Introduction
Desmoplastic fibroma, alternatively known as
aggressive fibromatosis or desmoid tumors, was initially described
by MacFarlane in 1832. The annual incidence of desmoplastic fibroma
is 2–4 per 1 million individuals, worldwide (1). Clinically, it presents as a monoclonal
fibroblastic proliferation arising in musculoaponeurotic structures
(2,3).
Magnetic resonance imaging (MRI) is typically used to determine the
extent of the tumor and histological analysis is the gold standard
for diagnosis. Desmoplastic fibroma can be treated with surgery,
radiotherapy or pharmacological agents (1–3). The
disease occurs in the form of benign locally aggressive tumors that
possess a high rate of recurrence. Desmoplastic fibroma of the bone
is rare, and the most common site of occurrence is the jaw,
followed by the pelvis and long bones. The forearm bones are rarely
involved, however, the development of desmoplastic fibroma
following a bone fracture has been previously reported. The
majority of studies recommend surgical treatment with a wide free
margin resection, followed by reconstruction of the bony defect
with a fibular graft (4–7).
The current study presents a case of desmoplastic
fibroma in the distal forearm treated by wide resection and
reconstructive surgery during the resection procedure. The patient
experienced recurrence three times and underwent four resections
during the subsequent 3 years following the initial resection.
After 10 years of follow-up, the patient's functional recovery
remains positive. The present case indicated that repeated
recurrences of limb desmoplastic fibroma are not an absolute
contraindication for restoration of function, however, frequent
follow-up is necessary. Written informed consent was obtained from
the patient.
Case report
In October 1999, a 23-year-old man presented at
Huashan Hospital, Fudan University (Shanghai, China) with a 2-year
history of a progressively swelling tumor in the right forearm
following spraining of the right wrist when playing basketball. The
patient attended a local hospital (Cixi City, China) for
conservative treatment after spraining in 1997. Upon presentation
to our hospital, local examination revealed an 8×5-cm solid mass
over the palmar and ulnar aspects of the wrist, with an unclear
boundary and superficial varicose veins. The overlying skin was
higher than normal. The patient demonstrated a full range of motion
of the wrist and hand joints. Plain radiograph revealed expansive
osteolytic growth involving the right distal radius, and a giant
cell tumor of the bone. MRI was performed. Imaging assessment
revealed a soft-tissue mass involving the right distal radius,
which appeared to be a benign giant cell tumor; however, the
possibility of malignancy could not be excluded.
A wide surgical resection of the tumor was
performed. The solid mass originated from the distal radius. On
gross examination, the encapsulated tumor measured 6×5×3.5 cm. The
tumor was excised with the involved radiocarpal joint and ulnar
periosteum, proximally up to ~8 cm from the wrist joint.
Reconstruction of the bony defect was performed using an autologous
vascularized fibular graft. Fibular head and diaphysis measuring 8
cm were harvested from the ipsilateral leg. The head of the fibula
was fitted to match the remaining radiocarpal joint in order to
recreate the wrist joint. Distally, the fibular diaphysis was fixed
with a radius shaft by a dynamic compression plate in order to
reconstruct the forearm and wrist joint. Vessel anastomosis was
performed during this procedure, with the dorsal branch of the
radial artery anastomosing to the knee arteries and the
accompanying vein to the head vein. A biopsy was performed
following tumor resection, which resulted in a diagnosis of
desmoplastic fibroma. Histologically, the hematoxylin and eosin
stained specimen resembled low-grade fibrosarcoma, with banal
fibroblasts infiltrating the adjacent tissue in fascicles, without
mitosis.
During the 3 years immediately after the tumor
resection, the patient experienced recurrence three times,
involving the distal ulnar, proximal radius and soft tissue of the
dorsal region of the distal forearm, respectively. An additional
resection was performed following each recurrence, as well as
functional reconstruction following the second and third
recurrences. The proximal ulnar and distal radius were fixed by a
dynamic compression plate to maintain the length of the forearm,
and thumb extension restoration was conducted in order to
compensate for the involved extensor hallucis muscle.
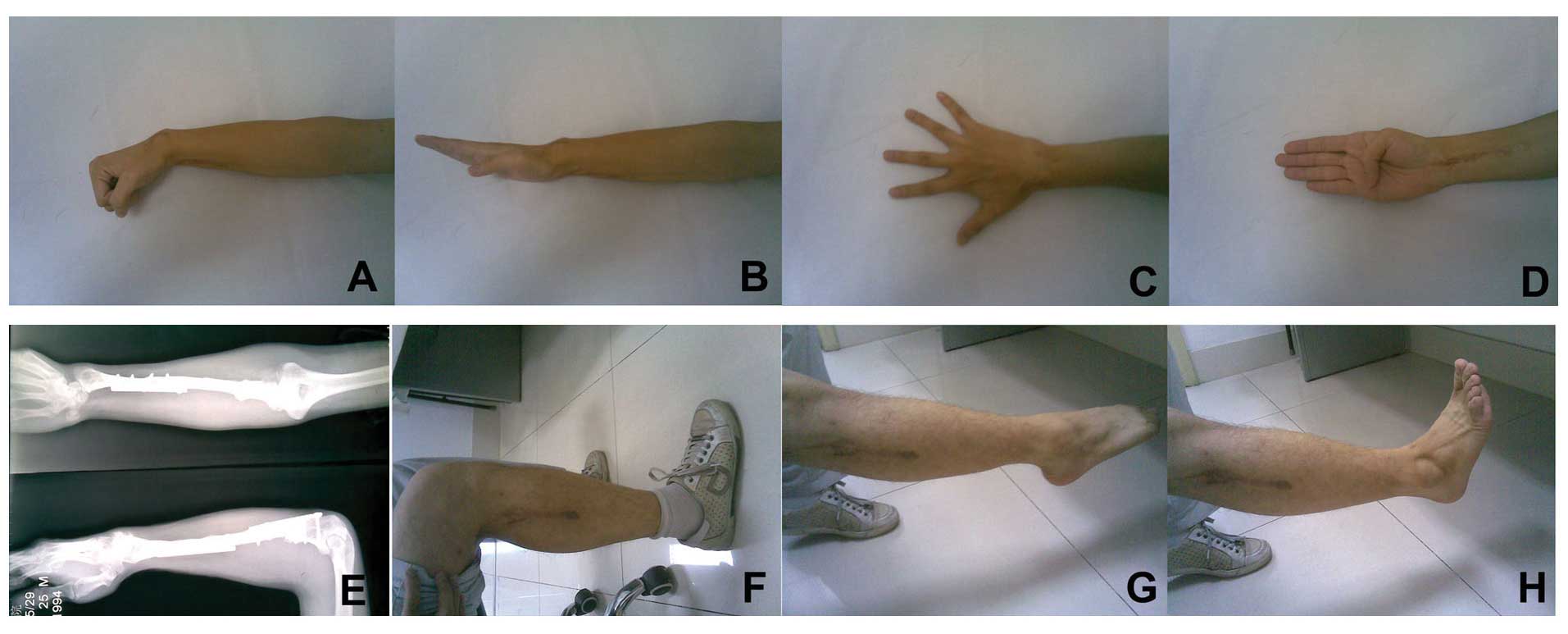
Subsequent to 10 years of follow-up, the patient
achieved 45-5° flexion-extension of the wrist, and 90–70°
pronation-supination and 100-0° flexion-extension of the elbow. The
function of the fingers, and the knee and ankle joints was
unlimited (Fig. 1).
The patient returned to work, and at that time, MRI
revealed no signs of tumor recurrence. In this case, the prognosis
was very good and the patient was advised to return every 2 years
for further follow-up. However, the patient chose not to
return.
Discussion
Desmoplastic fibroma of the bone has been generally
defined as a benign tumor that exhibits malignant behavior
(8–11). The etiology of desmoplastic fibroma
remains to be elucidated. A wide range of factors, including
genetic predisposition, estrogen stimulation and traumatic
activation, such as fractures and surgery, have been implicated in
the development of aggressive fibromatosis (12,13). In
the present case, the patient had a history of wrist sprains and
had undergone several surgeries, therefore, an association between
wrist trauma and tumor growth was suspected, in addition to an
association between surgical resections and recurrence.
Due to this locally aggressive behavior, the
majority of studies recommend a wide local surgical excision via
the normal soft tissue (14–21). The recurrence rate has been reported
to be 17% following resection, and may be as high as 55% following
curettage (22). In the present case,
the patient experienced three further recurrences and underwent
four resections.
Wide surgical resection and a high grade of
recurrence may result in significant dysfunction of the affected
area. Various options have been reported in the relevant literature
concerning the functional reconstruction of bone defects in the
forearm, including creation of a single forearm bone from the
radius and ulna, and centralizing the carpus over the single bone,
a free fibular graft, a fibular head graft for the distal radius
and a microvascular fibular graft, and allografts (4–7). The
technique utilized in the present study to create the articular
surface of the radiocarpal joint involved a microvascular fibular
head graft. In a total of three surgical procedures, a single bone
forearm was created from the radius and ulna, and the carpus was
centralized over the single bone. Although a normal forearm could
not be achieved, this reconstruction was an acceptable option
considering the morbidity of tumor resection for forearm
functioning.
The long-term outcome for patients exhibiting
extremity desmoid tumors remains to be elucidated, particularly for
patients who experience repeated recurrences. In the present case,
the patient experienced recurrence three times in the three years
immediately after the initial surgical resection, and after 10
years of follow-up, the patient demonstrated positive hand, elbow,
knee and ankle function, as well as moderate wrist function. The
patient was satisfied with the recovery of function and was able to
return to work and daily life with no limitations.
In conclusion, the present study indicates that
desmoplastic fibroma is a rare tumor that exhibits locally
aggressive behavior. The diagnosis is dependent on the correlation
of clinico-radio-pathological data. The treatment of choice is a
wide local excision and function reconstruction for the upper
limbs.
Acknowledgements
The present study was sponsored by the Scientific
Research project supported by Huashan Hospital, Fudan University
(Shanghai, China; grant no. No.2013QD05)
References
|
1
|
Spear MA, Jennings LC, Mankin HJ, Spiro
IJ, Springfield DS, Gebhardt MC, Rosenberg AE, Efird JT and Suit
HD: Individualizing management of aggressive fibromatoses. Int J
Radiat Oncol Biol Phys. 40:637–645. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zlotecki RA, Scarborough MT, Morris CG,
Berrey BH, Lind DS, Enneking WF and Marcus RB Jr: External beam
radiotherapy for primary and adjuvant management of aggressive
fibromatosis. Int J Radiat Oncol Biol Phys. 54:177–181. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ballo MT, Zagars GK, Pollack A, Pisters PW
and Pollack RA: Desmoid tumor: Prognostic factors and outcome after
surgery, radiation therapy, or combined surgery and radiation
therapy. J Clin Oncol. 17:158–167. 1999.PubMed/NCBI
|
|
4
|
Gebhardt MC, Campbell CJ, Schiller AL and
Mankin HJ: Desmoplastic fibroma of bone. A report of eight cases
and review of the literature. J Bone Joint Surg Am. 67:732–747.
1985.PubMed/NCBI
|
|
5
|
Kesani AK, Tuy B, Beebe K, Patterson F and
Benevenia J: Single-bone forearm reconstruction for malignant and
aggressive tumors. Clin Orthop Relat Res. 464:210–216.
2007.PubMed/NCBI
|
|
6
|
Muramatsu K, Ihara K, Azuma E, Orui R,
Goto Y, Shigetomi M and Doi K: Free vascularized fibula grafting
for reconstruction of the wrist following wide tumor excision.
Microsurgery. 25:101–106. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rastogi S, Varshney MK, Trikha V, Khan SA
and Mittal R: Desmoplastic fibroma: A report of three cases at
unusual locations. Joint Bone Spine. 75:222–225. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hattoma N, Largab A, Kafih M, Rafai M,
Maher N and Trafeh M: Desmoid tumors of the shoulder-girdle (report
of three cases). Chir Main. 23:184–189. 2004.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Berthe JV, Loréa P, De Prez C and De Mey
A: A case report of desmoid tumor of the finger. Chir Main.
22:312–314. 2003.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Reitamo JJ: The desmoid tumor. IV. Choice
of treatment, results, and complications. Arch Surg. 118:1318–1322.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Enzinger FM and Shiraki M:
Musculo-aponeurotic fibromatosis of the shoulder girdle
(extra-abdominal desmoid). Analysis of thirty cases followed up for
ten or more years. Cancer. 20:1131–1140. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gallucci GL, Boretto JG and De Carli P:
Desmoid tumor of the forearm. Reconstructive surgery and functional
result. Chir Main. 28:326–329. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsai LH, Thamboo TP and Lim AY: Desmoid
tumour following a distal radius fracture - a complication or a
coincidence? J Hand Surg Eur Vol. 32:330–332. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wood TJ, Quinn KM, Farrokhyar F, Deheshi
B, Corbett T and Ghert MA: Local control of extra-abdominal desmoid
tumors: Systematic review and meta-analysis. Rare Tumors. 5:e22013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rock MG, Pritchard DJ, Reiman HM, Soule EH
and Brewster RC: Extra-abdominal desmoid tumors. J Bone Joint Surg
Am. 66:1369–1374. 1984.PubMed/NCBI
|
|
16
|
Ridders J, Ernst A, Todt I and Seidl RO:
Extra-abdominal desmoid tumors. Case report and literature review.
HNO. 53:639–644. 2005.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pritchard DJ, Nascimento AG and Petersen
IA: Local control of extra-abdominal desmoid tumors. J Bone Joint
Surg Am. 78:848–854. 1996.PubMed/NCBI
|
|
18
|
Mankin HJ, Hornicek FJ and Springfield DS:
Extra-abdominal desmoid tumors: A report of 234 cases. J Surg
Oncol. 102:380–384. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chatelard PA, Gilly FN, Carret JP,
Vauzelle JL, Brunat M, Braillon G and Dejour H: Extra-abdominal
desmoid tumors. Therapeutic indications. Apropos of 28 cases. Acta
Orthop Belg. 57:227–233. 1991.(In French). PubMed/NCBI
|
|
20
|
Barrios RH, Leyes M, Losada JI, Schweitzer
D and Amillo S: Extra-abdominal desmoid tumors.
Diagnostic-therapeutic considerations and review of the literature.
Rev Med Univ Navarra. 39:14–20. 1995.(In Spanish). PubMed/NCBI
|
|
21
|
Ayadi K, Trigui M, Zribi M and Keskes H:
Extra-abdominal desmoid tumors: 7-year outcome after surgical
treatment in 12 patients. Rev Chir Orthop Reparatrice Appar Mot.
89:385–392. 2003.(In French). PubMed/NCBI
|
|
22
|
Böhm P, Kröber S, Greschniok A, Laniado M
and Kaiserling E: Desmoplastic fibroma of the bone. A report of two
patients, review of the literature, and therapeutic implications.
Cancer. 78:1011–1023. 1996. View Article : Google Scholar : PubMed/NCBI
|