Introduction
Spontaneous subarachnoid hemorrhage (SAH) is the
most common cerebral vascular disease, and 75% of SAHs are caused
by rupture of an intracranial aneurysm (1–4). In
patients with poor-grade aneurysm, 20–45% of SAHs are associated
with high morbidity and mortality, although a few studies have
reported fatality rates of ≤60–90% (1,2,5–8). The
conventional approach to treat this condition suggests that surgery
should be performed when the patients have recovered from the SAH
or when their Hunt and Hess grade has reduced to level ≤III, since
early surgery following SAH is considered to present a high risk,
as is associated with brain swelling, bleeding and unstable vital
signs (4). However, recent studies
have observed that early rebleeding occurs mostly within 24 h of
SAH, particularly in the first 6–12 h, when the risk of ultra-early
rebleeding is highest (9–12). Intracerebral hematoma, rebleeding and
severe cerebral vasospasm may lead to serious neurologic deficit in
the early time subsequent to SAH (8,9).
Therefore, the optimal time to operate and the strategy to select
for poor-grade aneurysms remain controversial (9,11). The aim
of the present study is to review the surgical management of
poor-grade aneurysms by ultra-early microsurgery, and to
investigate the prognosis of this strategy.
Materials and methods
Patient population
From April 2010 to June 2013, 18 cases of Hunt and
Hess grade IV or V aneurysms accompanied with hematoma were treated
by microsurgical clipping at the Department of Neurosurgery of The
101st Hospital of Chinese People's Liberation Army (Wuxi, China).
The patients' characteristics are presented in Table I. Of 18 patients, 12 (66.7%) exhibited
Hunt and Hess grade IV and 6 (33.3%) presented grade V (13). In total, 10 patients were men and 8
were women, and their mean age was 56.9±15.8 years (range, 31–75
years). Prior to the operation, 8 (44.4%) cases presented a
cerebral hernia, the clinical features of which included sudden
fall into a coma, acute vomiting and coma following headache for 1
h-3 days with Glasgow Coma Scale of 3–9. All surviving patients
were followed-up for 6–36 months.
 | Table I.Patients' characteristics. |
Table I.
Patients' characteristics.
| Variable | N (%) |
|---|
| Total | 18 (100.0) |
| Gender |
|
| Male | 10 (55.6) |
|
Female | 8 (44.4) |
| Age, years |
|
| ≥60 | 8 (44.4) |
|
<60 | 10 (55.6) |
| Hunt and Hess
grade |
|
| IV | 12 (66.7) |
| V | 6 (33.3) |
| Hypertension |
|
| Yes | 8 (44.4) |
| No | 10 (55.6) |
| Cerebral hernia prior
to operation |
|
| Yes | 8 (44.4) |
| No | 10 (55.6) |
| Operation time
following SAH |
|
| <24
h | 15 (83.3) |
| >24
h | 3 (16.7) |
Radiological features
All 18 patients underwent head computed tomography
(CT; Lightspeed VCT; GE Healthcare Bio-Sciences, Pittsburgh, PA,
USA) and CT angiography (CTA; Lightspeed VCT; GE Healthcare
Bio-Sciences) prior to surgery. Bleeding was distributed in the
anterior cerebral artery in 2 cases, in the middle cerebral artery
in 6 cases, in the anterior communicating artery in 7 cases and in
the posterior circulation in 3 cases. The location and diameter of
the aneurysm, and the volume of intracerebral hematoma are
presented in Table II.
| Table II.Radiological features of 18 cases of
poor-grade aneurysm. |
Table II.
Radiological features of 18 cases of
poor-grade aneurysm.
| Variable | Cases, n |
|---|
| Location of
aneurysm |
|
| Anterior
circulation | 2 |
| Anterior
communicating artery | 7 |
| Middle
cerebral artery | 6 |
| Posterior
circulation | 3 |
| Diameter of aneurysm,
mm |
|
|
<5 | 7 |
|
5–10 | 9 |
|
>10 | 2 |
| Volume of hematoma,
ml |
|
|
<30 | 9 |
|
30–50 | 5 |
|
>50 | 4 |
Procedure prior to surgery
In the emergency room, all patients received trachea
intubation to preserve normal oxygen concentration, and ventilation
to assist breathing. Intravenous access was established for all
patients to ensure sufficient blood supply, while central venous
catheter insertions were established in certain shocked patients.
After the vital signs were stable, patients received radiographic
examinations, including head CT and CTA. Prior to operation, all
patients received hemostatic and anti-vasospasm agents such as a
nimodipine injection (Bayer AG, Leverkusen, Germany). All patients
with cerebral hernia or posttraumatic acute diffuse brain swelling
also received 125 ml 20% mannitol (CR Double-Crane Pharmaceutical
Co., Ltd., Beijing, China) via bolus intravenous injection to
reduce intracranial pressure (ICP). The duration and frequency of
the drugs were adjusted according to the seriousness of the
disease.
Surgical procedure
In the operation room, all patients received urgent
trachea intubation and general anesthesia. A total of 15 patients
underwent microsurgery within 24 h of SAH, and 3 patients underwent
emergency microsurgery 24 h later, since these patients were
hospitalized 24 h after SAH. In total, 13 patients were operated by
standard large trauma craniotomy with transsylvian fissure
approach, while 2 patients with anterior cerebral artery and
anterior interhemispheric hematoma were subjected to
interhemispheric approach, and 3 patients with posterior
circulation aneurysm were operated by posterior fossa craniotomy. A
total of 7 patients received lateral ventricular drainage for 1
week. All 18 patients adopted bone flap decompression to reduce ICP
and risk of cerebral infarction following surgery.
Post-surgical procedure
All patients received nimodipine following surgery
to reduce cerebral vasospasm and improve blood circulation in the
brain. Lumbar puncture was used to release hemorrhagic
cerebrospinal fluid (CSF) as early as possible in patients who had
not received post-surgery lateral ventricular drainage. All
patients in coma were subjected to tracheotomy. Hyperbaric
oxygenation and acupuncture were also used in certain patients as a
later treatment if their clinical signs were stable. Hydrocephalus
cases underwent ventriculoperitoneal shunting.
Statistical analysis and outcome
assessment
Data analysis was performed using SPSS version 14.0
software (SPSS, Inc., Chicago, IL, USA). P<0.05 was considered
to indicate a statistically significant difference. Continuous
variables were expressed as range and mean ± standard deviation.
Independent samples tests were used for continuous variables. For
categorical variables, χ2 test, rank-sum test or
Fisher's exact test were used. The surgical curative effects were
evaluated post-surgery based on the Glasgow Outcome Scale (GOS)
(14): Favorable (grade 4-5),
dissatisfied (grade 2-3) and deceased (grade 1). All patients were
followed-up for 6–36 months.
The present study was approved by the Ethics
Committee of Anhui Medical University (Wuxi, China), and signed
informed consent was obtained from all patients.
Results
Clinical outcome
Follow-up CTA or angiography reexamination
demonstrated that all aneurysms were completely occluded and none
relapsed. All 18 patients received GOS assessment by follow-up for
6–36 months post-surgery. Of these, 4 (22.2%) cases presented
favorable outcomes, 10 (55.5%) cases presented dissatisfied
outcomes (including 4 cases who were severely disabled and 6 cases
who were in a vegetative state), and 4 (22.2%) cases succumbed to
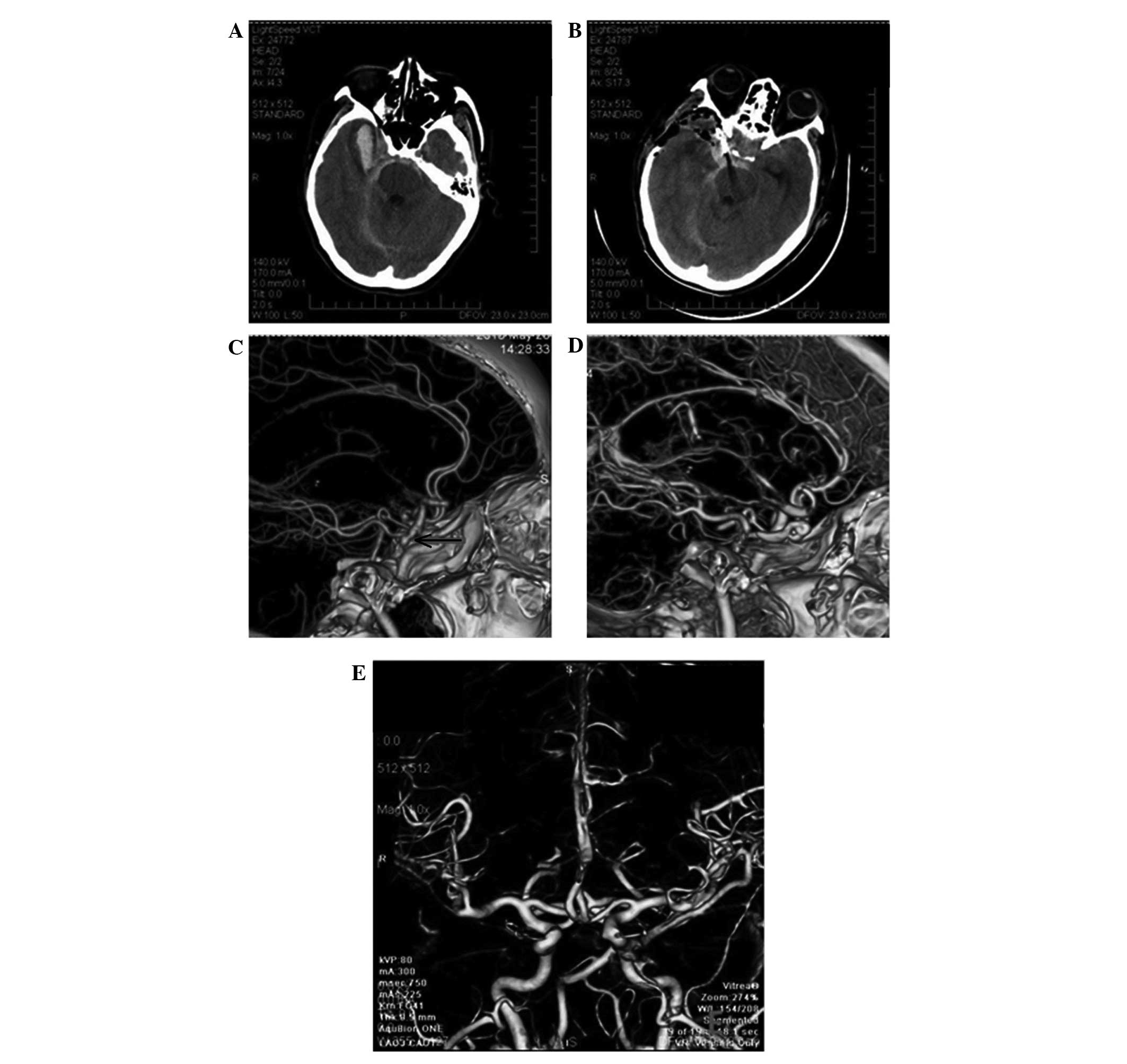
the disease. Representative cases appear in Fig. 1. CT imaging prior to surgery
demonstrated extensive SAH, particularly in the basal cistern. In
addition, intracerebral hematoma was observed in the right temporal
frontal lobes (Fig. 1A). Following
surgery, the aneurysm was occluded and the hematoma was
sufficiently removed (Fig. 1B). The
right posterior communicating aneurysms are indicated by a red
arrow in Fig. 1C. The immediate
post-surgery CTA demonstrated perfect occlusion of the aneurysm
(Fig. 1D). The follow-up CTA at 6
months post-surgery revealed no obvious intracranial vascular
stenosis and good vascular morphology (Fig. 1E).
Operation schedule
Patients who underwent surgery within 24 h of SAH
(of 15 cases, 7 cases were operated within 6 h of SAH, while 8
cases were operated within 6–24 h) exhibited more favorable
outcomes (favorable outcomes were observed in 4 patients), compared
with 3 cases who were subjected to surgery after 24 h of SAH (of
which, 2 patients were in vegetative state and 1 was deceased).
Vasospasm and cerebral infarction
Local vasospasm was identified by CTA and
transcranial Doppler sonography (Pro Focus 2202; BK Medical,
Herlev, Denmark) in 5 (27.8%) of 18 patients. These 5 patients
received decompressive craniectomy, lumbar puncture and nimodipine
therapy without technical complications. However, all of them had
poor prognosis, including 3 patients who were dissatisfied (GOS
grade 3) and 2 patients who succumbed to disease. Cerebral
infarction in different parts of the brain was detected in 7
patients, including 4 cases with cerebral infarction in the basal
ganglia region and 3 cases in the brain parenchyma.
Hunt and Hess grade and outcome
In the present study, 4 patients had favorable
prognosis among the 12 cases whose Hunt and Hess grade was IV,
while 6 patients whose Hunt and Hess grade was V had poor
prognoses.
Individual factors and outcome
The prognosis factors of poor-grade aneurysm
combined with intracerebral hematoma were the diameter of the
aneurysm, volume of the hematoma and cerebral hernia and absence of
operation. The association between these factors is indicated in
Table III. The present study
demonstrated that all patients with an aneurysm diameter >10 mm,
intracerebral hematoma volume >50 ml and presence of cerebral
hernia prior to operation had bad prognosis.
| Table III.Individual factors and outcome for 18
cases of poor-grade aneurysm. |
Table III.
Individual factors and outcome for 18
cases of poor-grade aneurysm.
|
| Cases, n |
|---|
|
|
|
|---|
| Variable | Fav | Dis | Dec | P-value |
|---|
| Diameter of
aneurysm, mm |
|
|
| 0.035 |
|
<5 | 1 | 4 | 2 |
|
|
5–10 | 3 | 6 | 0 |
|
|
>10 | 0 | 0 | 2 |
|
| Volume of hematoma,
ml |
|
|
| 0.046 |
|
<30 | 3 | 5 | 1 |
|
|
30–50 | 1 | 4 | 0 |
|
|
>50 | 0 | 1 | 3 |
|
| Cerebral
hernia |
|
|
| 0.038 |
|
Yes | 0 | 5 | 3 |
|
| No | 4 | 5 | 1 |
|
Extraventricular drainage and
outcome
In the present study, 7 patients underwent
extraventricular drainage following operation. Of them, 4 had
favorable outcomes, whereas the others had bad prognoses. In
addition, the 11 cases who did not accept extraventricular drainage
following operation had unfavorable outcomes (P=0.034 vs.
extraventricular drainage group; Table
IV).
| Table IV.Extraventricular drainage and outcome
of patients with poor-grade aneurysm. |
Table IV.
Extraventricular drainage and outcome
of patients with poor-grade aneurysm.
|
| Cases, n (%) |
|---|
|
|
|
|---|
| Variable | Favorable | Dissatisfied | Deceased | P-value |
|---|
| Extraventricular
drainage |
|
|
|
|
|
Yes | 4 (57.1%) | 2 (28.6%) | 1 (14.3%) | 0.034 |
| No | 0 (0.0%) | 8 (72.7%) | 3 (27.3%) | – |
Discussion
Conventionally, conservative treatment has been
initially employed for poor-grade aneurysms, followed by operation
when patients recovered or their Hunt and Hess grade reduced to
level ≤III (4). However, the majority
of patients would succumb to rebleeding and cerebral vasospasm
prior to surgery (1–3). Recent studies have suggested that
ultra-early microsurgery within 24 h of SAH may improve the
prognosis of patients with poor-grade aneurysm, since it may
prevent rebleeding and may delay the release of toxic substances
during cerebral vasospasm, thus reducing damage to the brain
(15–18).
It was previously considered that early surgery or
delayed surgery was meaningless to improve the prognosis of
patients with poor-grade aneurysm following SAH (4). To date, the selection of treatment time
in patients with Hunt and Hess grades IV and V remains
controversial (19,20). Certain authors disagree with the use
of ultra-early surgery due to the following reasons: i) Difficulty
of ultra-early diagnosis; ii) the bleeding of the ruptured aneurysm
may be not stopped, as time is limited; iii) the aneurysm may
rupture easily during the operation; iv) temporary occlusion of the
parent artery during microsurgery may lead to cerebral infarction;
and iv) surgery on the exposed aneurysm and parent artery is
difficult and has a high risk associated (4). By contrast, other authors agree with the
use of ultra-early surgery, due to the following benefits: i)
Ultra-early surgery may reduce the risk of rebleeding and the
occurrence of cerebral vasospasm; ii) ultra-early surgery may clip
the aneurysm and also remove the intracerebral hematoma, which may
lead to injury of the brain tissue; and iii) ultra-early
decompressive craniectomy may improve cerebral hernia by decreasing
ICP (9,15,16,18). In
the present study, 15 of 18 cases who underwent ultra-early surgery
had favorable outcomes, while 3 cases who underwent surgery after
24 h of SAH had poor prognosis. Therefore, ultra-early microsurgery
may improve the prognosis of patients with poor-grade aneurysm and
intracerebral hematoma.
The management of patients with poor-grade aneurysm
combined with intracerebral hematoma remains controversial
(21–23), due to the cerebral vasospasm and
intracerebral hematoma space-occupying effect as a consequence of
elevated ICP (21–23). Therefore, it is difficult to solve the
problem by simple microsurgical clipping and endovascular coiling.
Certain authors prefer to use endovascular coiling, since it is
considered to present several advantages, including less trauma and
shorter preoperative preparation or operative time when compared to
general surgery (17). However, this
procedure is generally ineffective or even aggravating for removing
the intracranial hematoma and resolving the vasospasm (24,25). Prat
and Galeano (26) reported 12 cases
of mild cerebral artery aneurysm with intracerebral hematoma who
demonstrated good outcomes following early surgery. Sasaki et
al (27) also observed that early
surgery clipped the aneurysm and removed the subarachnoid
hematocele and intracerebral hematoma. In addition, for the 26
patients who accepted conservative treatment, 20 succumbed to
disease and 6 suffered severe disabilities (28). These findings were significant
(P<0.01), compared with the ultra-early surgery group (28). Whether poor-grade aneurysms combined
with intracerebral hematoma are more suitable for ultra-early
surgery remains to be determined. Ultra-early surgery may achieve
four major goals: i) To remove the hematoma, thus relieving the
space-occupying effect and reducing the secondary injury of
perihematomal tissues; ii) intraoperative continuous irrigation of
papaverine or nimodipine may relieve cerebral vasospasm; iii)
decompressive craniectomy may reduce the ICP and release more space
to aid patients during the period of edema; and iv) it may reduce
the risks of delayed cerebral vasospasm (15–17). In
the present study, of the 18 patients that accepted early surgical
treatment, 4 (22.2%) cases had favorable outcomes, 11 (61.1%) cases
had dissatisfied outcomes, and 3 (16.7%) cases were deceased during
a follow-up of 1–2 years.
In total, 13 patients were operated by standard
large trauma craniotomy transsylvian fissure approach, 2 patients
with anterior cerebral artery were operated with interhemispheric
approach and 3 patients with posterior circulation aneurysms were
operated with posterior fossa craniotomy in the present study.
During surgery, it is important to fully remove the sphenoid ridge
upon removing the bone flap to facilitate the vision of the
operation (26). It is possible to
identify the majority of aneurysms from the sylvian fissure, while
a small number of anterior communicating artery aneurysms or distal
anterior cerebral artery aneurysms may be identified from
longitudinal observation (26). The
major difficulties of poor-grade aneurysm combined with
intracerebral hematoma are acute diffuse brain swelling, high ICP,
intraoperative rupture of the aneurysm and hematoma surrounding the
blood vessels, which results in a complicated local anatomic
structure (27). Mannitol may be used
as a dehydration therapy to partially remove the CSF and reduce the
ICP, but the hematoma should not be completely removed prior to the
occlusion of the aneurysm, since otherwise the aneurysm would
easily rupture during the operation. Prior to clipping the
aneurysm, the parent artery must be fully exposed to enable
adaptation to the temporary arterial occlusion (23). However, temporary arterial occlusion
must last <15 min, since otherwise it may lead to ischemia and
anoxia of the brain tissue. The hematoma should be extensively
removed once the aneurysm is occluded (18). Meanwhile, continuous irrigation of
papaverine or nimodipine intraoperative aids to relieve the
cerebral vasospasm (29).
Extraventricular drainage has been widely used for
treating poor-grade aneurysm, particularly when it is combined with
ventricle hematocele or obstruction of the fourth ventricle
(15). Occasionally, patients who
have received conservative treatments or delayed operation
treatments may adopt extraventricular drainage at the earliest
opportunity, in order to control acute ICP and improve the outcome
(30). In the present study, a high
risk of rebleeding was observed when patients underwent
extraventricular drainage prior to occlusion of the aneurysm. Of 7
patients with poor-grade aneurysms that received extraventricular
drainage, 4 patients succumbed to rebleeding within 48 h. These
findings are in agreement with those from previous studies on
extraventricular drainage prior to operation (15,16). In
the present study, the effect of extraventricular drainage
following the occlusion of the aneurysm was evaluated. Of the 18
patients enrolled in the study, 7 underwent this treatment, and
good recovery occurred in 4 (57.1%) patients, while severe
disabilities occurred in 2 (28.6%) patients and vegetative state
occurred in 1 (14.3%) patient. No rebleeding occurred subsequent to
the procedure. The prognosis of patients treated with
extraventricular drainage following the occlusion of the aneurysm
was improved, compared with those who did not undergo this
treatment (P<0.05).
The mortality and disability rates for patients with
poor-grade aneurysms remain high, particularly for those that are
accompanied by hematoma (18,23,26). The
diameter of the aneurysm, the volume of the hematoma and the
presence of cerebral hernia or absence of previous operation are
important prognosis factors for these patients (4). Early diagnosis, followed by ultra-early
surgery or emergency surgery to clip the aneurysm and remove the
intracerebral hematoma, contribute to a good prognosis.
Furthermore, the outcome improves if surgery is combined with
extraventricular drainage and decompressive craniectomy (4).
Although the current study is not a randomized
controlled trial, the present preliminary results suggest a
favorable outcome for patients with poor-grade aneurysm subjected
to ultra-early surgery following SAH, and constitute the basis for
future studies. In conclusion, ultra-early surgery or emergency
surgery may be beneficial for patients with severe SAH.
References
|
1
|
Rosengart AJ, Schultheiss KE, Tolentino J
and Macdonald RL: Prognostic factors for outcome in patients with
aneurysmal subarachnoid hemorrhage. Stroke. 38:2315–2321. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Komotar RJ, Schmidt JM, Starke RM,
Claassen J, Wartenberg KE, Lee K, Badjatia N, Connolly ES Jr and
Mayer SA: Resuscitation and critical care of poor-grade
subarachnoid hemorrhage. Neurosurgery. 64:397–411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Steiner T, Juvela S, Unterberg A, Jung C,
Forsting M and Rinkel G: European Stroke Organization: European
Stroke Organization guidelines for the management of intracranial
aneurysms and subarachnoid haemorrhage. Cerebrovasc Dis. 35:93–112.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yasargil MG and Feng L: Microneurosurgical
(1st). 3:Beijing Science and Technology Press. Beijing: 2005.
|
|
5
|
Longstreth WT Jr, Nelson LM, Koepsell TD
and van Belle G: Clinical course of spontaneous subarachnoid
hemorrhage: A population-based study in King County, Washington.
Neurology. 43:712–718. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nowak G, Schwachenwald R and Arnold H:
Early management in poor grade aneurysm patients. Acta Neurochir
(Wien). 126:33–37. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rordorf G, Ogilvy CS, Gress DR, Crowell RM
and Choi IS: Patients in poor neurological condition after
subarachnoid hemorrhage: Early management and long-term outcome.
Acta Neurochir (Wien). 139:1143–1151. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Le Roux PD, Elliott JP, Newell DW, Grady
MS and Winn HR: Predicting outcome in poor-grade patients with
subarachnoid hemorrhage: A retrospective review of 159 aggressively
managed cases. J Neurosurg. 85:39–49. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jartti P, Isokangas JM, Karttunen A,
Jartti A, Haapea M, Koskelainen T and Tervonen O: Early rebleeding
after coiling of ruptured intracranial aneurysms. Acta Radiol.
51:1043–1049. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hutchinson PJ, Power DM, Tripathi P and
Kirkpatrick PJ: Outcome from poor grade aneurysmal subarachnoid
haemorrhage - which poor grade subarachnoid haemorrhage patients
benefit from aneurysm clipping? Br J Neurosurg. 14:105–109. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
van den Berg R, Rinkel GJ and Vandertop
WP: Treatment of ruptured intracranial aneurysms: Implications of
the ISAT on clipping versus coiling. Eur J Radiol. 46:172–177.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Laidlaw JD and Siu KH: Ultra-early surgery
for aneurysmal subarachnoid hemorrhage: Outcomes for a consecutive
series of 391 patients not selected by grade or age. J Neurosurg.
97:250–258. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Botterell EH and Cannell DE: Subarachnoid
hemorrhage and pregnancy. Am J Obstet Gynecol. 72:844–855.
1956.PubMed/NCBI
|
|
14
|
Jennett B and Bond M: Assessment of
outcome after severe brain damage. Lancet. 1:480–484. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hosoda K, Fujita S, Kawaguchi T, Shose Y,
Hamano S and Iwakura M: Effect of clot removal and surgical
manipulation on regional cerebral blood flow and delayed vasospasm
in early aneurysm surgery for subarachnoid hemorrhage. Surg Neurol.
51:81–88. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fujii Y, Takeuchi S, Sasaki O, Minakawa T,
Koike T and Tanaka R: Ultra-early rebleeding in spontaneous
subarachnoid hemorrhage. J Neurosurg. 84:35–42. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Laidlaw JD and Siu KH: Poor-grade
aneurysmal subarachnoid hemorrhage: Outcome after treatment with
urgent surgery. Neurosurgery. 53:1275–1282. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wong GK, Boet R, Ng SC, Chan M, Gin T, Zee
B and Poon WS: Ultra-early (within 24 hours) aneurysm treatment
after subarachnoid hemorrhage. World Neurosurg. 77:311–315. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Haug T, Sorteberg A, Finset A, Lindegaard
KF, Lundar T and Sorteberg W: Cognitive functioning and
health-related quality of life 1 year after aneurysmal subarachnoid
hemorrhage in preoperative comatose patients (Hunt and Hess grade V
patients). Neurosurgery. 66:475–485. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nieuwkamp DJ, de Gans K, Algra A, Albrecht
KW, Boomstra S, Brouwers PJ, Groen RJ, Metzemaekers JD, Nijssen PC,
Roos YB, et al: Timing of aneurysm surgery in subarachnoid
haemorrhage - an observational study in The Netherlands. Acta
Neurochir (Wien). 147:815–821. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Natarajan SK, Sekhar LN, Ghodke B, Britz
GW, Bhagawati D and Temkin N: Outcomes of ruptured intracranial
aneurysms treated by microsurgical clipping and endovascular
coiling in a high-volume center. AJNR Am J Neuroradiol. 29:753–759.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Molyneux AJ, Kerr RS, Birks J, Ramzi N,
Yarnold J, Sneade M and Rischmiller J: ISAT Collaborators: Risk of
recurrent subarachnoid haemorrhage, death, or dependence and
standardised mortality ratios after clipping or coiling of an
intracranial aneurysm in the International Subarachnoid Aneurysm
Trial (ISAT): Long-term follow-up. Lancet Neurol. 8:427–433. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ohashi Y, Horikoshi T, Sugita M, Yagishita
T and Nukui H: Size of cerebral aneurysms and related factors in
patients with subarachnoid hemorrhage. Surg Neurol. 61:239–247.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Murayama Y, Malisch T, Guglielmi G, Mawad
ME, Viñuela F, Duckwiler GR, Gobin YP, Klucznick RP, Martin NA and
Frazee J: Incidence of cerebral vasospasm after endovascular
treatment of acutely ruptured aneurysms: Report on 69 cases. J
Neurosurg. 87:830–835. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Abbed KM and Ogilvy CS: Intracerebral
hematoma from aneurysm rupture. Neurosurg Focus.
15:E42003.PubMed/NCBI
|
|
26
|
Prat R and Galeano I: Early surgical
treatment of middle cerebral artery aneurysms associated with
intracerebral haematoma. Clin Neurol Neurosurg. 109:431–435. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sasaki T, Sato M, Oinuma M, Sakuma J,
Suzuki K, Matsumoto M and Kodama N: Management of poor-grade
patients with aneurysmal subarachnoid hemorrhage in the acute
stage: Importance of close monitoring for neurological grade
changes. Surg Neurol. 62:531–537. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen JH, Wang YH, Yang LK, Shi ZH, Cai S,
Zhou JX and Feng Y: Analysis the prognosis factors of microsurgical
treatment for poor-grade aneurysms associated with hematoma. Zhong
Hua Shen Jing Wai Ke Za Zhi. 31:158–160. 2015.(In Chinese).
|
|
29
|
Yin YH, Wang F, Pan YH, Wang Y, Wang Y,
Luo QZ and Jiang JY: Effect of dose-response of topical
administration of nimodipine on cerebral vasospasm following
subarachnoid hemmorrhage in rabbits. Am J Med Sci. 337:123–125.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shirao S, Yoneda H, Kunitsugu I, Ishihara
H, Koizumi H, Suehiro E, Nomura S, Kato S, Fujisawa H and Suzuki M:
Preoperation prediction of outcome in 283 poor-grade patients with
subarachnoid hemorrhage: A project of the Chugoku-Shikoku Division
of the Japan Neurosurgical Society. Cerebrovasc Dis. 30:105–113.
2010. View Article : Google Scholar : PubMed/NCBI
|