Introduction
Despite a significant decline in its incidence and
mortality in the past century (1),
gastric cancer remains the fourth most common type of cancer, and
the second leading cause of cancer-associated mortalities worldwide
(2). In China, the majority of
gastric cancer cases are diagnosed as metastatic or recurrent
gastric cancer, which generally involves the liver, lung, bone and
abdominal cavity, and in 2008 the five-year survival rate was
<5% (3). The incidence of primary
carcinoma in the temporal bone has been previously reported to be
1/2,000 (4,5), while metastatic tumors in this organ are
less common than primary tumors (2).
In the present study, a rare case of hearing loss as a consequence
of metastasis of gastric cancer to temporal bone without the
involvement of other organs is reported.
Case report
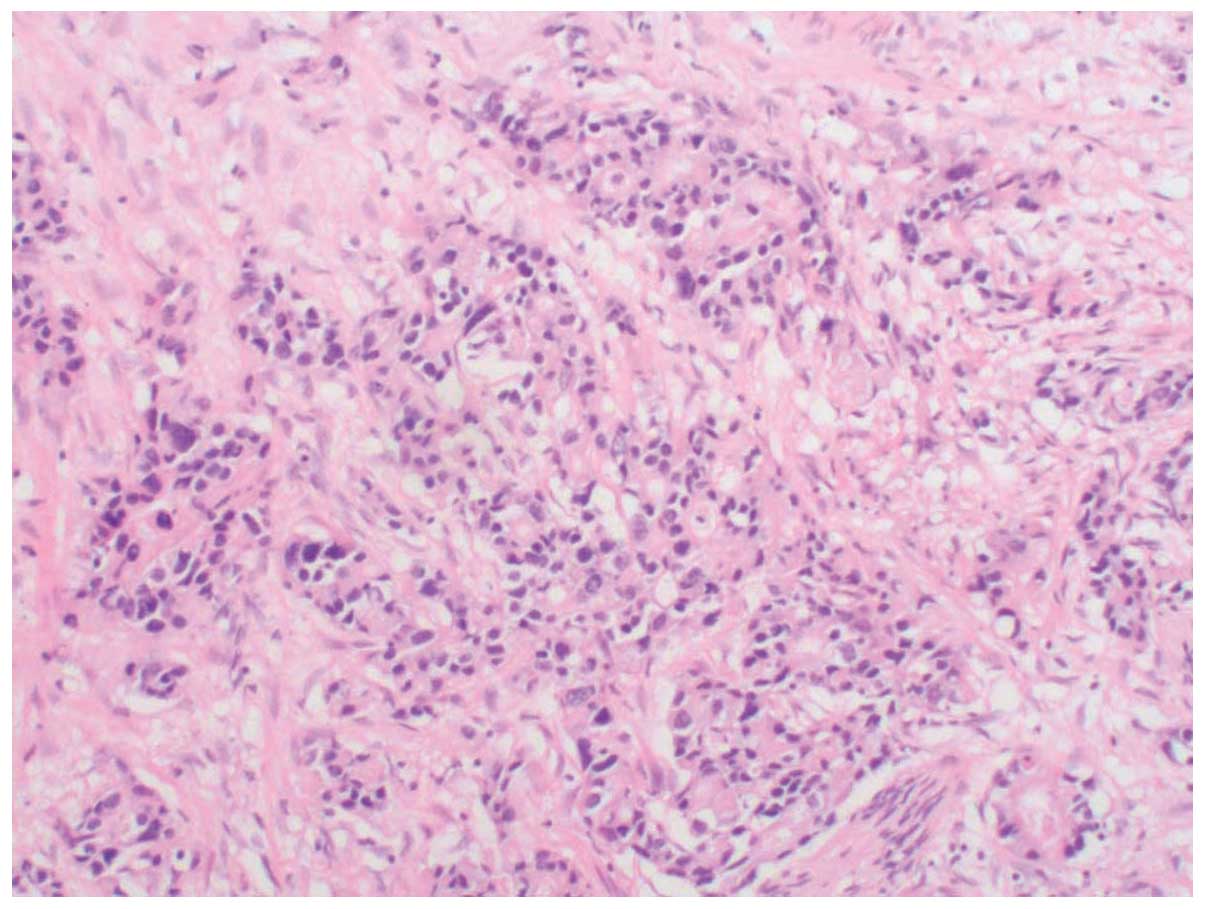
In April 2014, a 55-year-old male was diagnosed with
gastric cancer at The Affiliated Jiangyin Hospital of Southeast
University Medical College (Jiangyin, China). The patient underwent
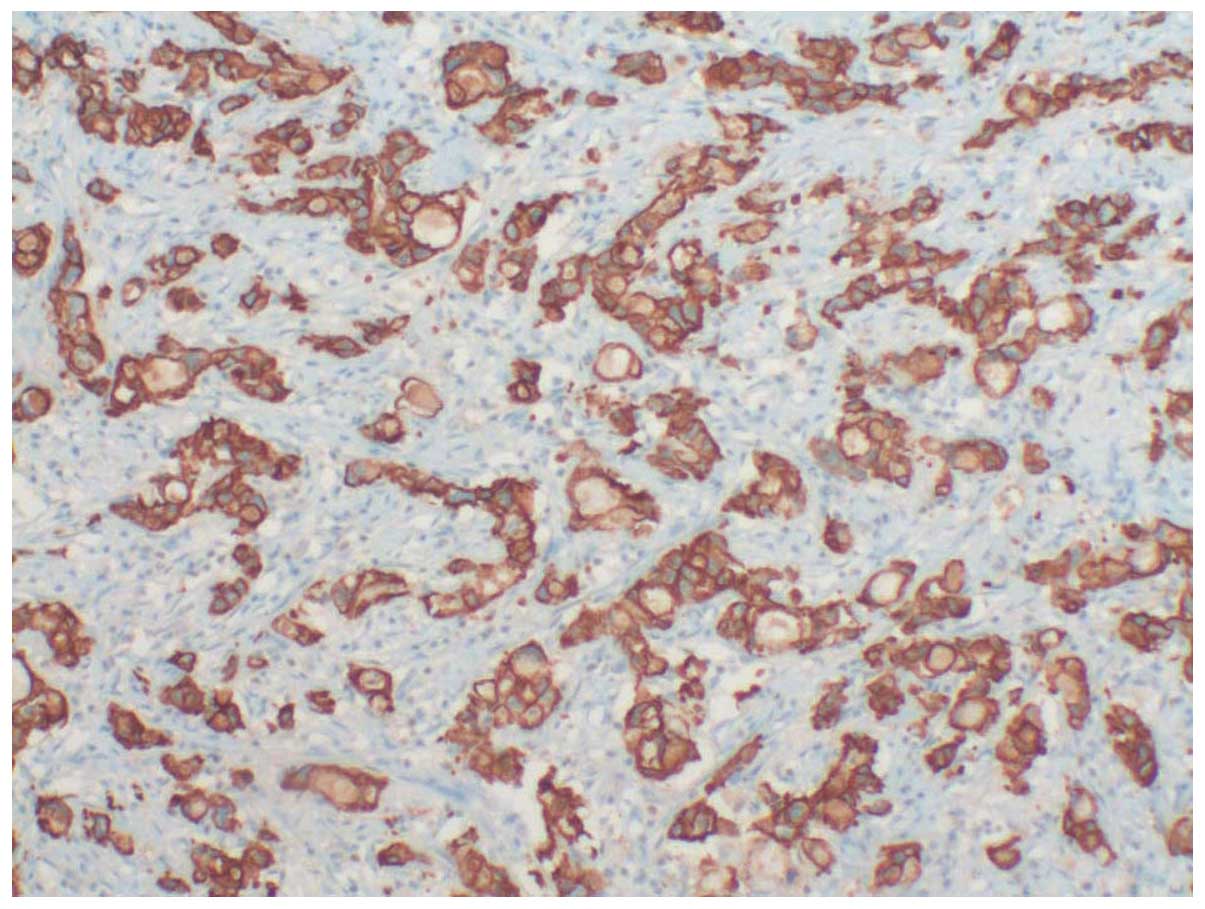
radical total gastrectomy, and the histopathological diagnosis was
gastric adenocarcinoma (Figs. 1 and
2). Immunohistochemistry demonstrated
positive staining for cytokeratin (CK)7, CK8/18, CK20 and
CKAE1/AE3, and negative staining for human epidermal growth factor
receptor (Her)-2, P53 and vimentin. The patient was next subjected
to postoperative chemotherapy, which consisted of six cycles of
combination chemotherapy with oxaliplatin (135 mg/m2 on
day 1 by intravenous (iv) infusion), epirubicin (EPI)-adriamycin
(ADM) (50 mg/m2 on day 1) and 5-fluorouracil (FU)
(375–425 mg/m2 on days 1–5 via iv infusion). Concomitant
palliative radiotherapy was administered to the gastric tumor bed
and local lymphatic drainage area, with a total dose of 45 Gy/25 F.
Bone scan (Symbia T16, Siemens AG, Munich, Germany) and abdominal
computed tomography (CT) (Brilliance-64, Philips Healthcare, DA
Best, The Netherlands) were performed as part of the regular
follow-up. The patient experienced hearing loss 11 months later,
and was admitted to the Department of Otolaryngology of The
Affiliated Jiangyin Hospital of Southeast University Medical
College for a full evaluation of the ear. Physical examination
indicated normal external auditory canal and tympanic membrane.
Bone conduction pure tone audiometry revealed mild (35 dB) loss of
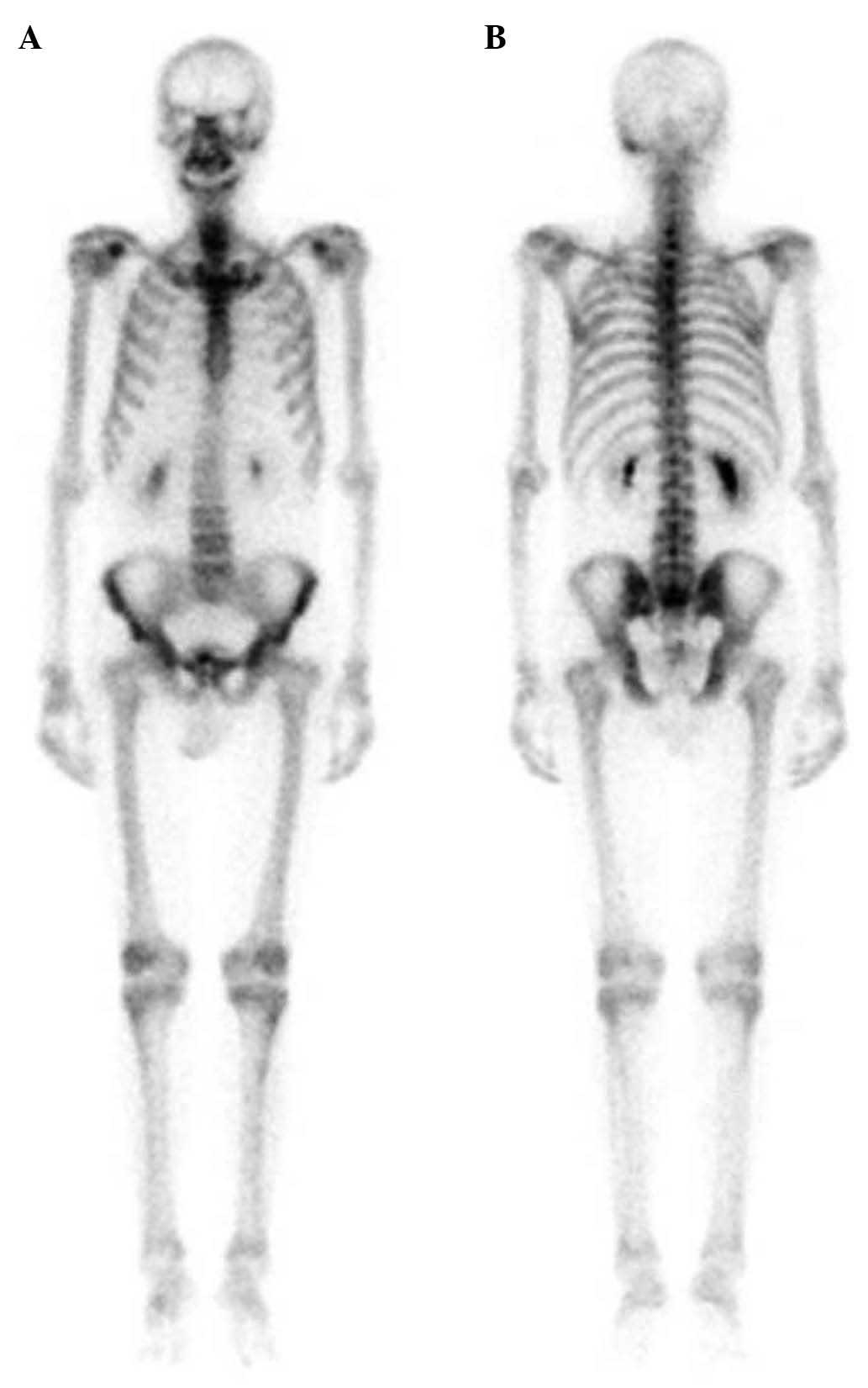
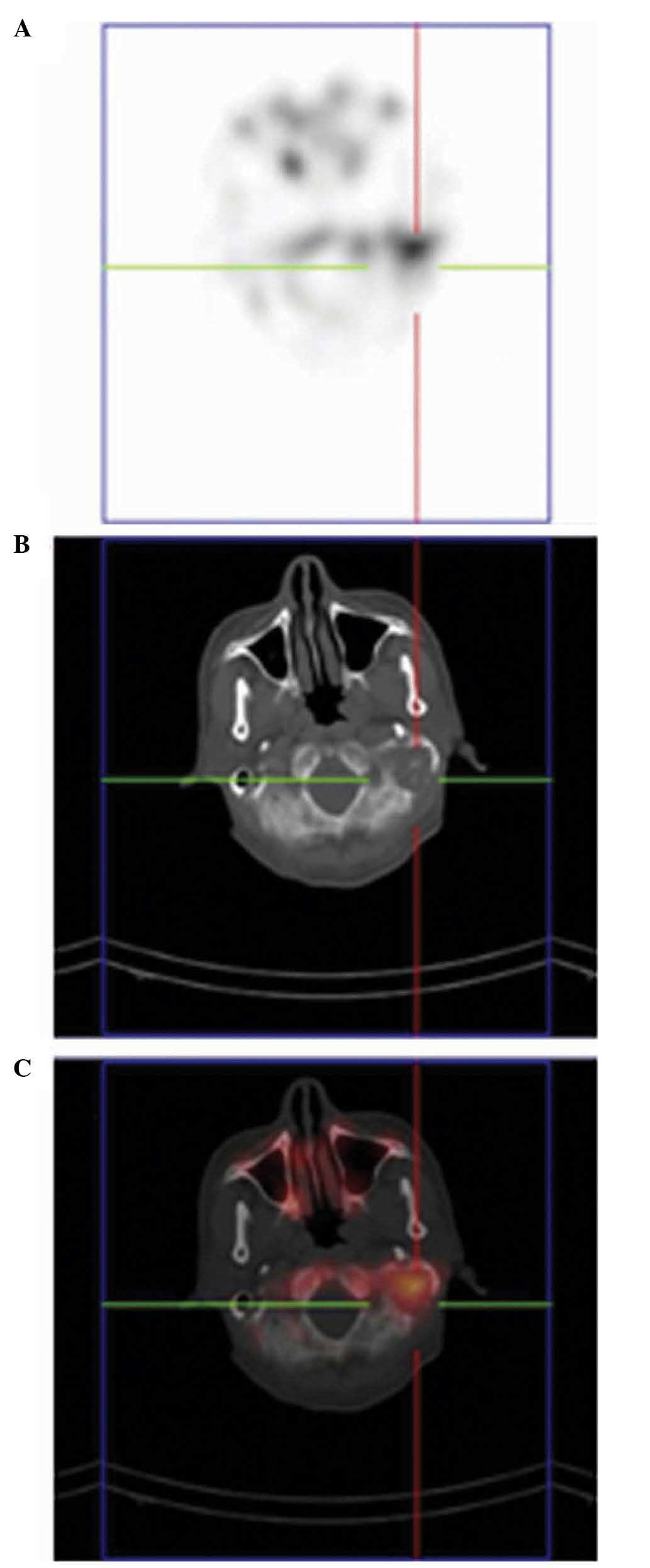
sensor neural hearing on the left side. Bone scan demonstrated
uptake in the left temporal bone (Figs.
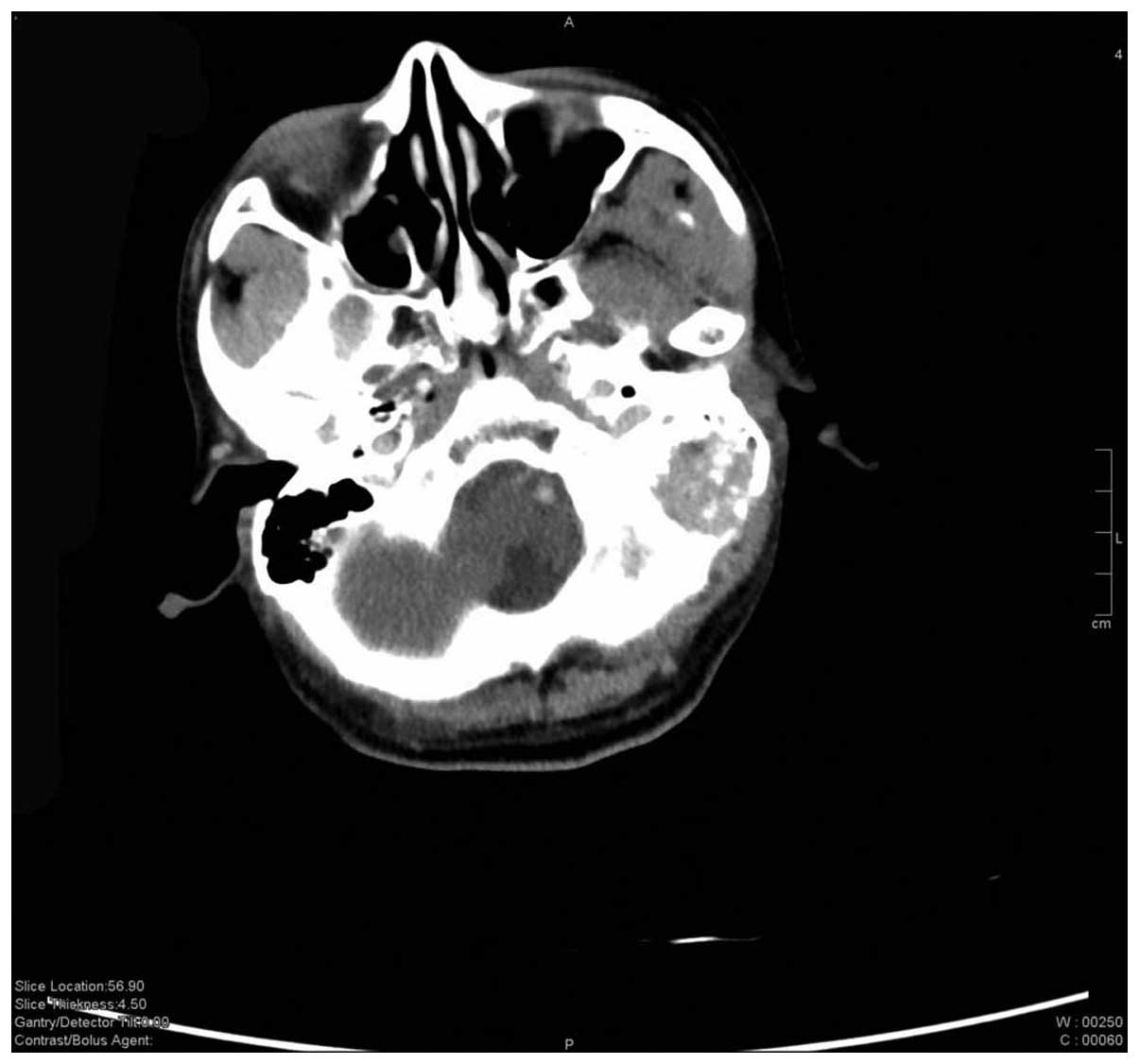
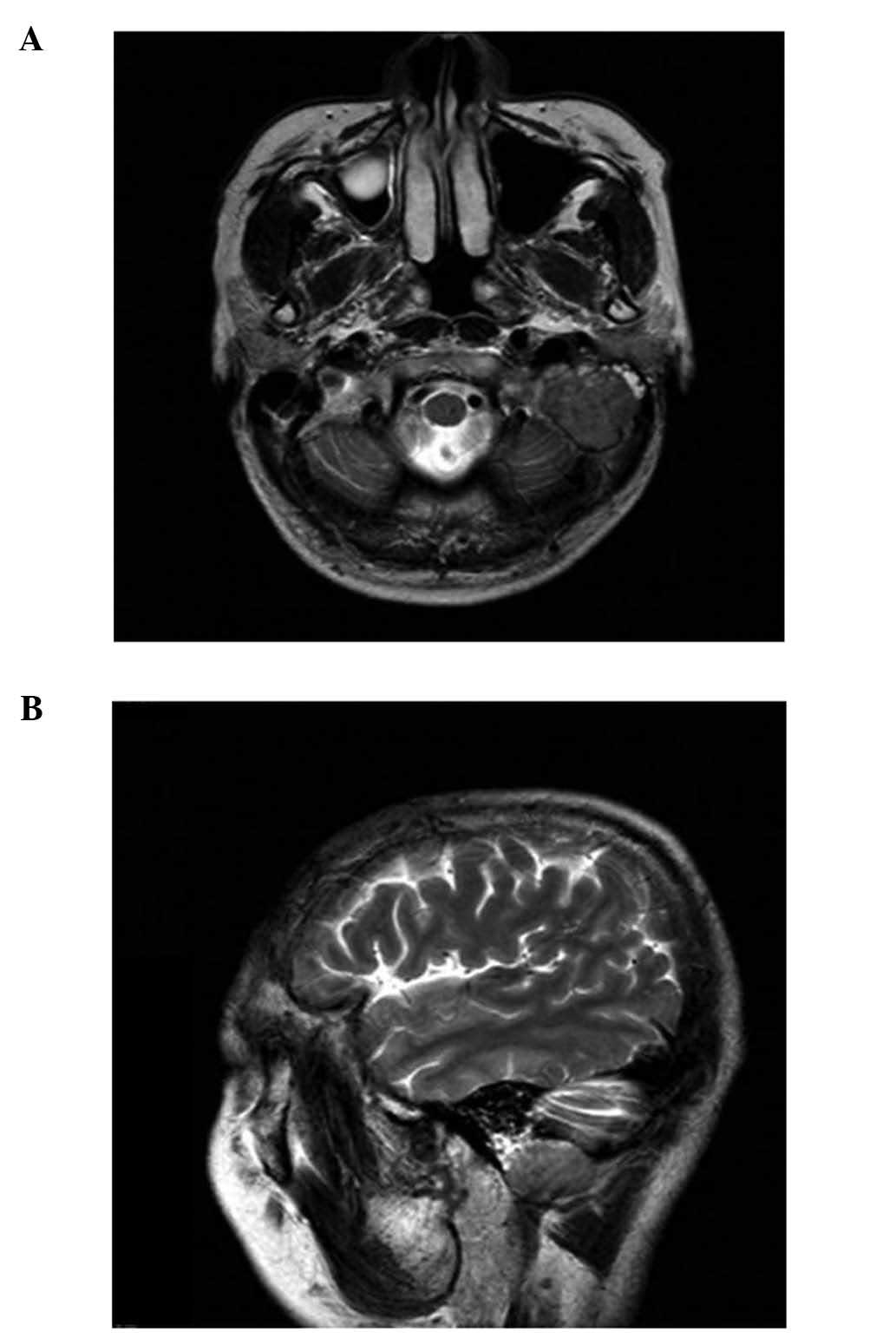
3 and 4). CT and magnetic
resonance imaging (MRI) (Achieva 3.0T, Philips Healthcare) of the
brain identified an enhancing lesion in the left petrous apex
(Figs. 5 and 6, respectively). Previous patients who were
clinically diagnosed with metastasis to the temporal bone received
radiotherapy with a total dose of 60 Gy for the treatment of the
tumor mass (6). Therefore, this
treatment was also applied to the patient of the present case
report, who is currently under treatment and has been under
observation for one year.
Discussion
Gastric cancer is one of the most common types of
cancer worldwide (2). A significant
number of patients with gastric cancer experience recurrence
following radical gastrectomy (7).
According to Baiocchi et al (8), the most frequent sites of recurrence
were the local/regional lymph nodes (35.4%), liver (24.3%),
peritoneum (30.3%), lung (10.4%) and intralumen (7.5%). A small
number of cases of metastasis to unusual sites such as skin, mouth
and leptomeninges have been previously reported (9–11).
Previous reports of hearing loss due to metastasis of gastric
cancer are infrequent (2,6). Ohno et al (12) and Kim et al (13) reported cases of metastasis of gastric
cancer to meningeal carcinoma, which resulted in hearing loss. Joo
et al (14) reported a case of
gastric cancer manifesting as a solitary metastasis in the
cerebellopontine angle that mimicked acoustic neuroma and caused
hearing loss. In addition, a case of metastasis of gastric cancer
to the internal auditory canal with multiple metastases to bone and
liver has been previously reported (15). To the best of our knowledge, there are
no reported cases of metastasis of Her-2− gastric cancer
to temporal bone without the involvement of other organs that only
present with the symptom of hearing loss.
Temporal bone cancer accounts for <0.2% of all
tumors involving the head and neck region (6). The majority of metastatic temporal bone
tumors tend to be asymptomatic, and it may cause a variety of
symptoms (6). Lionello et al
(16) reported the most common
clinical findings of temporal bone cancer, including aural
discharge (24–100%), bleeding (19–81%), hearing loss (2–75%) and
facial nerve paresis (7–64%).
The most common primary malignancy affecting the
temporal bone is breast cancer. Other sites of primary tumors
include the thyroid gland, brain, lungs, prostate and blood
(17). The most common site of
involvement in the temporal bone is the petrous apex, followed by
the tegmen tympani, mastoid bone and internal auditory canal
(17). Han et al (15) hypothesized that the circulation in the
marrow spaces of the petrous apex facilitates the deposition of
tumor cells, which is unusual in pneumatized areas inflated by the
tumor.
There are five possible patterns of tumor spreading
from the primary site to the temporal bone (5,6,15,17): i)
Hematogenous spreading; ii) directly spreading though the
surrounding tissues; iii) spreading through the cerebrospinal fluid
from an intracranial tumor; iv) leptomeningeal extension; and v)
leukemic infiltration. Hematogenous spreading appears to be the
most common route of tumor spreading, since it was responsible for
11 of the 12 cases reported in a previous study by Belal Jr
(17). In the present case, the
symptom of hearing loss may have been caused by direct invasion of
the estrous apex through hematogenous spreading from the gastric
cancer.
All patients with suspected temporal bone cancer
should be subjected to a full neurologic evaluation, including
hearing test, electronystagmography and cerebrospinal fluid
examination, which may aid in the diagnosis of meningeal carcinoma
(16). Radiological imaging,
including high-resolution CT and contrast-enhanced MRI are of
importance, since the anatomy of the temporal bone hinders physical
examination (13). Contrast-enhanced
MRI is capable of revealing the extent of the tumor and
differentiating the tumor from non-neoplastic soft tissue, while CT
scanning enables a reliable assessment of any invasion of the wall
of the internal carotid artery canal, jugular bulb and otic capsule
(13). The patient of the present
case report underwent CT, MRI and bone scan, and was diagnosed with
metastasis of gastric cancer to the temporal bone.
The prognosis of temporal bone carcinoma is
associated with the stage of the tumor and the effectiveness of the
primary treatment (16). The
recommend treatment for temporal bone cancer varies widely, and
surgery, radiotherapy and chemotherapy should be all considered,
depending on the performance status of the patient (6). There is previous evidence of systemic
chemotherapy being effective in metastatic disease (6,16,18). Previous studies have reported that
chemotherapy combined with 5-FU and cisplatin did not increase the
survival rate of patients with temporal bone cancer, but resulted
in an improved control of the pain in these patients (5,6,13). Furthermore, previous studies have
reported a positive effect of radiotherapy for advanced (T2-T4,
according to the Pittsburgh staging system) temporal bone
malignancies (6,13).
In conclusion, metastatic tumor of the temporal bone
with a history of Her-2− gastric cancer is rare.
Radiological imaging, including MRI, CT, bone scan and positron
emission tomography-CT may aid to delineate the extent of
metastases.
References
|
1
|
Redon R, Ishikawa S, Fitch KR, Feuk L,
Perry GH, Andrews TD, Fiegler H, Shapero MH, Carson AR, Chen W, et
al: Global variation in copy number in the human genome. Nature.
444:444–454. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carcas LP: Gastric cancer review. J
Carcinog. 13:142014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lim ST, Hee SW, Quek R, Lim LC, Yap SP,
Loong EL, Sng I, Tan LH, Ang MK, Ngeow J, et al: Comparative
analysis of extra-nodal NK/T-cell lymphoma and peripheral T-cell
lymphoma: Significant differences in clinical characteristics and
prognosis. Eur J Haematol. 80:55–60. 2008.PubMed/NCBI
|
|
4
|
Lee HJ, Yang HK and Ahn YO: Gastric cancer
in Korea. Gastric Cancer. 5:177–182. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Streitmann MJ and Sismanis A: Metastatic
carcinoma of the temporal bone. Am J Otol. 17:780–783.
1996.PubMed/NCBI
|
|
6
|
Choi SH, Park IS, Kim YB and Hong SM:
Unusual presentation of a metastatic tumor to the temporal bone:
Severe otalgia and facial paralysis. Korean J Audiol. 18:34–37.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fukuchi M, Ishiguro T, Ogata K, Kimura A,
Kumagai Y, Ishibashi K, Ishida H, Kuwano H and Mochiki E: Risk
factors for recurrence after curative conversion surgery for
unresectable gastric cancer. Anticancer Res. 35:6183–6187.
2015.PubMed/NCBI
|
|
8
|
Baiocchi GL, Marrelli D, Verlato G,
Morgagni P, Giacopuzzi S, Coniglio A, Marchet A, Rosa F, Capponi
MG, Di Leo A, et al: Follow-up after gastrectomy for cancer: An
appraisal of the Italian research group for gastric cancer. Ann
Surg Oncol. 21:2005–2011. 2014.PubMed/NCBI
|
|
9
|
Satoh H, Okhi T, Momma T, Saito S, Niizeki
H, Hirose S and Kuramochi S: Penile skin metastasis of gastric
carcinoma associated with prostate carcinoma: A case report. Nihon
Hinyokika Gakkai Zasshi. 92:628–631. 2001.(In Japanese). PubMed/NCBI
|
|
10
|
Nakabayashi H, Murata K, Sakaguchi M,
Nakajima K and Katsuyama J: Choroid plexus metastasis from gastric
cancer - case report. Neurol Med Chir (Tokyo). 34:183–186. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shimoyama S, Seto Y, Aoki F, Ogawa T, Toma
T, Endo H, Itouji T and Kaminishi M: Gastric cancer with metastasis
to the gingiva. J Gastroenterol Hepatol. 19:831–835. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ohno T, Yokoyama Y, Aihara R, Mochiki E,
Asao T and Kuwano H: Sudden bilateral sensorineural hearing loss as
the presenting symptom of meningeal carcinomatosis of gastric
cancer: Report of a case. Surg Today. 40:561–565. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim CH, Shin JE, Roh HG, Lee JS and Yoon
SY: Sudden hearing loss due to internal auditory canal metastasis
of Her2-positive gastric cancer: A case report. Oncol Lett.
8:394–396. 2014.PubMed/NCBI
|
|
14
|
Joo HY, Chae MH, Lim JH, Yi HG, Lee MH,
Kim CS and Park YH: A case of gastric cancer manifesting as a
solitary brain metastasis in the cerebellopontine angle that
mimicked acoustic neuroma. Chonnam Med J. 49:133–135. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Han JK, Park KH, Lee MS and Lee CK:
Gastric carcinoma metastasis to the internal auditory canal. Otol
Neurotol. 33:e19–e20. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lionello M, Stritoni P, Facciolo MC,
Staffieri A, Martini A, Mazzoni A, Zanoletti E and Marioni G:
Temporal bone carcinoma. Current diagnostic, therapeutic, and
prognostic concepts. J Surg Oncol. 110:383–392. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Belal A Jr: Metastatic tumours of the
temporal bone. A histopathological report. J Laryngol Otol.
99:839–846. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kunst H, Lavieille JP and Marres H:
Squamous cell carcinoma of the temporal bone: Results and
management. Otol Neurotol. 29:549–552. 2008. View Article : Google Scholar : PubMed/NCBI
|