Lung cancer remains one of the most common types of
cancer worldwide (1.8 million novel cases were diagnosed in 2012,
13% of the total cancer cases diagnosed), and it was the leading
cause of cancer-associated mortality in 2012 (1.59 million
mortalities; 19.4% of all cancer-associated mortalities in 2012)
(1). Conventional platinum-based
chemotherapy has reached a plateau in improving patient survival
and disease control obtained with classic doublet chemotherapy in
patients with advanced lung cancer is usually restricted to a few
months (2–4). Fortunately, developments in molecular
biology have attracted attention to the molecular subtypes of lung
cancer, resulting in great improvements in understanding the
disease, including the identification of mutations in the epidermal
growth factor receptor (EGFR).
The majority of EGFR mutations are located at exon
19, which are deletions (Del-19), and exon 21 (L858R), and
mutations at these sites account for 45 and 40% of all EGFR
mutations, respectively (5). These
mutations are considered to be sensitizing mutations that confer
sensitivity to EGFR-tyrosine kinase inhibitors (EGFR-TKIs),
including gefitinib and erlotinib (6–8). Clinical
trials have demonstrated that EGFR-TKIs are associated with a
significantly increased response rate (RR) and progress free
survival (PFS) rate for patients harboring EGFR sensitizing
mutations, as compared with chemotherapy alone (9,10). To
date, the detection of EGFR mutations has been performed prior to
the treatment of advanced non-squamous NSCLC, while an increasing
number of rare types of EGFR mutations have been discovered, which
are not only limited to the mutation of a single exon, but the
concurrence of two mutations on different exons, primarily exons
18–21, in a single tumor sample (11,12). These
mutations are termed ‘complex mutations’. However, the response of
patients harboring the complex EGFR mutations to first-line
EGFR-TKIs remains unclear. The present study reports a case of a
patient with advanced NSCLC and complex EGFR mutations, and the
patient's response to first-line EGFR-TKI treatment. Written
informed consent was obtained from the patient for the publication
of the present study.
On March 10, 2014, a 62-year-old, non-smoking woman
with an Eastern Cooperative Oncology Group Performance Status score
of 2 (13) presented to the
Department of Oncology, Comprehensive Cancer Center of Drum-Tower
Hospital (Nanjing, China) with a cough that had been ongoing for 2
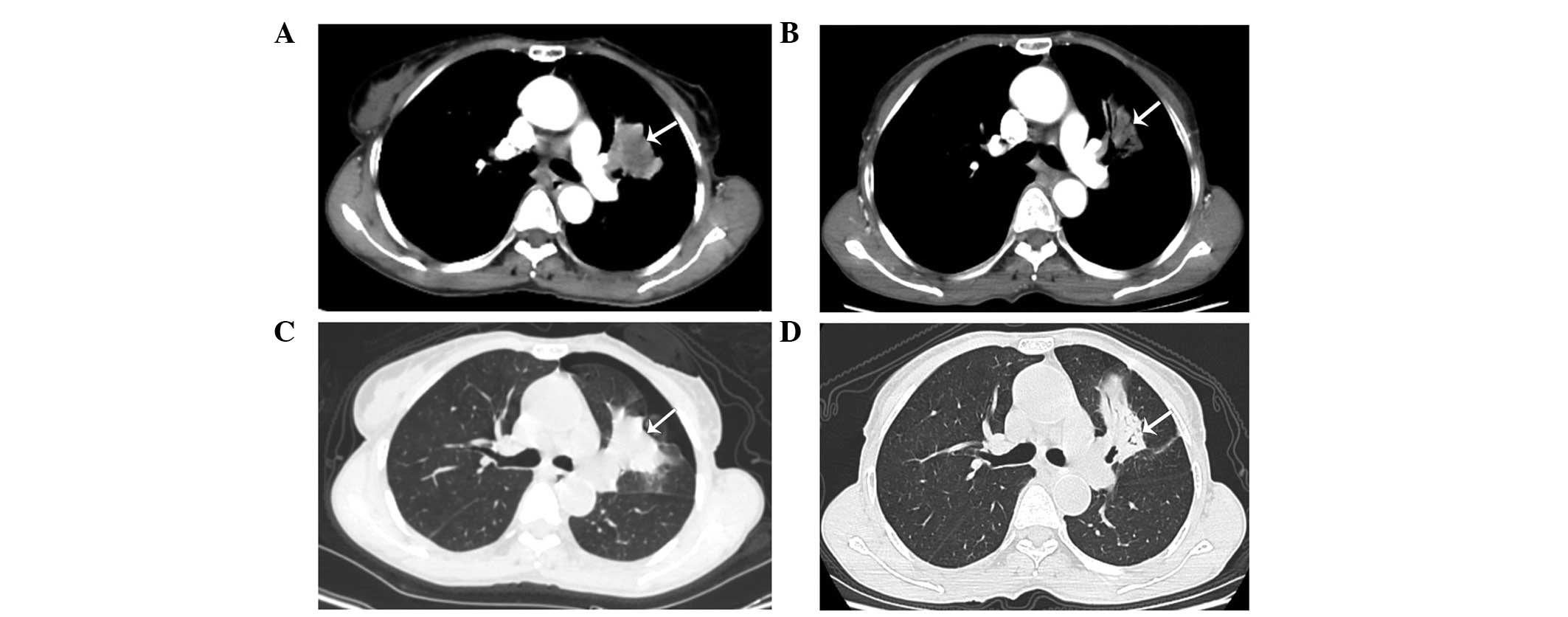
months. Computed tomography (CT; Discovery CT750 HD; GE Healthcare
Life Sciences, Shanghai, China) revealed a primary mass in the left
upper lobe of the lung (Fig. 1A and
B), with multiple small pulmonary nodules (maximum diameter, 4
mm) observed bilaterally. A CT-guided fine needle aspiration biopsy
of the primary lesion was performed on the left lung, which
revealed the presence of a middle-differentiated adenocarcinoma.
EGFR mutation analysis was performed on the biopsied tissue within
exons 18 and 21. EGFR mutations were detected by amplification
refractory mutation system in multiple quantitative polymerase
chain reaction analysis with the Human EGFR Mutation Detection kit
(YuanQi Bio-Pharmaceutical Co., Ltd., Shanghai, China), as
previously described (14), which
demonstrated a co-mutant of Del-19 (del 2239_2248+insC) and L858R.
In addition, anaplastic lymphoma kinase rearrangement analysis was
performed using fluorescence in situ hybridization, with
negative results. The patient was orally administered erlotinib, at
a dose of 150 mg/day. Two months later, no considerable relief of
the cough was noted; however, a CT scan revealed that the primary
lung mass had shrunk (Fig. 1C and D),
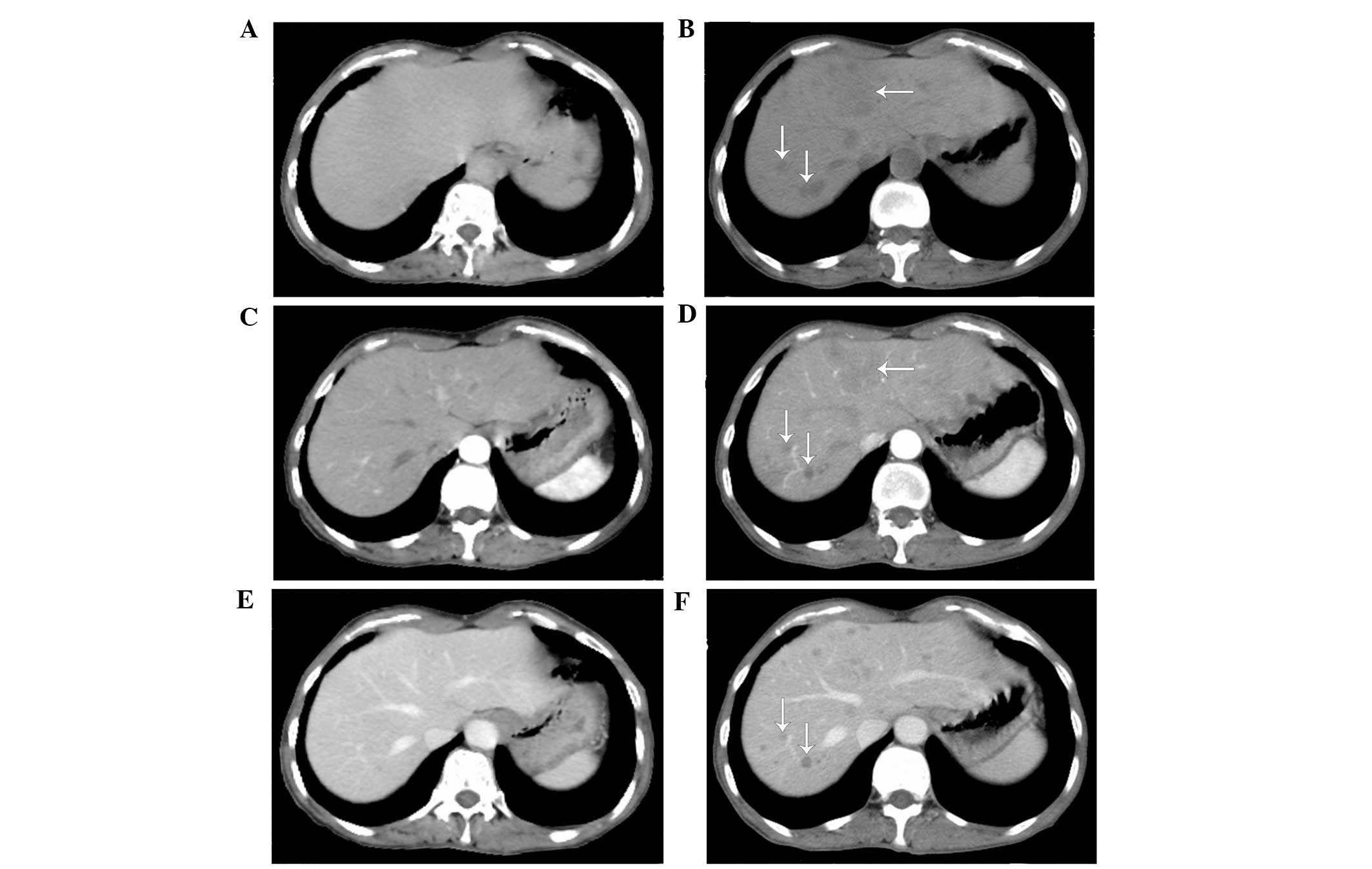
but the bilateral multiple pulmonary nodules remained. In addition,
prior to erlotinib treatment there was no hepatic metastases
(Fig. 2A–C); however, following
treatment multiple hepatic metastases were observed (Fig. 2D–F). Based on the Response Evaluation
Criteria in Solid Tumors (RECIST) (15), the treatment response of the patient
was assessed as progressive disease (PD). The patient refused to
undergo a biopsy of the liver. Treatment with erlotinib was stopped
when PD was detected, and 2 cycles (3 weeks/cycle) of chemotherapy
with pemetrexed (500 mg/m2) plus cisplatin (75
mg/m2) were administered to the patient intravenously.
However, the hepatic metastases continued to progress under the
assessment of CT scans, which were performed monthly. The patient
succumbed 2 months subsequent to the detection of PD, with the best
supportive care possible. The patient's overall survival was ~5.3
months.
The use of first-line EGFR-TKIs in NSCLC patients
with EGFR sensitizing mutations has been demonstrated to be
superior to chemotherapy in terms of PFS, RR and quality of life;
however, previous phase III clinical trials primarily enrolled
patients harboring common EGFR mutations, including exon 19
deletion or exon 21 L858R (16). For
patients who exhibit uncommon mutations, particularly complex 19+21
mutations, the efficacy of first-line EGFR-TKIs remains unknown.
Despite the fact that the present patient harbored Del-19 and
L858R, which are sensitizing EGFR mutations, the patient
experienced PD following treatment with first-line erlotinib. In
order to acquire an improved understanding of this, the present
study performed a comprehensive search of relevant studies
published on the PubMed database (www.ncbi.nlm.nih.gov/pubmed) using keywords, including
‘complex mutations’, ‘double mutations’, ‘compound mutations’,
‘multiple mutations’, ‘rare mutations’ and ‘uncommon mutations’,
with ‘EGFR’ added to each keyword. All studies with relevant
abstracts (1,949 abstracts) were retrieved first, and the full
texts of those that were considered valuable, including studies
that contained patients carrying complex, double, compound,
multiple, rare or uncommon mutations of EGFR, were carefully
reviewed (27 studies). Relevant references from the searched
studies (6 references) were also reviewed.
In total, 18 patients with EGFR Del-19 + L858R
mutations that received EGFR-TKIs were identified between January
2002 and January 2015 (Table I)
(17–22). Of these 18, 16 patients were assessed
based on RECIST (15) and 2 patients
were not evaluated. The 18 patients presented in Table I exhibited the following responses: 2
(11.1%), complete response; 10 (55.6%), partial response; 2
(11.1%), stable disease; 2 (11.1%), PD; and 2 patients (11.1%) that
were not evaluated experienced a relief of their symptoms. Only 2
out of the 18 patients experienced PD following the initiation of
EGFR-TKIs, and these patients were administered EGFR-TKIs as
second-line treatment, following first-line carboplatin and
paclitaxel regimens. Compared with patients harboring EGFR
mutations that were administered first-line EGFR-TKIs, those who
received EGFR-TKIs as second-line treatment following
platinum-based chemotherapy exhibited a lower response rate
(23,24). A study by Bai et al (25) demonstrated that prior chemotherapy may
reduce the EGFR mutation rate in the plasma, suggesting that the
poor response of the 2 aforementioned patients with PD may be
associated with the first-line chemotherapy each received.
The present patient had concurrent EGFR19+21
sensitizing mutations and received EGFR-TKI as a first-line
treatment; however, the patient had PD following treatment.
Previously, genetic heterogeneity of tumors has received
considerable attention. Studies on clear cell renal carcinoma have
demonstrated substantial intratumor heterogeneity of mutations in
known cancer genes (26,27), which suggests that a single biopsy of
a tumor may be inadequate to detect all cancer gene mutations,
resulting in inconsistencies between detection and clinical
efficacy. By contrast, a recent study by Zhang et al
(28) on lung adenocarcinoma
demonstrated that 76% of mutations were detected in various regions
of the same tumor, indicating that single-region biopsy may
compromise the intratumor heterogeneity to an acceptable extent,
therefore identifying the majority of cancer gene mutations in
localized lung adenocarcinomas.
In the present case, the EGFR gene detection assay
on the core biopsy tissue of the primary lesion in the left lung
revealed Del-19 and L858R mutations. Notably, following the
initiation of EGFR-TKI treatment the primary lung mass shrunk and
hepatic metastases appeared extensively. The present study
hypothesizes that the genomic features of the hepatic metastases
varied from those of the primary tumor, indicating that intertumor
heterogeneity may be responsible for the PD observed in the present
patient. In addition, de Bruin et al (29) revealed evidence of branched evolution
with driver mutations arising prior to and following subclonal
diversification, which supports the hypothesis of the present
authors. Considering that the majority of NSCLC driver mutations
occur in the early phases of tumor evolution (29), the Del-19 + L858R mutations of the
present patient may have been truncal mutations of the ancestral
clone, existing only in the primary lung lesion. With regard to the
hepatic metastases, it is likely that they consisted of sectional
and predominant subclones with branch gene alternations that confer
de novo resistance to EGFR-TKIs, including
phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit α,
phosphatase and tensin homolog, protein kinase B and
serine/threonine kinase 11 alterations, c-met amplification,
hepatocyte growth factor overexpression and Kirsten ras mutations
(30–34). Under circumstances when re-biopsy is
not feasible, comprehensive genomic detection and multi-targeted
therapies may be used. It has been suggested that liquid biopsy may
reveal relatively comprehensive gene alternations and provide
predictive information on the identification of therapeutic targets
and resistance mechanisms (35).
To the best of our knowledge, this is the first
study of a treatment-naive NSCLC patient harboring complex EGFR
19+21 sensitizing mutations presenting with de novo
resistance to first-line EGFR-TKI treatment. Previous studies have
suggested that NSCLC patients harboring complex EGFR 19+21
mutations usually have good response to EGFR-TKIs; however, in
order to understand the complexity of EGFR mutations and determine
the efficacy of EGFR-TKIs against them, large-scale clinical trials
are required.
The present study was supported by the Health
Scientific Research Project of Jiangsu Province, Nanjing, China
(grant no. H201235) and Key Project of Nanjing Medical Science and
Technology Development Foundation, Nanjing, China (grant no.
ZKX12012).
|
1
|
Ferlay JSI, Ervik M, Dikshit R, Eser S,
Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: GLOBOCAN 2012
v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No.
11 (Internet). International Agency for Research on Cancer (Lyon,
France). 2013.http://globocan.iarc.frAccessed. January
23–2015
|
|
2
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH: Eastern
Cooperative Oncology Group: Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Scagliotti GV, De Marinis F, Rinaldi M,
Crinò L, Gridelli C, Ricci S, Matano E, Boni C, Marangolo M, Failla
G, et al: Phase III randomized trial comparing three platinum-based
doublets in advanced non-small-cell lung cancer. J Clin Oncol.
20:4285–4291. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fossella F, Pereira JR, von Pawel J,
Pluzanska A, Gorbounova V, Kaukel E, Mattson KV, Ramlau R, Szczesna
A, Fidias P, et al: Randomized, multinational, phase III study of
docetaxel plus platinum combinations versus vinorelbine plus
cisplatin for advanced non-small-cell lung cancer: The TAX 326
study group. J Clin Oncol. 21:3016–3024. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shigematsu H, Lin L, Takahashi T, Nomura
M, Suzuki M, Wistuba II, Fong KM, Lee H, Toyooka S and Shimizu N:
Clinical and biological features associated with epidermal growth
factor receptor gene mutations in lung cancers. J Natl Cancer Inst.
97:339–346. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pao W, Miller V, Zakowski M, Doherty J,
Politi K, Sarkaria I, Singh B, Heelan R, Rusch V, Fulton L, et al:
EGF receptor gene mutations are common in lung cancers from ‘never
smokers’ and are associated with sensitivity of tumors to gefitinib
and erlotinib. Proc Natl Acad Sci USA. 101:13306–13311. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gerber DE, Gandhi L and Costa DB:
Management and future directions in non-small cell lung cancer with
known activating mutations. Am Soc Clin Oncol Educ Book. e353–e365.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee JY, Lim SH, Kim M, Kim S, Jung HA,
Chang WJ, Choi MK, Hong JY, Lee SJ, Sun JM, et al: Is there any
predictor for clinical outcome in EGFR mutant NSCLC patients
treated with EGFR TKIs? Cancer Chemother Pharmacol. 73:1063–1070.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Huang SF, Liu HP, Li LH, Ku YC, Fu YN,
Tsai HY, Chen YT, Lin YF, Chang WC, Kuo HP, et al: High frequency
of epidermal growth factor receptor mutations with complex patterns
in non-small cell lung cancers related to gefitinib responsiveness
in Taiwan. Clin Cancer Res. 10:8195–8203. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hsieh MH, Fang YF, Chang WC, Kuo HP, Lin
SY, Liu HP, Liu CL, Chen HC, Ku YC, Chen YT, et al: Complex
mutation patterns of epidermal growth factor receptor gene
associated with variable responses to gefitinib treatment in
patients with non-small cell lung cancer. Lung Cancer. 53:311–322.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Huang SW, Ho CF, Chan KW, Cheng MC, Shien
JH, Liu HJ and Wang CY: The genotyping of infectious bronchitis
virus in Taiwan by a multiplex amplification refractory mutation
system reverse transcription polymerase chain reaction. J Vet Diagn
Invest. 26:721–733. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT and Christian MC: New guidelines to evaluate the
response to treatment in solid tumors. European organization for
research and treatment of cancer, national cancer institute of the
united states, national cancer institute of Canada. J Natl Cancer
Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al: Spanish Lung Cancer Group in
collaboration with Groupe Français de Pneumo-Cancérologie and
Associazione Italiana Oncologia Toracica: Erlotinib versus standard
chemotherapy as first-line treatment for European patients with
advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial.
Lancet Oncol. 13:239–246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhang GC, Lin JY, Wang Z, Zhou Q, Xu CR,
Zhu JQ, Wang K, Yang XN, Chen G, Yang JJ, et al: Epidermal growth
factor receptor double activating mutations involving both exons 19
and 21 exist in Chinese non-small cell lung cancer patients. Clin
Oncol (R Col Radiol). 19:499–506. 2007. View Article : Google Scholar
|
|
18
|
Masago K, Fujita S, Kim YH, Ichikawa M,
Hatachi Y, Fukuhara A, Nagai H, Irisa K, Mio T and Mishima M:
Epidermal growth factor receptor (EGFR) double-activating somatic
mutations in exons 19 and 21 in Japanese non-small cell lung cancer
patients. Cancer Genet Cytogenet. 195:179–182. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Masago K, Togashi Y, Fukudo M, Terada T,
Irisa K, Sakamori Y, Fujita S, Kim YH, Mio T and Inui K: Good
clinical response to erlotinib in a non-small cell lung cancer
patient harboring multiple brain metastases and a double active
somatic epidermal growth factor gene mutation. Case Rep Oncol.
3:98–105. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Keam B, Kim DW, Park JH, Lee JO, Kim TM,
Lee SH, Chung DH and Heo DS: Rare and complex mutations of
epidermal growth factor receptor and efficacy of tyrosine kinase
inhibitor in patients with non-small cell lung cancer. Int J Clin
Oncol. 19:594–600. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Peng L, Song ZG and Jiao SC: Efficacy
analysis of tyrosine kinase inhibitors on rare non-small cell lung
cancer patients harboring complex EGFR mutations. Sci Rep.
4:61042014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hata A, Yoshioka H, Fujita S, Kunimasa K,
Kaji R, Imai Y, Tomii K, Iwasaku M, Nishiyama A and Ishida T:
Complex mutations in the epidermal growth factor receptor gene in
non-small cell lung cancer. J Thorac Oncol. 5:1524–1528. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shepherd FA, Rodrigues Pereira J, Ciuleanu
T, Tan EH, Hirsh V, Thongprasert S, Campos D, Maoleekoonpiroj S,
Smylie M, Martins R, et al: Erlotinib in previously treated
non-small-cell lung cancer. N Engl J Med. 353:123–132. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Thatcher N, Chang A, Parikh P, Rodrigues
Pereira J, Ciuleanu T, von Pawel J, Thongprasert S, Tan EH,
Pemberton K and Archer V: Gefitinib plus best supportive care in
previously treated patients with refractory advanced non-small-cell
lung cancer: Results from a randomised, placebo-controlled,
multicentre study (iressa survival evaluation in lung cancer).
Lancet. 366:1527–1537. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bai H, Wang Z, Chen K, Zhao J, Lee JJ,
Wang S, Zhou Q, Zhuo M, Mao L, An T, et al: Influence of
chemotherapy on EGFR mutation status among patients with
non-small-cell lung cancer. J Clin Oncol. 30:3077–3083. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gerlinger M, Rowan AJ, Horswell S, Larkin
J, Endesfelder D, Gronroos E, Martinez P, Matthews N, Stewart A,
Tarpey P, et al: Intratumor heterogeneity and branched evolution
revealed by multiregion sequencing. N Engl J Med. 366:883–892.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gerlinger M, Horswell S, Larkin J, Rowan
AJ, Salm MP, Varela I, Fisher R, McGranahan N, Matthews N, Santos
CR, et al: Genomic architecture and evolution of clear cell renal
cell carcinomas defined by multiregion sequencing. Nat Genet.
46:225–233. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang J, Fujimoto J, Zhang J, Wedge DC,
Song X, Zhang J, Seth S, Chow CW, Cao Y, Gumbs C, et al: Intratumor
heterogeneity in localized lung adenocarcinomas delineated by
multiregion sequencing. Science. 346:256–259. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
de Bruin EC, McGranahan N, Mitter R, Salm
M, Wedge DC, Yates L, Jamal-Hanjani M, Shafi S, Murugaesu N, Rowan
AJ, et al: Spatial and temporal diversity in genomic instability
processes defines lung cancer evolution. Science. 346:251–256.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lee SY, Kim MJ, Jin G, Yoo SS, Park JY,
Choi JE, Jeon HS, Cho S, Lee EB, Cha SI, et al: Somatic mutations
in epidermal growth factor receptor signaling pathway genes in
non-small cell lung cancers. J Thorac Oncol. 5:1734–1740. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Benedettini E, Sholl LM, Peyton M, Reilly
J, Ware C, Davis L, Vena N, Bailey D, Yeap BY, Fiorentino M, et al:
Met activation in non-small cell lung cancer is associated with de
novo resistance to EGFR inhibitors and the development of brain
metastasis. Am J Pathol. 177:415–423. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yano S, Yamada T, Takeuchi S, Tachibana K,
Minami Y, Yatabe Y, Mitsudomi T, Tanaka H, Kimura T, Kudoh S, et
al: Hepatocyte growth factor expression in EGFR mutant lung cancer
with intrinsic and acquired resistance to tyrosine kinase
inhibitors in a Japanese cohort. J Thorac Oncol. 6:2011–2017. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ludovini V, Bianconi F, Pistola L, Chiari
R, Minotti V, Colella R, Giuffrida D, Tofanetti FR, Siggillino A,
Flacco A, et al: Phosphoinositide-3-kinase catalytic alpha and KRAS
mutations are important predictors of resistance to therapy with
epidermal growth factor receptor tyrosine kinase inhibitors in
patients with advanced non-small cell lung cancer. J Thorac Oncol.
6:707–715. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Shih JY, Gow CH and Yang PC: EGFR mutation
conferring primary resistance to gefitinib in non-small-cell lung
cancer. N Engl J Med. 353:207–208. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rolfo C, Castiglia M, Hong D, Alessandro
R, Mertens I, Baggerman G, Zwaenepoel K, Gil-Bazo I, Passiglia F,
Carreca AP, et al: Liquid biopsies in lung cancer: The new ambrosia
of researchers. Biochim Biophys Acta. 1846:539–546. 2014.PubMed/NCBI
|