Introduction
Angiosarcoma accounts for ~2% of soft tissue
sarcomas (1). Epithelioid
angiosarcoma is a rare type of angiosarcoma that was first reported
by Ng et al in 1996 (2).
Epithelioid angiosarcoma occurs in various sites, including the
skin, head and neck, lungs, breasts, adrenal glands, bones and deep
soft tissue in the extremities (3–8).
Epithelioid angioma has a male predilection and typically occurs in
adults, with the highest incidence being in the seventh decade of
life (4). Treatment modalities
include surgical resection of the primary tumor, radiation therapy
and chemotherapy (4–6). Within 2–3 years of diagnosis, ~50% of
patient succumb to disease, however, 20–30% of patients are free of
disease (4,9). Advanced age, increased tumor size and a
retroperitoneal primary site are considered to be adverse
prognostic factors (9). Although
pathological examination is the gold standard of diagnosis,
radiological studies may provide assistance for determining the
treatment choice and assessing the prognosis (10). Magnetic resonance imaging (MRI)
reveals the infiltration of the lesion, and computed tomography
(CT) angiography (CTA) reveals the involvement of the arteries in
the lower extremities, which determines whether or not thrombosis
is present (3,4). The current study presents the imaging
analysis of a patient with epithelioid angiosarcoma that occurred
in the deep soft tissue of the lower extremities. Written informed
consent was obtained from the patient.
Case report
A 44-year-old woman presented at the Department of
Radiology, The Affiliated Hospital of Xuzhou Medical College
(Jiangsu, China) on September 16, 2012 with soreness in the medial
side of the right thigh, which had developed over 2 months. Almost
1 month later, a mass had evolved at the painful site; however, the
pain was not associated with exertion. A physical examination
revealed an increased temperature on the medial side, at the
mid-shaft of the femur. The mass was ~5.0×4.0 cm in size, palpable,
hard, red and swollen, although there was no evident varicosity.
The mass had undefined margins and was not easy to move. A vascular
murmur was also identified, but no notable sensory loss on the skin
and good peripheral circulation were identified.
Following an X-ray, multiple osteolytic lesions
involving the cortex and medullary cavity, with defined margins,
were identified in the right femur (Fig.
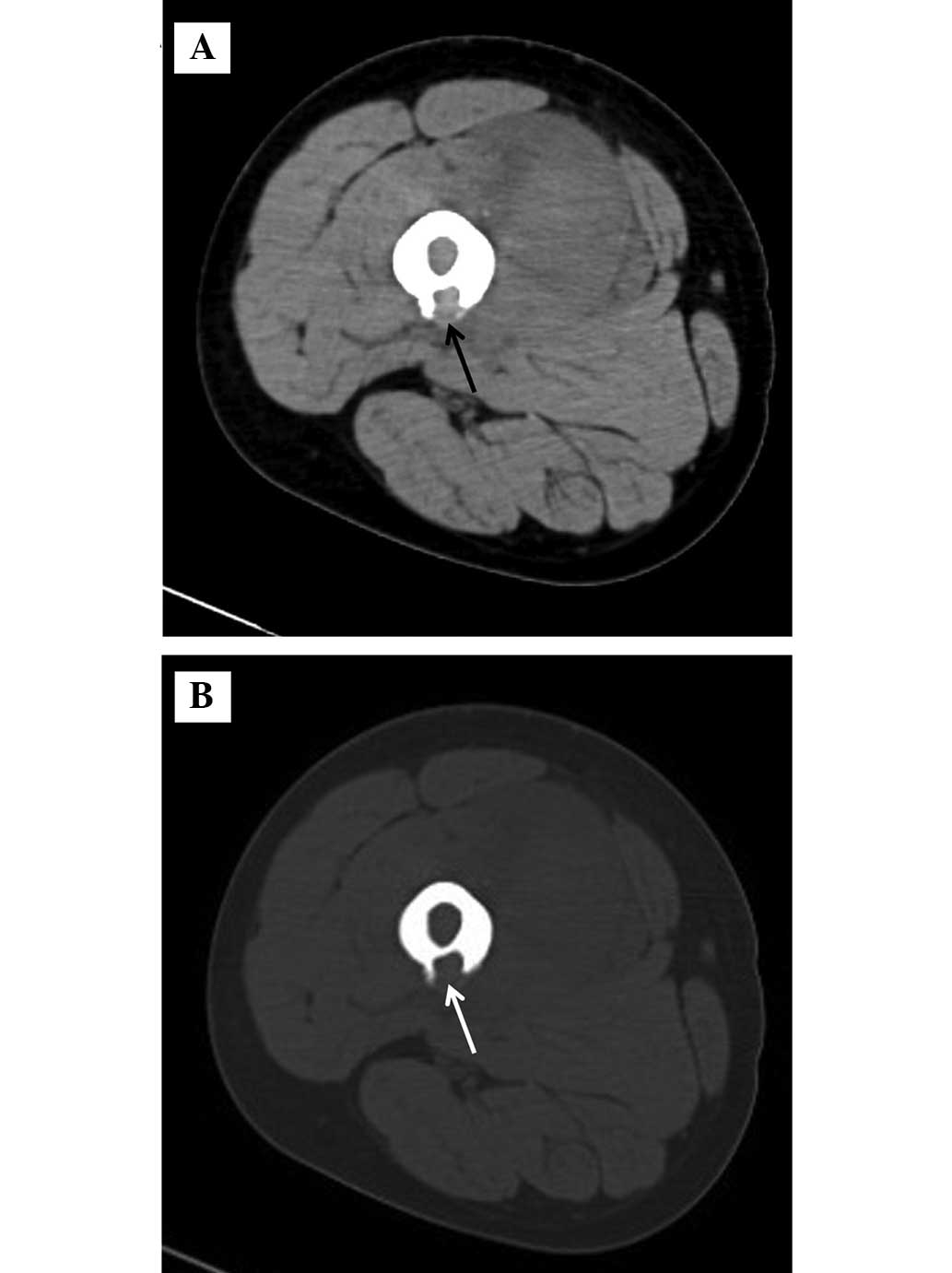
1). The CT scan revealed that the lesions were centered in the
medial aspect of the quadriceps muscle group, affecting the vastus
medialis and intermedius muscles of the soft tissue window, with
decreased heterogeneous density and a blurred intermuscular plane
(Fig. 2A). The CT scan revealed the
presence of osteolytic lesions on the right femoral cortex of the
bone window, the inside of which had a soft tissue density
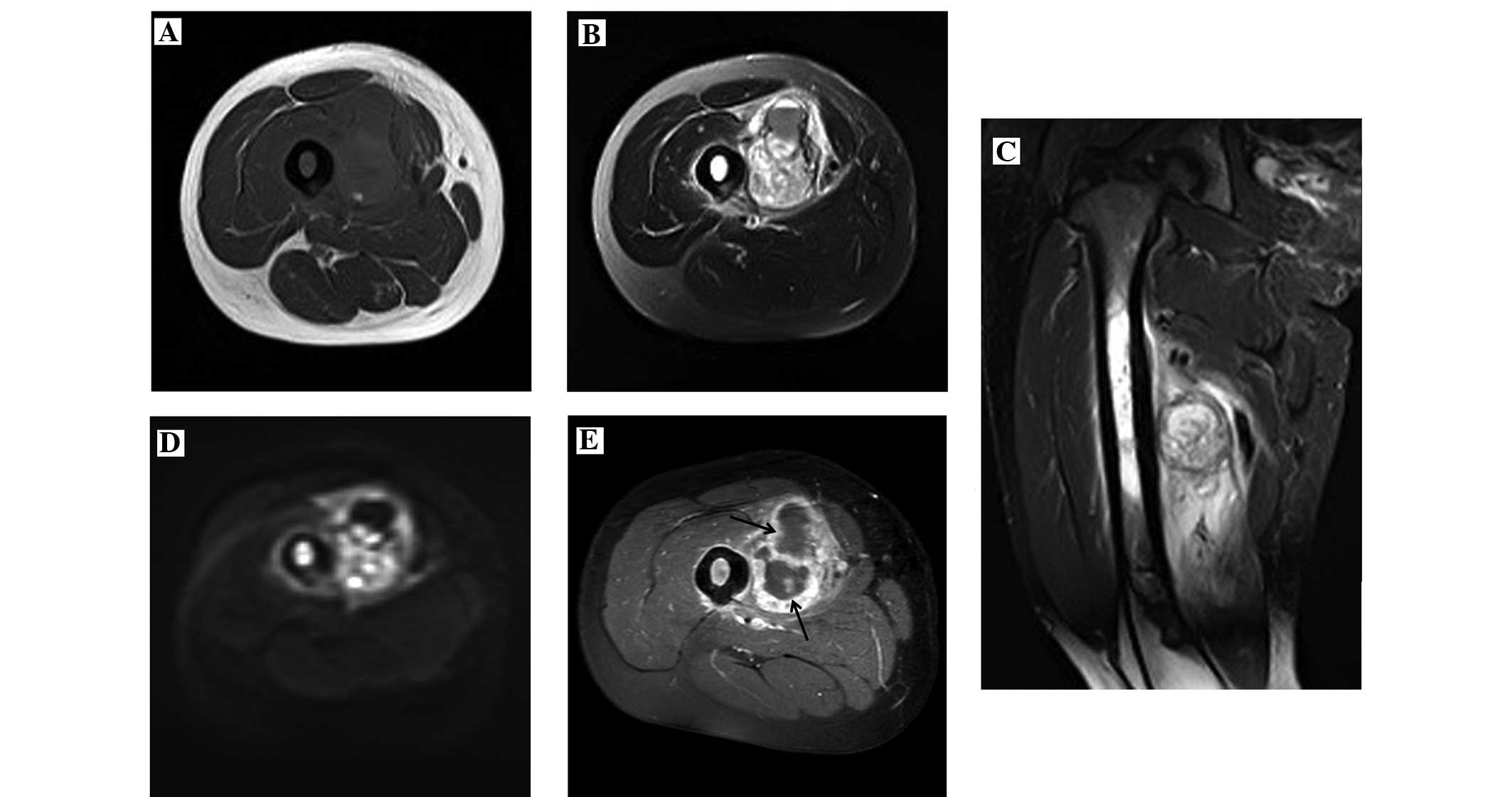
(Fig. 2B). The findings of the MRI
scan were as follows: T1 weighted image (WI) sequence identified a
mass with a low signal that was located in the adductor group of
the right femur (Fig. 3A); and the
T2WI sequence identified a mass with a slightly increased signal
that was surrounded by a low-signal capsule, and adjacent muscles
demonstrated a large patch with a slightly high signal with
undefined margins (Fig. 3B and C);
the diffusion weighted imaging sequence revealed a heterogeneous
high signal (Fig. 3D). An enhanced
MRI scan demonstrated a heterogeneous enhancement of the mass,
possessing undefined demarcation with adjacent normal muscle tissue
and non-enhanced necrosis inside the lesion (Fig. 3E).
The mass was located in the adductor group of the
right thigh, with an intact capsule and sufficient blood supply. A
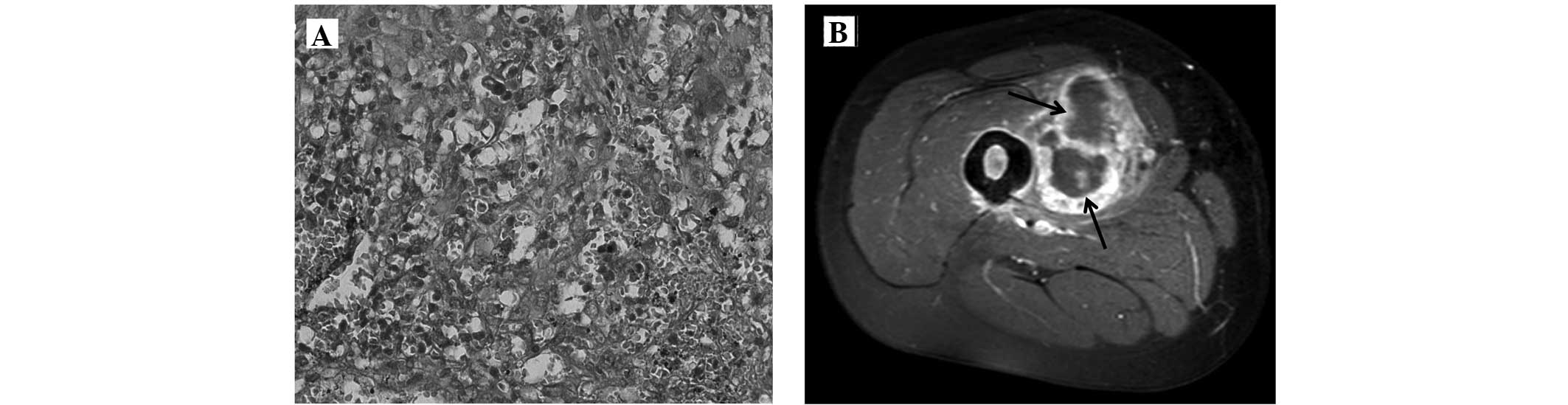
biopsy of the lesion was performed. Hematoma and necrosis were
present inside the tumor mass. Hematoxylin and eosin (Nanjing
Jiancheng Bioengineering Institute, Nanjing, China) staining
revealed epithelioid tumor cells that were oval or irregular in
shape with abundant eosinophilic cytoplasms, unequal and vacuolar
nuclei and certain notable nucleoli (Fig.
4A). Immunohistochemistry (Nanjing Jiancheng Bioengineering
Institute, Nanjing, China) revealed the presence of cluster of
differentiation (CD)-31 (Fig. 4B),
CD34, 2-keto-6-phosphate-D-gluconic acid, factor VIII and ki-67
(80%) in the carcinoma cells. The pathological diagnosis was
epithelioid angiosarcoma.
Since the patient did not undergo amputation
surgery, palliative surgery was adopted and the tumor was excised,
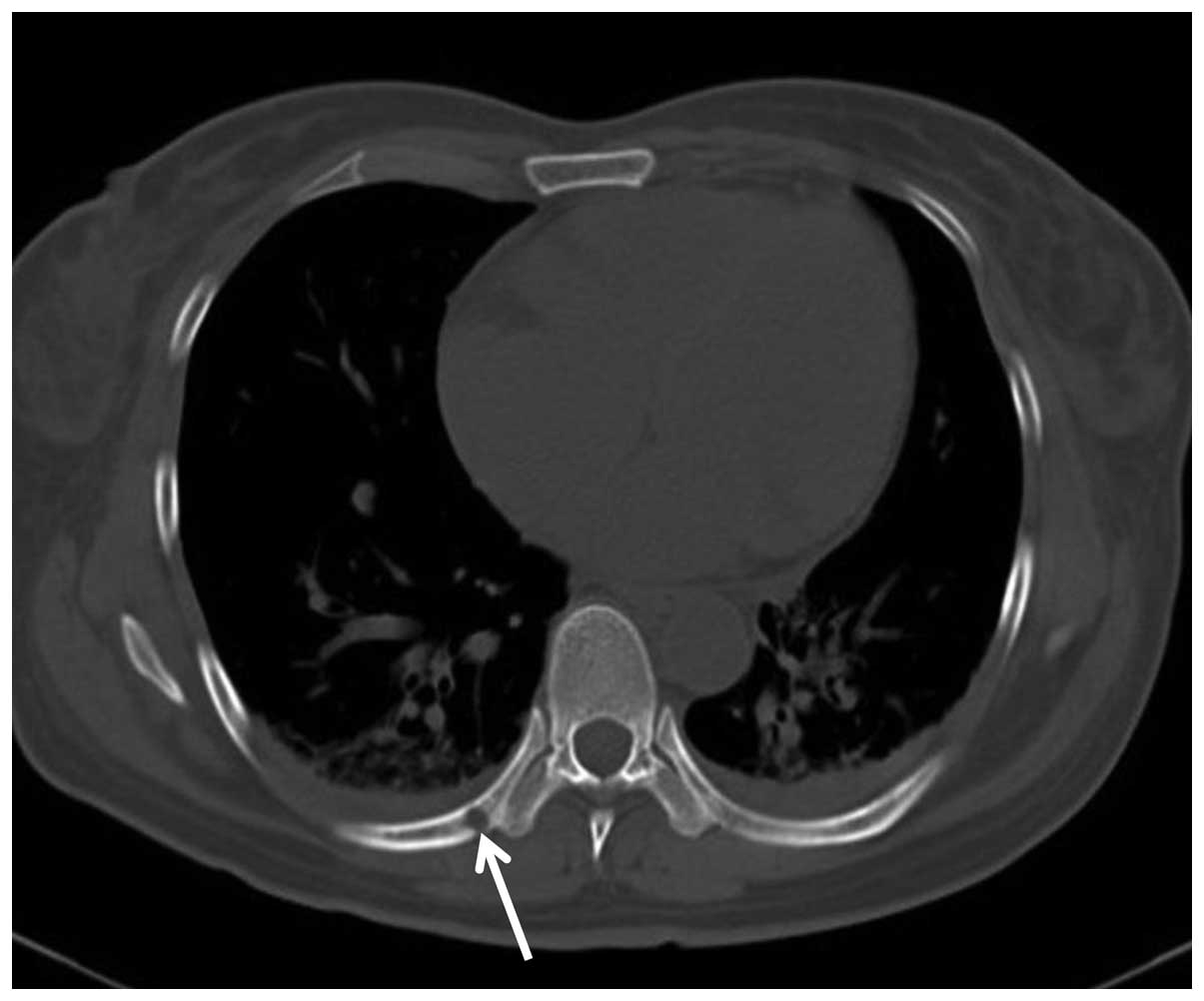
followed by chemotherapy. Thrombosis was observed in the femoral
artery of the leg following the surgery. In total, 6 months
subsequent to surgery, multiple osteolytic lesions on the right
ribs and metastases on the lungs were located by a CT scan
(Fig. 5). By the 1-year follow-up,
the patient had succumbed to the carcinoma.
Discussion
The majority of epithelioid angiosarcomas occur in
males and the incidence peaks at ~70 years of age (9). The clinical manifestations of
epithelioid angiosarcomas vary depending on the sites of the
lesions (10). A tumor diagnosis must
be corroborated by immunohistochemical analysis. Classical tumor
cells reveal the presence of CD31, CD34 and factor VIII (11). In the early stages, epithelioid
angiosarcomas are able to metastasize to lymph nodes and
parenchymal organs, particularly the lung, bone and soft tissue
(1,3).
In total, >50% of patients succumb to the disease within 2–3
years of a confirmed diagnosis (4,9). Treatment
varies according to the patient, but radical excision combined with
radiotherapy is generally considered to be the routine method
(12,13). According to certain studies, lesion
containment and limb preservation using radiotherapy may be
beneficial to primary or relapsed tumors; however, the survival
rate is not increased (4,7,14).
Imaging features of epithelioid angiosarcoma in the
deep soft tissue of the lower extremities are usually identified by
X-ray, CT and MRI. X-ray usually reveals that the soft tissue is
swollen with osteolytic destruction on the adjacent cortex, while
the CT scan demonstrates that the lesions manifest as soft tissue
masses with undefined margins and blurred adjacent intermuscular
planes. CT bone window scans are superior to X-rays, due to the
improved evaluation of bone destruction. Lower extremity CTAs aid
the evaluation of the association between masses and arteries,
identification of the origin of the tumor and selection of a
surgical approach (10). MRI scans
allow evaluation of the tumor infiltration and internal structure.
In the present study, the epithelioid angiosarcoma mass manifested
as a mottled, increased signal on T1WI MRI, suggesting an abundant
blood supply and predisposition to internal hemorrhage (4). An enhanced MRI scan may reveal the
infiltration level of a lesion. In the current study, an enhanced
MRI scan of the lesion demonstrated that there was significant
enhancement of the solid component of the tumor, and the
enhancement region was much more extensive compared with the
routine MRI scan. This provided information concerning the amount
of radical excision to be performed by the surgeon. Non-enhanced
regions inside a tumor, as demonstrated by an enhanced MRI scan,
suggest rapid growth with ischemia and local necrosis (15).
In order to provide an accurate prognosis and
correct treatment of epithelioid angiosarcomas, the tumors are
classified into two categories. Primary tumors are those that have
been diagnosed for the first time without metastasis and are
generally resectable. Developing tumors are those that are
diagnosed for the first time with metastases or those that are
unresectable (16). It has been
reported that the average survival time for a developing tumor is
~7.3 months (16).
It is important to eliminate differential diagnoses
of epithelioid angiosarcomas when diagnosing soft tissue masses in
the lower extremities. Hemangiomas in the lower extremities are
mainly plexiform cavernous hemangiomas. On T1WI MRI, these
demonstrate an equal or slightly increased signal, while T2WI MRI
reveals a high signal without bone destruction on adjacent
structures, along with defined margins with adjacent soft tissue.
Fibrosarcomas mainly occur in the elderly, and these exhibit
relatively low signals on T1WI and T2WI MRI. The enhancement of
fibrosarcomas is generally not significant compared with
epithelioid angiosarcomas when using an MRI enhancement scan.
Metastasis generally occurs in elderly patients, who are usually
predisposed to pathological fractures. Metastases are not
challenging to identify based on clinical symptoms and primary
lesions. In clinical practice, if a pampiniform abnormal density
signal is identified in tubular bones with evident enhancement on a
MRI scan, along with adjacent bone destruction, it is crucial for
the clinician to consider a diagnosis of epithelioid angiosarcoma.
Phlebolith-like calcifications or hemorrhaging also supports this
diagnosis. However, the gold standard for diagnosing epithelioid
angiosarcomas remains pathological examination (10).
In summary, there are specific imaging features that
can be used in the diagnosis of epithelioid angiosarcomas of the
soft tissue of the lower extremities. The present study aimed to
improve the understanding of this disease for radiologists.
Together, X-ray, CT and MRI scans may be effective in diagnosing
epithelioid angiosarcomas by eliminating differential diagnosis of
other soft tissue masses of the lower extremities.
References
|
1
|
Cafiero F, Gipponi M, Peressini A,
Queirolo P, Bertoglio S, Comandini D, Percivale P, Sertoli MR and
Badellino F: Radiation-associated angiosarcoma: Diagnostic and
therapeutic implications - two case reports and a review of the
literature. Cancer. 77:2496–2502. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ng WK, Collins RJ, Law D and Gwi E:
Cutaneous epithelioid angiosarcoma: A potential diagnostic trap for
cytopathologists. Diagn Cytopathol. 16:160–166; discussion 166–167.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Asmane I, Litique V, Heymann S, Marcellin
L, Métivier AC, Duclos B, Bergerat JP and Kurtz JE: Adriamycin,
cisplatin, ifosfamide and paclitaxel combination as front-line
chemotherapy for locally advanced and metastatic angiosarcoma.
Analysis of three case reports and review of the literature.
Anticancer Res. 28(5B): 3041–3045. 2008.PubMed/NCBI
|
|
4
|
Deshpande V, Rosenberg AE, O'Connell JX
and Nielsen GP: Epithelioid angiosarcoma of the bone: A series of
10 cases. Am J Surg Pathol. 27:709–716. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lund L and Amre R: Epithelioid
angiosarcoma involving the lungs. Arch Pathol Lab Med. 129:e7–e10.
2005.PubMed/NCBI
|
|
6
|
Goldblum JR and Rice TW: Epithelioid
angiosarcoma of the pulmonary artery. Hum Pathol. 26:1275–1277.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ghanem N, Riede U, Uhrmeister P, Weigang E
and Altehoefer C: Epithelioid angiosarcoma of the aorta. Vasa.
31:269–273. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Macías-Martínez V, Murrieta-Tiburcio L,
Molina-Cárdenas H and Domínguez-Malagón H: Epithelioid angiosarcoma
of the breast. Clinicopathological, immunohistochemical, and
ultrastructural study of a case. Am J Surg Pathol. 21:599–604.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Meis-Kindblom JM and Kindblom LG:
Angiosarcoma of soft tissue: A study of 80 cases. Am J Surg Pathol.
22:683–697. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hart J and Mandavilli S: Epithelioid
angiosarcoma: A brief diagnostic review and differential diagnosis.
Arch Pathol Lab Med. 135:268–272. 2011.PubMed/NCBI
|
|
11
|
Callister MD, Ballo MT, Pisters PW, Patel
SR, Feig BW, Pollock RE, Benjamin RS and Zagars GK: Epithelioid
sarcoma: Results of conservative surgery and radiotherapy. Int J
Radiat Oncol Biol Phys. 51:384–391. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lăzureanu C, Baderca F, Burlacu O and
Nicodin A: Soft tissue epithelioid angiosarcoma. Rom J Morphol
Embryol. 51:787–792. 2010.PubMed/NCBI
|
|
13
|
Lydiatt WM, Shaha AR and Shah JP:
Angiosarcoma of the head and neck. Am J Surg. 168:451–454. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mendeszoon MJ, Mendeszoon ER Jr, Rasmussen
S, Bell J and Harris SY: Epithelioid angiosarcoma of the talus. J
Foot Ankle Surg. 50:87–92. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bürk J, Gerlach U, Baumann T, Langer M and
Winterer JT: Epithelioid angiosarcoma of the scapula. In Vivo.
24:783–786. 2010.PubMed/NCBI
|
|
16
|
Abraham JA, Hornicek FJ, Kaufman AM,
Harmon DC, Springfield DS, Raskin KA, Mankin HJ, Kirsch DG,
Rosenberg AE, Nielsen GP, et al: Treatment and outcome of 82
patients with angiosarcoma. Ann Surg Oncol. 14:1953–1967. 2007.
View Article : Google Scholar : PubMed/NCBI
|