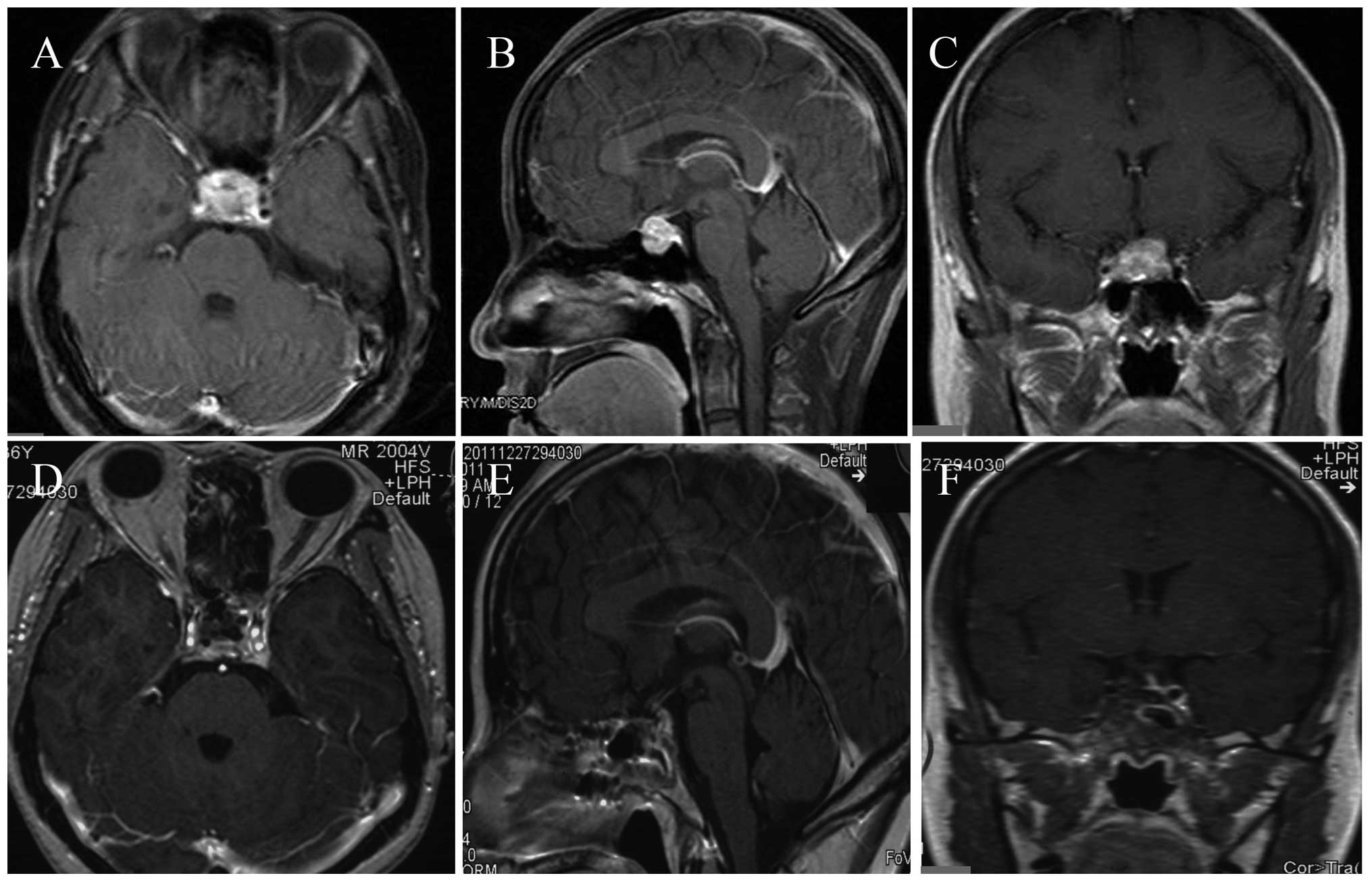
fragment 21-1 were also normal. A magnetic resonance imaging (MRI)
scan revealed a 1.7×1.9×2.1-cm, enhanced, heterogeneous,
intrasellar mass with invasion into the right cavernous sinus, and
the optic chiasm was slightly displaced (Fig. 1A–C). No lesion was observed on the
enhanced computed tomography (CT) scan of the chest and
abdomen.
The slightly hypervascularized mass was removed
subtotally through a transsphenoidal approach. The tumor was soft
enough to remove with gentle curettage, unlike previously reported
fibrous lesions (5,13). The cavernous sinus wall was invaded
under intraoperative visual inspection and no post-operative
complications were detected. Tissue samples were formalin-fixed,
paraffin-embedded and cut into 3-µm sections, prior to staining
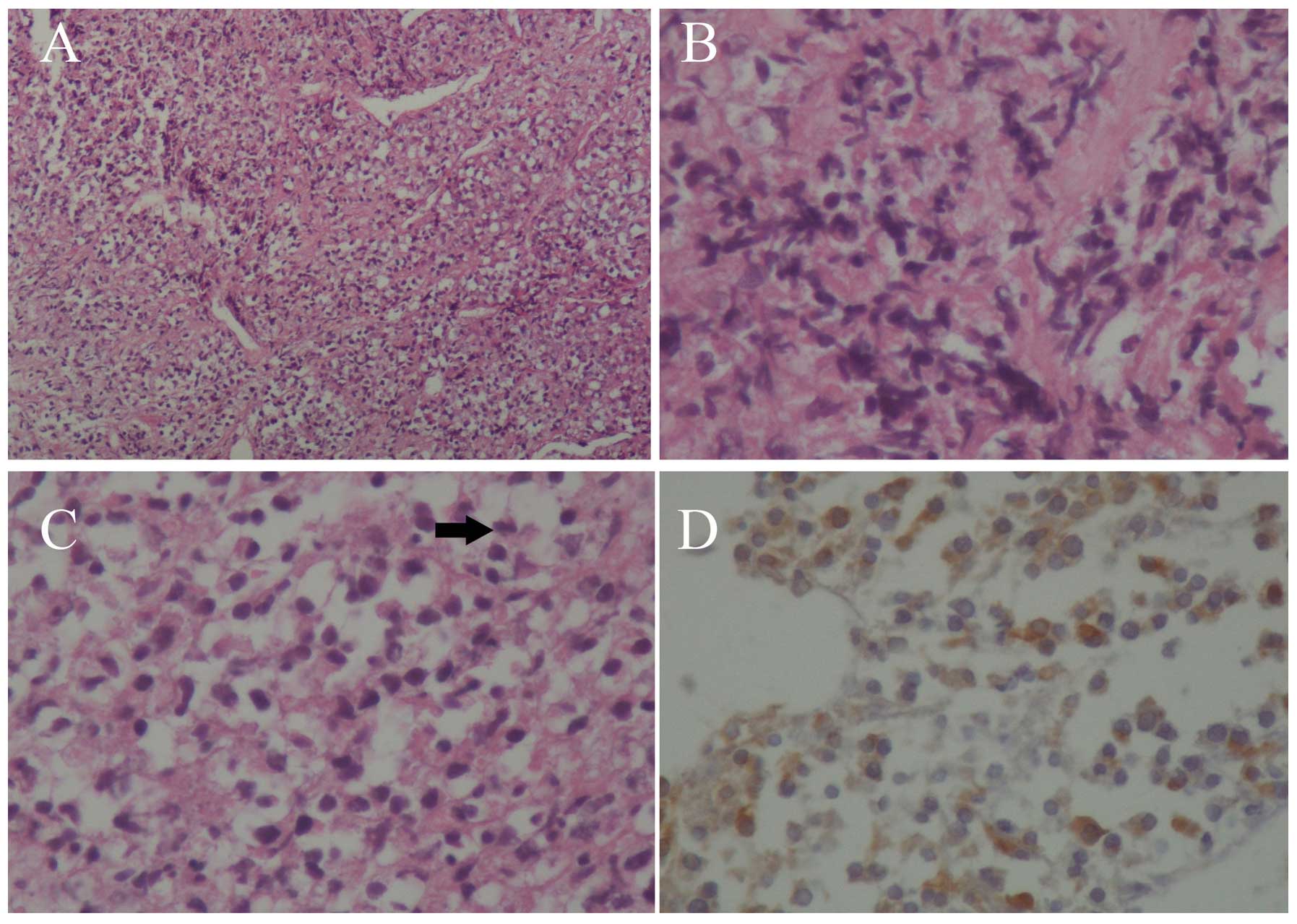
with hematoxylin and eosin. When observed under the microscope, the
tumor tissue exhibited increased cellularity, a sheet-like growth
pattern and necrosis. Neoplastic cells with anaplastic prominent
nucleoli and high mitotic activity were also noted [>20/10
high-power fields (HPFs)] (Fig.
2A–C), with a Ki-67 labeling index of up to 40%.
Immunohistochemical (IHC) examination revealed positive staining
for vimentin (Fig. 2D), focally
positive staining for epithelial membrane antigen (EMA) and S100,
and negative staining for chromogranin, synaptophysin, glial
fibrillary acidic protein, AFP, placental alkaline phosphatase,
octamer-binding transcription factor 3/4, B-cell lymphoma 2,
cluster of differentiation (CD)34, leukocyte common antigen, CD117,
melan A, human melanoma black 45, CEA, myeloperoxidase, desmin,
cytokeratin 8 and CD30. No pituitary hormone was expressed. A
diagnosis of malignant meningioma [World Health Organization (WHO)
grade III (1)] was formed based on
the pathological findings and clinical features.
Following surgery, the patients headache was
partially alleviated, whilst the oculomotor paralysis persisted.
Adjuvant three-dimensional conformal radiation therapy (3D-CRT)
with a 32-Gy dose was implemented 1 week after surgery, aiming to
target the residual tumor in the cavernous sinus. Subsequently,
three 4-week cycles of combined chemotherapy treatment with
cyclophosphamide (3 g, days 1–3) and nimustine (125 mg, day 1) were
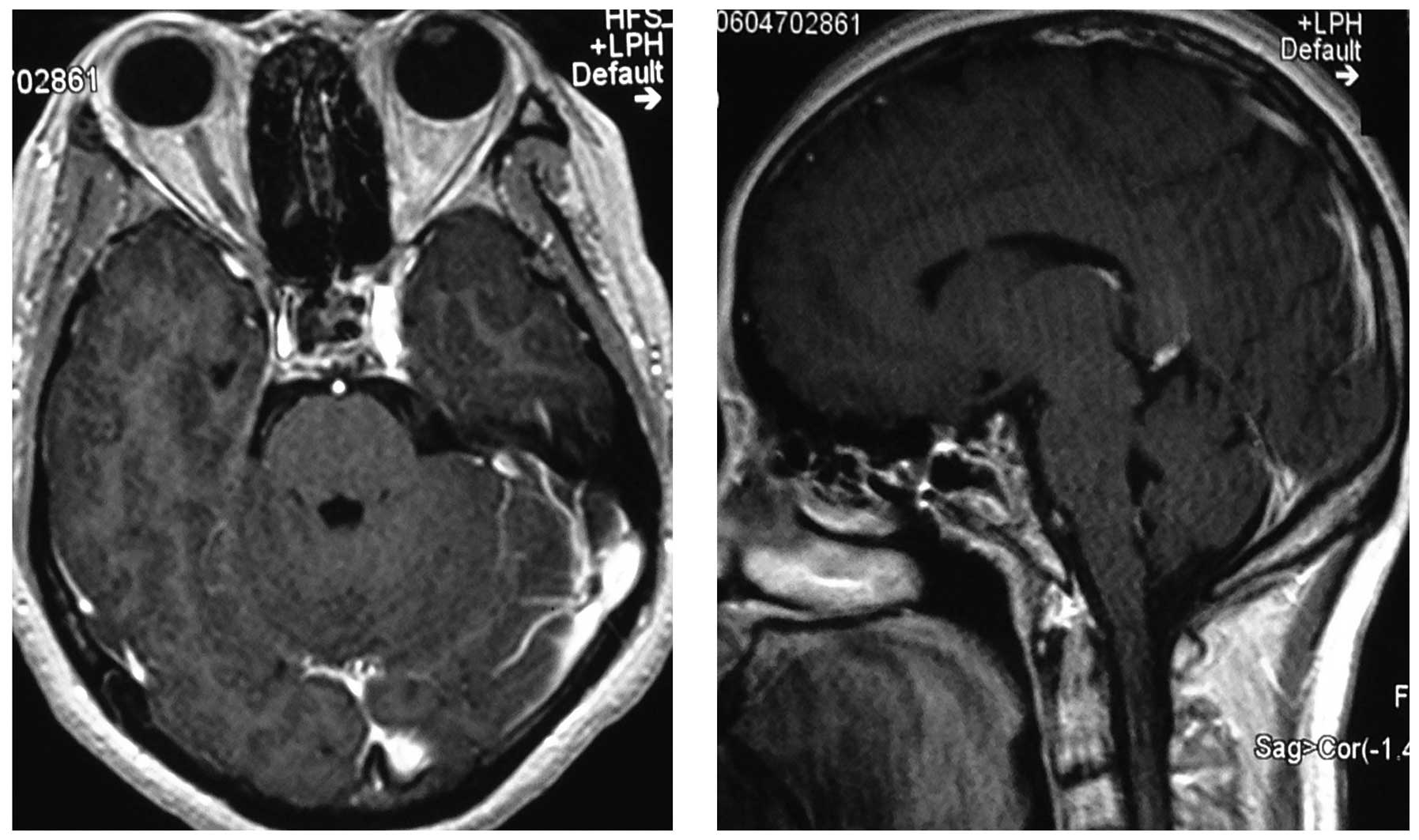
administered. The patient's symptoms ceased ~2 months after
chemotherapy, with no tumor regrowth detected during the 8-month
(Fig. 1D–F) and 3-year follow-ups
(Fig. 3).
Discussion
Meningiomas are common primary intracranial tumors
observed in adults that arise from the meningothelial cells of the
arachnoid mater, subsequently attaching to the adjacent dura mater
(15). Currently, meningiomas are
classified based on histological features, accepted as benign
(grade I), atypical (grade II) or anaplastic/malignant (grade III)
(1). Anaplastic or malignant
meningiomas account for only 1.0–2.8% of all meningiomas (6,16). The
surface area of the dura mater, located at the sella turcica, is
relatively small (<6 cm2), and meningiomas
originating from the sellar turcica have not been frequently
reported (17). Hardy and Robert
(18) first described an intrasellar
meningioma originating from the inferior leaf of the diaphragma.
Kinjo et al (14) classified
diaphragmatic meningiomas into three types, including type C, which
originates from the inferior leaf of the diaphragma sellar. Type C
diaphragm meningiomas resemble non-functioning pituitary adenomas,
and are commonly complicated by bitemporal hemianopsia and
hypopituitarism. Previously, Nozaki et al (2) reported the case of a hypervascularized
anaplastic intrasella meningioma and to the best of our knowledge,
the present study describes the second known case diagnosed as
malignant intrasellar meningioma originating from the dura mater of
the sellar turcica.
Intrasellar meningioma and pituitary adenoma share
comparable features on CT and MRI scans. Enlargement of the sellar
turcica is frequently observed, but an hourglass appearance is rare
among intrasellar meningiomas. CT and MRI scans may reveal a
well-enhanced intrasellar or intrasuprasellar mass that is
difficult to distinguish from pituitary adenoma, or even pituitary
apoplexy (7). Dural enhancement,
including the tail sign, is not specific, as it is one of the most
common manifestations of meningioma. However, a differential
diagnosis may still be conducted efficiently the majority of the
time. External carotid angiograms may demonstrate marked tumor
blush, and dynamic scanning techniques may be useful, as the
meningiomas exhibit complete enhancement with maximum signal
intensity during the early phase and a significantly different
time-intensity curve from that of pituitary adenomas (8).
We hypothesize that the transsphenoidal approach
should be considered to provide a moderately safe route to an
intrasellar mass (even with small suprasellar extension),
regardless of the pathological nature of the lesion. However, in
certain cases, it may not be the leading choice for intrasellar
meningiomas, as the tumor may be too firm to be extirpated and it
would therefore be difficult to control the hemorrhage, which
requires reoperation via transcranial approach. The combined
transsphenoidal and transcranial approach could be applied for
large intra-suprasellar masses. For cases with anaplastic or
malignant meningiomas, adjuvant radiotherapy should be
administered, as these tumors have a high rate of recurrence and
distant metastases. Despite chemotherapies and hormonal therapies
largely being proved as ineffective against the majority of
meningiomas, chemotherapies may, however, have potential in cases
demonstrating distant metastasis and an excessive mitotic index. In
the present study, 3D-CRT and concurrent chemotherapy were selected
due to the presence of tumor invasion into the cavernous sinus,
which leads to a high recurrence risk and subsequent adjacent nerve
adhesion. The alleviation of the patient's symptoms and an extended
tumor-free phase confirmed the effectiveness of the treatment.
Anaplastic/malignant meningiomas represent a higher
degree of cell cycle dysregulation and loss of differentiation,
with focal or diffuse findings of an excessive mitotic index
(>20/10 HPFs) and/or evident anaplasia (6,16). Tumor
necrosis and hemorrhage may also be present. The tumor cells may be
carcinoma-, sarcoma- or melanoma-like in appearance. Therefore, IHC
examinations, including EMA, vimentin, CK, S-100 and CEA, are
required to demonstrate meningothelial features that differ from
other malignant tumors. Geographic necrosis and brain invasion may
also be observed. In the current study, the tumor acquired several
anaplastic features with invasion to the carvernous sinus. A
variety of genetic changes have been identified in anaplastic
meningiomas, including N-myc downstream-regulated gene 2 (NDRG2)
hypermethylation, 17q23 amplification, loss of tumor suppressor in
lung cancer-1 and progesterone receptor expression, and alterations
in chromosomes, such as the loss in 1p, 6q, 9p21, 10, 14q and 18q
(19). Recent research has supported
the theory that molecular genetics serves a role in the
pathogenesis of atypical and anaplastic meningiomas, which may
promote anti-angiogenic and targeted molecular therapies to improve
the prognosis of high-grade meningiomas (20).
In conclusion, intrasellar meningioma mimicking
pituitary adenoma is rare and even rarer when malignant. WHO grade
III meningiomas have a recurrence rate of 50–80% and life
expectancy following diagnosis is ~2 years. With regard to
malignant intrasellar meningioma, substantial damage may incur due
to its location. However, in the present case, no recurrence was
observed in the 3 years following combined therapy. Further
research may aid in achieving an accurate pre-operative diagnosis,
confirming whether surgery and subsequent treatment is required.
Compared with possible recurrence affecting adjacent nerves when
patients are treated conservatively, those individuals with
malignant meningiomas in unique locations may benefit from
aggressive treatment combining chemotherapy and radiotherapy.
Research to elucidate the molecular hallmarks of anaplastic tumors
would be likely to aid the production of multi-modal and
molecular-targeted therapy in the future.
References
|
1
|
Louis DN, Ohgaki H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of the central nervous system. Acta
Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nozaki K, Nagata I, Yoshida K and Kikuchi
H: Intrasellar meningioma, Case report and review of the
literature. Surg Neurol. 47:447–454. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pinzer T, Krishnan KG and Schackert G: The
diaphragma sellae meningioma - a rare differential diagnosis of
non-functioning pituitary adenoma. Zentralbl Neurochir. 65:195–197.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Valassi E, Biller BM, Klibanski A and
Swearingen B: Clinical features of nonpituitary sellar lesions in a
large surgical series. Clin Endocrinol (Oxf). 73:798–807. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matsumoto S, Hayase M, Imamura H, Oda Y,
Kikuchi H, Katayama M and Ishihara T: A case of intrasellar
meningioma mimicking pituitary adenoma. No Shinkei Geka.
29:551–557. 2001.(In Japanese). PubMed/NCBI
|
|
6
|
Rogers L, Gilbert M and Vogelbaum MA:
Intracranial meningiomas of atypical (WHO grade II) histology. J
Neurooncol. 99:393–405. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Orakdöğeny M, Karadereler S, Berkman Z,
Erşahin M, Ozdoğan C and Aker F: Intra-suprasellar meningioma
mimicking pituitary apoplexy. Acta Neurochir (Wien). 146:511–515.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Satoh H, Arita K, Kurisu K, Sumida M,
Nakahara T, Eguchi K and Kuroki K: Intrasellar meningioma,
Characteristic imaging findings. Neuroradiology. 38:328–329. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Watanabe M, Toyama M, Watanabe M,
Taniguchi Y, Kaneko K and Yokoyama M: A case of intrasellar
meningioma with panhypopituitarism and hyperprolactinemia. No
Shinkei Geka. 15:869–874. 1987.(In Japanese). PubMed/NCBI
|
|
10
|
Nagao S, Kawai N, Ohomoto T and Oohashi T:
A case of intrasellar and suprasellar meningioma with
hypopituitarism. No Shinkei Geka. 18:637–642. 1990.(In Japanese).
PubMed/NCBI
|
|
11
|
Ildan F: Recurrent intrasellar meningioma
after total excision in a woman with hyperprolactinaemia. Turkish
Neurosurg. 4:93–97. 1994.
|
|
12
|
Yoneoka Y, Tanaka R, Minakawa T and Tamura
T: Psammomatous meningioma arising from the diaphragma sellae. Acta
Neurochir (Wien). 140:291–292. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kudo H, Takaishi Y, Minami H, Takamoto T,
Kitazawa S, Maeda S and Tamaki N: Intrasellar meningioma mimicking
pituitary apoplexy, Case report. Surg Neurol. 48:374–381. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kinjo T, al-Mefty O and Ciric I:
Diaphragma sellae meningiomas. Neurosurgery. 36:1082–1092. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cushing H: The meningiomas (dural
endotheliomas): Their source and favoured seats of origin. Brain.
45:282–316. 1922. View Article : Google Scholar
|
|
16
|
Sade B, Chahlavi A, Krishnaney A, Nagel S,
Choi E and Lee JH: World Health Organization Grades II and III
meningiomas are rare in the cranial base and spine. Neurosurgery.
61:1194–1198. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Grisoli F, Vincentelli F, Raybaud C,
Harter M, Guibout M and Baldini M: Intrasellar meningioma. Surg
Neurol. 20:36–41. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hardy J and Robert F: A meningioma of the
sella turcica subdiaphragmatic variety. Histopathology.
Neurochirurgie. 15:535–543. 1969.(In French). PubMed/NCBI
|
|
19
|
Perry A, Gutmann DH and Reifenberger G:
Molecular pathogenesis of meningiomas. J Neurooncol. 70:183–202.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wen PY, Quant E, Drappatz J, Beroukhim R
and Norden AD: Medical therapies for meningiomas. J Neurooncol.
99:365–378. 2010. View Article : Google Scholar : PubMed/NCBI
|