Introduction
Localized amyloidoma is generally divided into two
styles: AL-type and AA-type. AL-type occurs with an immunocyte
dyscrasia while AA-type occurs with chronic infection,
non-immunocyte neoplasia or inflammation. Localized amyloidoma
occurs most often in the mediastinum or abdomen. Although
amyloidomas may occur in almost all organ systems in the body;
however, primary amyloidoma of the renal pelvis is rare. Using the
keywords: ‘renal pelvis’, ‘amyloidoma’ and ‘amyloid tumor’ and
search terms (renal pelvis) and (amyloidoma or amyloid tumor) in
PubMed (National Center for Biotechnology Information, U.S.
National Library of Medicine, Bethesda, MD, USA), a literature
search was performed and only 26 cases of primary amyloidomas of
the renal pelvis were identified (Table
I) (1–23). Primary localized amyloidoma may
present as hematuria and lumbago (14). A primary localized amyloidoma of the
renal pelvis consists of amyloid deposits that may present as
malignant tumors (15). The present
study reports the rare case of a patient with amyloidoma that was
confined to the renal pelvis, and the patient exhibited similar
symptoms to those of upper urinary tract transitional cell
carcinoma (TCC). In addition, 26 cases of patients with primary
amyloidoma of the renal pelvis identified from the literature were
also reviewed. Nephrectomy was the most selected treatment in the
reported cases. The majority of patients achieved long time disease
free survival and good prognosis. (7). The clinical and pathological features of
the cases were discussed, in particular, the treatment methods and
prognosis.
 | Table I.Review of the reported cases of
primary localized amyloidoma of the renal pelvis. |
Table I.
Review of the reported cases of
primary localized amyloidoma of the renal pelvis.
| First author, year
(Ref.) | Gender | Age, years | Symptoms or clinical
finding | Medical history | Treatment | Outcome |
|---|
| Akimoto, 1927
(22) | NA | NA | NA | NA | NA | NA |
| Gilbert et al,
1952 (1) | F | 52 | Flank pain | NA | Nephrectomy | NA |
| Sato, 1957 (23) | M | 37 | Hematuria and flank
pain | None | Nephrectomy | NA |
| Chisholm et
al, 1967 (2) | M | 66 | Painless
hematuria | None | Nephrectomy | Succumbed to renal
failure following a short period of time |
| Chisholm et
al, 1967 (2) | F | 58 | Iron-deficiency
anemia and mild azotemia | None | Nephrostomy | Alive with no
evidence of disease |
| Gardner et al,
1971 (3) | M | 39 | Left flank pain and
rust-colored urine | None | Biopsy of renal
pelvis | Alive with no
evidence of disease |
| Ullmann, 1973
(4) | F | 58 | Hematuria and flank
pain | NA | Nephrectomy | NA |
| Dias et al,
1979 (5) | F | 67 | Painless gross
hematuria | Left hemicolectomy
for carcinoma of the sigmoid colon | Nephrectomy/partial
ureterectomy | Succumbed to unknown
causes 3 years later |
| Gelbard et al,
1980 (6) | M | 67 | Left flank pain and
gross hematuria | Cardiovascular
accident incurred during a total hip replacement for
osteoarthritis | Radical
nephrectomy | NA |
| Fujibara et
al, 1981 (7) | M | 66 | Hematuria | N.A | Nephrectomy | NA |
| Fox et al,
1984 (8) | M | 81 | Painless
hematuria | None |
Nephroureterectomy | NA |
| Murphy et al,
1986 (9) | F | 67 | Hematuria and left
flank pain | Tuberculosis of the
chest, spine and right breast |
Nephroureterectomy | NA |
| Davis et al,
1987 (10) | M | 58 | Intermittent gross
hematuria | None |
Nephroureterectomy | Alive with no
evidence of disease 5 years later |
| Sparwasser et
al, 1991 (11) | M | 81 | Hematuria | Contusion of the left
kidney and labile hypertension | Nephrectomy/proximal
ureterectomy | Alive with no
evidence of disease 5 years later |
| Shiramizu et
al, 1992 (12) | F | 63 | Left flank pain and
gross hematuria | None |
Nephroureterectomy | Alive with no
evidence of disease |
| German, 1994
(13) | M | 64 | Diarrhea, vomiting
and urinary frequency | None | Amyloid material
cleared by laparotomy | Obstruction and
perforation at the pelvi-ureteric junction by sharp calculus
Succumbed to pneumonia 8 months later |
| Tsuji et al,
1994 (19) | F | 47 | Intermittent gross
hematuria and right flank pain | Right
mastectomy | Ieal ureter | Alive with no
evidence of disease 2 years later |
| Merrimen et
al, 2006 (14) | F | 51 | Flank pain, fever
and gross hematuria | None | Nephrectomy | NA |
| Borza et al,
2010 (15) | M | 58 | Gross, painless
hematuria and right flank pain | None | Active
surveillance | No clinical or
radiographical signs of progressive disease 6 years later |
| Pan et al,
2011 (16) | M | 70 | None | Partial nephrectomy
of the right kidney for an angiomyolipoma 4 years prior | Active
surveillance | Recurrence in the
unilateral bladder and ureter |
| Monge et al,
2011 (17) | M | 68 | Gross hematuria and
renal colic | None | Nephrectomy,
repeated, resections double J stent | No recurrence. Only
mild renal insufficiency remained 5 years later |
| Paidy et al,
2012 (20) | F | 72 | Gross hematuria and
right flank pain | Nephrolithiasis,
hypertension, osteoarthritis stroke, transient ischemic attack,
atrial fibrillation and hypercholesterolemia | Nephrectomy | NA |
| Zhou et al,
2014 (21) | F | 77 | Gross
hematuria | None | Nephrectomy | Alive with no
evidence of disease 12 years later |
| Zhou et al,
2014 (21) | M | 71 | Gross
hematuria | None | Nephrectomy | Alive with no
evidence of disease 6 years later |
| Grigor, 2015
(18) | F | 60 | Gross hematuria
intraepithelial | Supraventricular
tachycardia, neoplasia. Retinal detachment, macular hole and
cervical lattice degeneration in right eye | Laparoscopic
nephrectomy | Alive with no
evidence of disease 30 months later, but diagnosed with breast
cancer 21 months ago |
| Present study | M | 56 | Gross
hematuria | Kidney calculi | Nephrectomy | Alive with no
evidence of disease 4 months later |
Case report
A 56-year-old man presented to the Department of
Urology, Sun-Yat Sen University Cancer Center (Guangzhou, China)
with left flank pain, symptoms of urinary irritation and
intermittent gross hematuria. The patient had experienced the
symptoms for 6 years; however, in the month prior to presentation,
the symptoms had become worse. Ultrasonography revealed a mass with
a low-intensity heterogeneous pattern that measured 55×19 mm in
size and obstructed the lumen of the renal pelvis. Dilatation of
the renal pelvis was located in the left kidney (Fig. 1). A preliminary diagnosis of TCC of
the renal pelvis was suggested based on sonography, and therefore,
a nephroureterectomy was advised. However, 5 urinary cytology tests
were negative and pre-operative examinations revealed no abnormal
signs, such as abdominal tenderness or rebound pain, during
physical examination. Blood tests yielded the following results:
Urine protein, 2+; urine red blood cell count, >3 cells/high
power field; urine erythrocytes, 932 µl/l; left renal glomerular
fitration rate, 18 ml/min; right renal glomerular fitration rate,
64ml/min; and the serum creatinine levels, eosinophil numbers and
basophil numbers were within the normal ranges. The patient had
been a smoker for ~20 years and had suffered from nephrolithiasis
for 6 years. The patient possessed no known drug allergies.
Subsequently, the patient agreed to undergo a
nephroureterectomy.
Following surgery, the excised mass underwent
additional tests. Macroscopically, the surgical specimen revealed
tumors located in the renal pelvis. No clear difference in the
ureter was observed. A cut section of the tumor revealed a
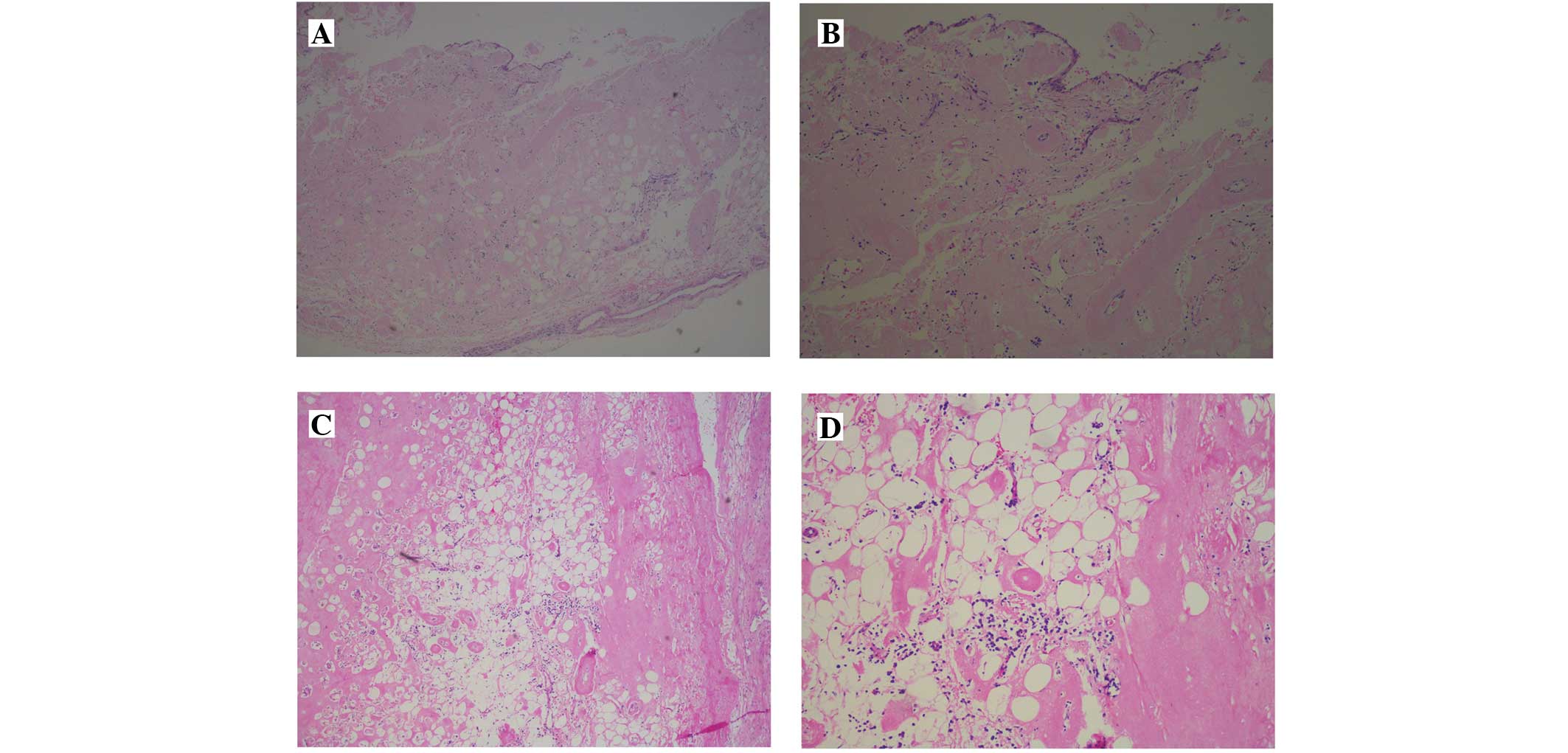
red-yellow surface with firm regions. Microscopically,
histopathological studies revealed that the tumor consisted of
massive diffuse deposits of amyloid and microscopic, eosinophilic,
amorphous material (Fig. 2) and an
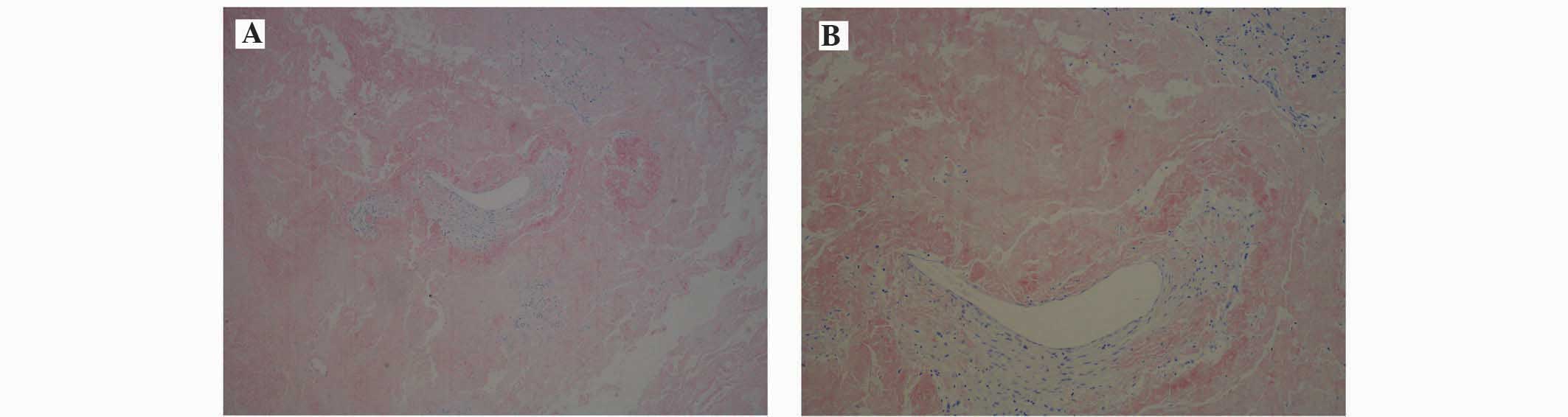
absence of neoplastic cells. The tumor stained positive for Congo
red (Fig. 3), which indicates the
presence of material that is retained following potassium
permanganate digestion. A final diagnosis of amyloid light
chain-type amyloidoma of the renal pelvis was determined. The
patient received regular surveillance and was alive with no
evidence of disease 5 months later.
Written informed consent was obtained from the
patient for the publication of the present study.
Discussion
Amyloidosis refers to a large heterogeneous group of
diseases that is characterized by extracellular deposits of amyloid
in individual organs or tissue. Amyloid is an amorphous, insoluble
and proteinaceous material (17).
Extracellular amyloidosis consists of specific protein fibrils
(24). Amyloidosis can be classified
into 4 groups, consisting of primary, secondary, heredofamilial and
β2-microglobulin-associated amyloidosis. This disease may be
additionally classified as localized amyloidosis, which involves a
single organ, or systemic amyloidosis, which involves multiple
organs and is the most common classification among reported cases
(6). By contrast, localized
amyloidosis occurs much less frequently. (15) Systemic amyloidosis may be primary,
progressive and fatal. Primary amyloidosis is commonly associated
with an underlying immune dyscrasia, such as multiple myeloma and
Waldenstrom's macroglobulinemia (15).
The etiology of primary localized urinary
amyloidosis remains unknown; however, it may be possible that
amyloid deposits are produced locally, or the submucosa of the
genitourinary tract may be targeted by light-chains that are
produced elsewhere. Numerous studies support the first hypothesis,
as there is an absence of a monoclonal plasma component. An
additional hypothesis is that protein deposits in bladder
non-amyloid associated (AA) localized amyloidosis consist of the
immunoglobulin λ light-chain subgroup I or IV (17).
Furthermore, non-AA localized amyloidosis has been
described in the lung (25), nervous
system (26), skin (24), larynx (27), intestinal tract (28) and genitourinary tract (17). Using PubMed, a literature search was
performed and only 26 cases of primary amyloidomas of the renal
pelvis were identified. The inclusion and exclusion criteria is
whether primary localized amyloidoma. The majority of reported
cases concerned with localized urinary tract amyloidosis are
characterized as primary type, but secondary localized amyloidosis
has been reported without a chronic systemic inflammatory state.
Renal pelvis primary localized amyloidoma is an extremely rare
condition, and is notable due to its clinical presentation and
radiographic appearance, which mimics that of transitional cell
carcinoma. In a review of the English and French literature by
Monge et al (17), 169 cases
of genitourinary tract localized amyloidoma were reported over the
past 100 years. The renal pelvis was the most rare location
identified, accounting for ~6% of the 169 cases, which was lower
than the number located in the bladder, ureter and urethra. To the
best of our knowledge, only 26 cases of renal pelvis primary
localized amyloidoma have been reported (1–23).
Positive staining for Congo red is used to diagnose
primary localized amyloidoma. In order to exclude AA-type
amyloidosis, screening by pre-exposure of tissue slides to
KMnO4 stain is performed, since false-negative results
may be obtained using immunohistochemistry (negative for Congo red)
(17). Clinical symptoms of primary
localized amyloidoma of the renal pelvis typically present as gross
hematuria, flank pain and urinary irritative symptoms, which mimic
the symptoms of inflammation and neoplasm (21). It is challenging to distinguish
between amyloidoma and upper urinary tract TCC solely from
radiological findings, which may be non-specific (17). In addition, urine cytology does little
to contribute to the diagnosis, since the majority of amyloid
deposits are subepithelial. Consequently, to avoid misdiagnosis,
upper urinary tract tumors should be evaluated microscopically by
ureteroscopic biopsy when multiple urine cytology analyses are
negative, or if possible, by surgical biopsy using frozen tissue
sections examined prior to radical resection.
Primary localized amyloidoma possesses a relatively
good prognosis in the genitourinary tract and other organ systems.
Recurrence and implantation of the tumor has not been identified in
reported cases. Nephrectomy was the chosen treatment in the present
study, and is used in the majority of reported cases. However, by
monitoring the progression of the primary localized amyloid tumor
in the renal pelvis, using active surveillance with serial
imageological examination, a similar outcome to nephrectomy may be
observed (15). This should be
considered by all urologists.
Primary localized amyloidoma is extremely rare in
the renal pelvis (14,15). Consequently, there is a lack of
standardized clinical symptoms and specific laboratory tests, and
in addition, imageological examination mimics TCC. A pre-operative
ureteroscopic biopsy or surgical biopsy is required when multiple
urinary cytology analyses are not positive or a benign tumor,
including primary localized amyloidoma, is suspected, to avoid an
unnecessary nephroureterectomy. Early radical surgery is not
required unless there is no renal function or a severe urinary
tract obstruction. Instead, active surveillance with serial
imageological examination may be used to monitor the progression of
the lesion. In conclusion, primary localized amyloidoma of renal
pelvis is a benign and rare tumor, which has a relatively good
prognosis.
References
|
1
|
Gilbert LW and McDonald JR: Primary
amyloidosis of the renal pelvis and ureter: Report of case. J Urol.
68:137–139. 1952.PubMed/NCBI
|
|
2
|
Chisholm GD, Cooter NB and Dawson JM:
Primary amyloidosis of the renal pelvis. BMJ. 1:736–738. 1967.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gardner KD Jr, Castellino RA, Kempson R,
Young BW and Stamey TA: Primary amyloidosis of the renal pelvis. N
Engl J Med. 284:1196–1198. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ullmann AS: Primary amyloidosis of the
renal pelvis: A case report and review of literature. Mich Med.
72:29–33. 1973.PubMed/NCBI
|
|
5
|
Dias R, Fernandes M and Patel RC: deS
hadarevian JJ and Lavengood RW: Amyloidosis of renal pelvis and
urinary bladder. Urology. 14:401–404. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gelbard M and Johnson S: Primary
amyloidosis of renal pelvis and renal cortical adenoma. Urology.
15:614–617. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fujihara S and Glenner GG: Primary
localized amyloidosis of the genitourinary tract:
Immunohistochemical study on eleven cases. Lab Invest. 44:55–60.
1981.PubMed/NCBI
|
|
8
|
Fox M, Hammond JC, Knox R and Underwood
JC: Localised primary amyloidosis of the renal pelvis. Br J Urol.
56:223–224. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Murphy MN, Alguacil-Garcia A and MacDonald
RG: Primary amyloidosis of renal pelvis with duplicate collecting
system. Urology. 27:470–473. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Davis PS, Babaria A, March DE and Goldberg
RD: Primary amyloidosis of the ureter and renal pelvis. Urol
Radiol. 9:158–160. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sparwasser C, Gilbert P, Mohr W and Linke
RP: Unilateral extended amyloidosis of the renal pelvis and ureter,
A case report. Urol Int. 46:208–210. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shiramizu M, Nakamura K, Baba S, Katsuoka
Y and Kinoshita H: Primary localized amyloidosis of the renal
pelvis coexisting with transitional cell carcinoma, A case report.
Hinyokika Kiyo. 38:699–702. 1992.PubMed/NCBI
|
|
13
|
German KA and Morgan RJ: Primary
amyloidosis of the renal pelvis and upper ureter. Br J Urol.
73:99–100. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Merrimen JL, Alkhudair WK and Gupta R:
Localized amyloidosis of the urinary tract, Case series of nine
patients. Urology. 67:904–909. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Borza T, Shah RB, Faerber GJ and Wolf JS
Jr: Localized amyloidosis of the upper urinary, tract. A case
series of three patients managed with reconstructive surgery or
surveillance. J Endourol. 24:641–644. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pan DL and Na YQ: Amyloidosis of the
unilateral renal pelvis ureter and urinary bladder: A case report.
Chin Med Sci J. 26:197–200. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Monge M, Chauveau D, Cordonnier C, Noël
LH, Presne C, Makdassi R, Jauréguy M, Lecaque C, Renou M, Grünfeld
JP, et al: Localized amyloidosis of the genitourinary tract: Report
of 5 new cases and review of the literature. Medicine (Baltimore).
90:212–222. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Grigor T and Munro N: Amyloidosis of the
renal pelvis: A harbinger of mammary carcinoma? BMJ Case Rep.
16:20152015.
|
|
19
|
Tsuji Y, Michinaga S and Ariyoshi A: Ileal
ureter, Another option for the treatment of localized amyloidosis
of the upper urinary tract. J Urol. 151:999–1000. 1994.PubMed/NCBI
|
|
20
|
Paidy S, Unold D and Catanzano TM: AIRP
best cases in radiologic-pathologic correlation, localized
amyloidosis of the renal pelvis. Histopathology. Inc. 32:2025–2030.
2012.
|
|
21
|
Zhou F, Lee P, Zhou M, Melamed J and Deng
FM: Primary localized amyloidosis of the urinary tract frequently
mimics neoplasia, A clinicopathologic analysis of 11 cases. Am J
Clin Exp Urol. 2:71–75. 2014.PubMed/NCBI
|
|
22
|
Akimoto K: Ober amyloidartigeE
iweissniederschlage im Nierenbecken. Beitr Pathol Anat.
78:2391927.
|
|
23
|
Sato S: Primary amyloidosis of the renal
pelvis and ureter: R eport of a case. Acta Med Biol. 5:151957.
|
|
24
|
Reitboeck JG, Feldmann R, Loader D, Breier
F and Steiner A: Primary cutaneous amyloidoma, A case report. Case
Rep Dermatol. 6:264–267. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Dong MJ, Zhao K, Liu ZF, Wang GL and Yang
J: Primary pulmonary amyloidosis misdiagnosed as malignancy on
dual-time-point fluoro-deoxyglucose positron emission
tomography/computed tomography, A case report and review of the
literature. Oncol Lett. 9:591–594. 2015.PubMed/NCBI
|
|
26
|
Apostolova LG, Hwang KS, Avila D, Elashoff
D, Kohannim O, Teng E, Sokolow S, Jack CR, Jagust WJ, Shaw L, et
al: Alzheimer's Disease Neuroimaging Initiative: Brain amyloidosis
ascertainment from cognitive, imaging, and peripheral blood protein
measures. Neurology. 84:729–737. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheng KJ, Wang SQ and Lin S: Localized
amyloidosis concurrently involving the nasopharynx, larynx and
nasal cavities, A case report. Zhonghua Er Bi Yan Hou Tou Jing Wai
Ke Za Zhi. 44:875–876. 2009.(In Chinese). PubMed/NCBI
|
|
28
|
Yaita H, Nakamura S, Kurahara K, Nagasue
T, Kochi S, Oshiro Y, Ohshima K, Ikeda Y and Fuchigami T: Primary
small-bowel adult T-cell leukemia/lymphoma with gastric AL
amyloidosis. Endoscopy. 46:E613–614. 2014.
|