Introduction
Inflammatory myofibroblastic tumors (IMTs),
originally termed as inflammatory pseudotumors, are rare neoplastic
lesions with a tendency for locally aggressive behavior and
recurrence (1,2). Due to the rarity of IMTs, only a few
cases have been reported in the literature to date (2–17), and the
incidence rates remain unclear. IMTs are most prevalent in the
pulmonary system of children and young adults, however, they may
also develop in older patients and in other organs (18). Symptoms are non-specific and typically
depend on the location of the tumor (3), therefore, diagnosis is difficult. IMTs
are most commonly diagnosed via ultrasound, abdominal computed
tomography (CT) or magnetic resonance imaging (18). Radical resection is the treatment of
choice for patients with IMT (2).
Prognostic factors for the disease remain unclear, however,
survival is good in the majority of patients, with a five-year
survival rate of ~87% (4). The
current study describes a case of jejunal IMTs presenting in a
42-year-old woman. Following a review of the appropriate
literature, the clinical and pathological features of this rare
tumor, and the controversies of diagnostic and treatment tactics
are discussed.
Case report
In August 2014, a 42-year-old female was admitted to
the Department of General and Abdominal Oncological Surgery of the
National Cancer Institute (Vilnius, Lithuania), presenting with
intermittent abdominal pain that had begun 11 months previously.
The symptoms had become more intense and painful the month prior to
admittance.
At the time of admittance, the vital signs of the
patient were stable, with no vomiting, distention of the abdomen,
palpable abdominal masses, palpable local or distant lymph nodes,
or malnutrition. The abdomen was mildly tender on palpation in all
quadrants, particularly surrounding the umbilical area. Peritoneal
signs were negative, and a chest X-ray, laboratory tests and
electrocardiogram exhibited no pathological changes or
abnormalities. During gastroscopy, a mucosal inflammatory reaction
with a few superficial erosions and without signs of bleeding, was
observed in the distal end of the esophagus. Following consultation
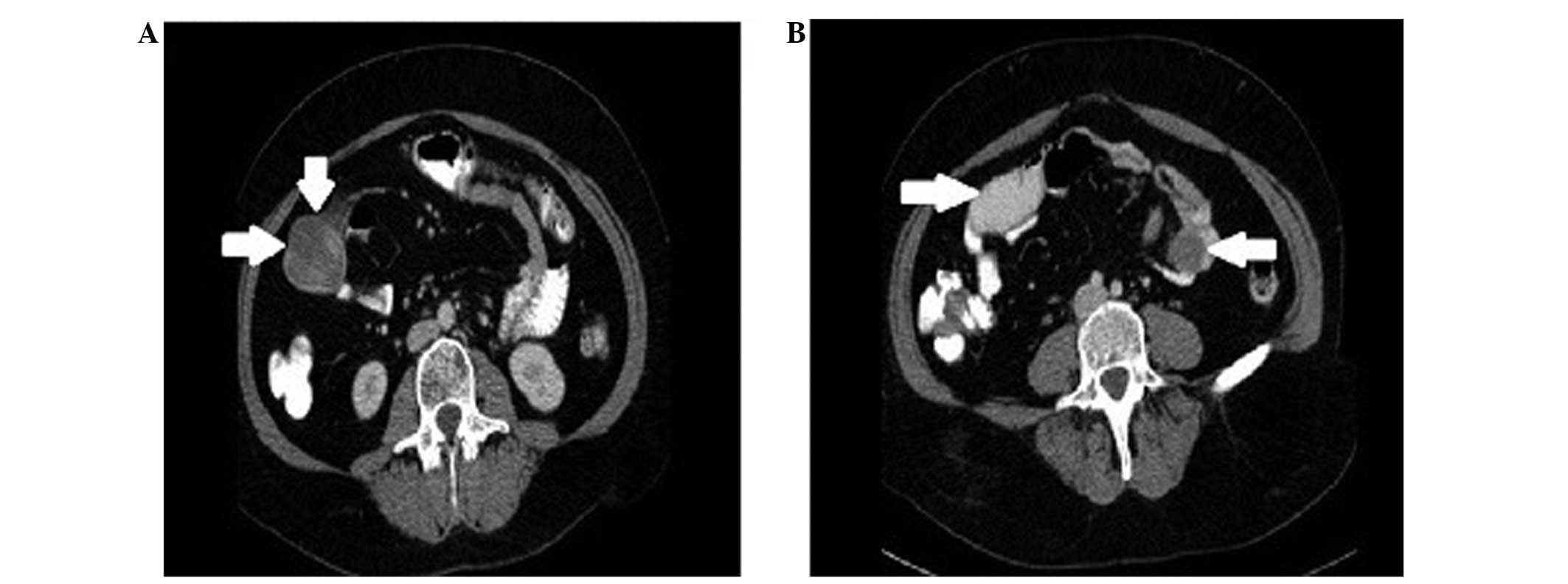
with a general surgeon, an abdominal CT scan was obtained. The scan
demonstrated that, at the L4 level, two solid cystic structures
existed: The first mass was 51 mm in diameter and was present on
the right side of the patient, whilst the other mass was 30 mm in
diameter and was present on the left side of the patient. The two
masses were in close association with the small bowel wall
(Fig. 1).
A laparotomy was performed and a ~30-cm specimen of
the jejunum, which presented with 3 separate solid exophytic tumors
and bowel invagination, was removed. A side-to-side anastomosis was
also performed. No other peritoneal cavity changes were observed.
The post-surgical recovery was uneventful and the patient was
discharged on the 10th day post-surgery.
The specimen that had been removed during the
laparotomy was 34 cm in length and presented with 3 separate
exophytic tumors of the small bowel wall. A small bowel
intussusception was confirmed, with 4 lymph nodes observed in the
mesentery. Under microscopic analysis, resection margins were clear
of neoplastic tissue and the lymph nodes were without metastases.
Immunohistochemical investigation demonstrated a positive reaction
of 10% cancer cells to Ki-67 and a 90% positive cytoplasmic
reaction, whilst negative reactions were exhibited for estrogen
receptors, pan cytokeratin, cluster of differentiation (CD)10,
melan A, human melanoma black 45, S100, CD117, CD21, CD23, CD31,
CD34, activin receptor-like kinase, anaplastic lymphoma kinase
(ALK), desmin, myogenic differentiation 1 and myogenin.
The patient remains asymptomatic following 6 months
of follow-up, without any evidence of recurrent disease. Full
written informed consent was obtained from the patient for
publication of this case study.
Discussion
IMTs are rare, distinctive lesions of unknown
etiology (5) that were first
described by Dr H. Brunn in 1939 (6).
Previously, IMTs have been referred to by various names, including
plasma cell granuloma, myofibroblastoma, pseudosarcomatous
myofibroblastic proliferation, inflammatory myofibrohistiocytic
proliferation, xanthomatous pseudotumor, and most commonly,
inflammatory pseudotumor (5). This
confusion in nomenclature is believed to have arisen due its
unknown etiology. Argument has arisen over whether it is a true
neoplasm or a reactive process (7).
IMTs are locally recurrent, however, they rarely metastasize (~5%
of cases). The most common sites of metastasis are the lungs and
brain, followed by the liver and bones (8). It has been proposed that the
inflammatory reaction may occur as a result of surgery, trauma or
infections implicating the Epstein-Barr virus, human herpes virus
type 8 (9). However, with the
improvement of molecular techniques, it has been identified that a
subset of these tumors are neoplastic in nature, harboring
translocations of the ALK gene (3).
The histopathological features that are associated
with the aggressive behavior of IMTs remain undetermined, although
the presence of cellular atypia, ganglion-like cells, increased
mitotic figures, multinodularity, DNA aneuploidy, an elevated Ki-67
proliferative index and overexpression of oncogenic proteins,
including ALK, p53 and B-cell lymphoma 2, may identify a subset of
tumors that have the potential for recurrence or malignant
transformation (10). In the case
described by the present study, cellular atypia and multinodularity
were observed with ALK-negative IMT, demonstrating the increased
risk of metastases in the patient. Despite this, IMT metastasis was
not observed, and mitotic figures and Ki-67 proliferative activity
were low. Coffin et al (11,12)
demonstrated that ALK-positive IMTs were diagnosed in younger
patients and had a tendency to recur. By contrast, ALK-negative
IMTs were associated with the presence of metastases. The study
concluded that ALK reactivity may be a favorable prognostic
indicator in IMT and that abdominopelvic IMTs recur more
frequently.
In the current literature, IMTs have been
established as distinct entities by the World Health Organization,
being classified as tumors of intermediate biological potential due
to a tendency for local recurrence and the small risk for distant
metastasis (13). Three basic
histological patterns have been described: i) fibrous
histocytoma-like; ii) granulomatous; and iii) sclerosing. In the
present case, the tumor was categorized as the first type.
IMTs are most typically observed in children and
young adults, with the lungs presenting as the most commonly
affected site; however, it has been recognized that any anatomical
location may be involved (14). In
present case, the tumor arose from the proximal jejunum. This tumor
location appears to be particularly rare, with only one other adult
female case identified in the literature (15). This patient presented clinically with
non-specific symptoms of IMT, including acute abdomen and fever
with anaemia, with later complications that included septic shock
and jaundice. CT indicated a left adnexal mass and intra-operative
findings suggested an inflammatory process. However, postoperative
histopathology and immunohistochemical studies finally diagnosed
IMT. The tumor presented with intussusception, causing intestinal
obstruction. Intussusception in adults typically denotes
intraluminal pathology, as was the case in the patient discussed in
the present study.
The clinical presentation of intra-abdominal IMTs
depends on their location and growth pattern. Typically, the most
frequent early symptoms presented in patients are a palpable mass,
weight loss and/or fever, and abdominal pain. Laboratory
abnormalities are exhibited in a small number of patients (15,16). The
current case presented clinically with long-lasting abdominal pain
that had recently worsened to cramping. The results of the imaging
analysis of the tumor were not specific.
It is mainly agreed that surgery is the predominant
treatment modality for IMTs. However, a few studies have reported
certain benefits in the treatment of invasive or incompletely
resected IMT using immunosuppressive therapy with corticosteroids
and non-steroidal inflammatory agents (10,15),
radiation therapy (16) and
chemotherapy (2,5,16). In the
aggressive forms of IMT, exhibiting a high local recurrence rate
and a potential for metastasis, it is recommended that close
follow-up consisting of physical examination, radiographic imaging
and the evaluation of serial erythrocyte sedimentation rates is
undertaken (15). It has also been
recommended that post-surgical adjuvant treatments are administered
for intraabdominal IMT, as it has the highest rate of local
recurrence (25%) (17). The present
patient underwent a clear margin surgical excision with no further
adjuvant therapy. The patient remains asymptomatic following 6
months of follow-up, without any evidence of recurrent disease.
In conclusion, IMTs are rare, true neoplasms
exhibiting biological behavior that ranges from borderline to
potentially malignant variants. Complete surgical excision and a
long-term follow-up is the recommended therapeutic approach for
this disease.
References
|
1
|
Kim HW, Choi YH, Kang SM, Ku JY, Ahn JH,
Kim JM, Chung JM, Ha HK and Chung MK: Malignant inflammatory
myofibroblastic tumor of the bladder with rapid progression. Korean
J Urol. 53:657–661. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ernst CW, Van Der Werff Ten Bosch J,
Desprechins B, de Mey J and De Maeseneer M: Malignant
transformation of an abdominal inflammatory myofibroblastic tumor
with distant metastases in a child. JBR-BTR. 94:78–80.
2011.PubMed/NCBI
|
|
3
|
Gleason BC and Hornick JL: Inflammatory
myofibroblastic tumours: Where are we now? J Clin Pathol.
61:428–437. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Singer S, Neilsen T and Antonescu CR: Soft
tissue sarcoma. Cancer: Principles and Practice of Oncology. DeVita
VT Jr, Lawrence TS and Rosenberg SA: (9th). (Philadelphia, PA).
Lippincott Williams & Wilkins. 15402012.
|
|
5
|
Dishop MK, Warner BW, Dehner LP, Kriss VM,
Greenwood MF, Geil JD and Moscow JA: Successful treatment of
inflammatory myofibroblastic tumor with malignant transformation by
surgical resection and chemotherapy. J Pediatr Hematol Oncol.
25:153–158. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Brunn H: Two interesting benign lung
tumors of contradictory histopathology. J Thorac Surg. 9:119–131.
1939.
|
|
7
|
Navale P, Menon S, Bakshi G, Pruthy R and
Desai S: Inflammatory myofibroblastic tumor of kidney with
heterotopic bone formation: An unusual case mimicking a renal
malignancy. Indian J Med Paediatr Oncol. 34:320–322. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamrubboon W, Phongkitkarun S, Jaovisidha
S, Sirikulchayanonta V, Tapaneeyakorn J and Siripornpitak S:
Inflammatory myofibroblastic tumor of abdomen: Computerized
tomographic (CT) and pathological findings. J Med Assoc Thai.
91:1487–1493. 2008.PubMed/NCBI
|
|
9
|
Salim Rezaii M, Vahedi H, Salimi Z,
Froutan H and Sotoudeh P: Inflammatory myofibroblastic tumor of the
small bowel: A case report. Middle East J Dig Dis. 3:134–137.
2011.PubMed/NCBI
|
|
10
|
Baspınar S, Kapucuoglu N, Caloglu E,
Ozorak A, Guzel A and Degirmenci B: Invasive inflammatory
myofibroblastic tumor of the kidney with anaplastic lymphoma kinase
(ALK) expression. A case report. J Clin Anal Med. 4(Suppl 1):
77–80. 2013.
|
|
11
|
Coffin CM, Hornick JL and Fletcher CD:
Inflammatory myofibroblastic tumor: Comparison of
clinicopathologic, histologic, and immunohistochemical features
including ALK expression in atypical and aggressive cases. Am J
Surg Pathol. 31:509–520. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathologic and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Coffin CM and Fletcher JA: Inflammatory
myofibroblastic tumor. WHO classification of tumours of soft tissue
and bone. Fletcher CDM, Bridge JA, Hogendoorn PWC and Mertens F:
(Lyon, France). IARC Press. 83–84. 2013.
|
|
14
|
Bjelovic M, Micev M, Spica B, Babic T,
Gunjic D, Djuric A and Pesko P: Primary inflammatory
myofibroblastic tumor of the stomach in an adult woman: A case
report and review of the literature. World J Surg Oncol. 11:352013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bawahab MA: Inflammatory myofibroblastic
tumor of the small intestine presenting as septic shock in a young
woman. Pak J Surg. 29:143–146. 2013.
|
|
16
|
Ntloko S, Gounden A, Naidoo Madiba TE,
Singh Y, Ramdial PK and Hadley GP: Intestinal inflammatory
myofibroblastic tumour. S Afr J Surg. 49:190–193. 2011.PubMed/NCBI
|
|
17
|
Lorenzi L, Cigognetti M, Medicina D,
Pellegrini V, Balzarini P, Cestari R and Facchetti F: ALK-positive
inflammatory myofibroblastic tumor of the abdomen with widespread
microscopic multifocality. Int J Surg Pathol. 22:640–644. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ida S, Matsuzaki H, Kawashima S, Watanabe
M, Akiyama Y and Baba H: Adult intestinal intussusception caused by
an inflammatory myofibroblastic tumor. Case Rep Gastroenterol.
7:224–228. 2013. View Article : Google Scholar : PubMed/NCBI
|