Introduction
Cardiac metastasis is relatively common in malignant
neoplasms such as lung cancer, breast cancer, melanoma and
lymphoma, with an incidence rate of ~10–15% (1). In contrast to these types of malignancy,
cardiac metastasis of uterine cervical cancer is rare (1–4). In
autopsy cases of uterine cervical cancer, the incidence rate of
cardiac metastasis has been reported to be 0.3–8.0% (1–4). Cardiac
metastasis of uterine cervical cancer diagnosed prior to mortality
(antemortem) is much rarer, as only 4.0% of cardiac metastasis
cases are diagnosed antemortem (5).
Among them, solitary metastasis to the heart is particularly rare,
since cardiac metastasis is usually the result of the hematogenous
spread of systemically disseminated disease (6). In the present study, a case of solitary
cardiac metastasis of uterine cervical cancer diagnosed antemortem
is reported, and a review of the literature is conducted.
Case report
A 78-year-old woman with squamous cell carcinoma
(SCC) of the uterine cervix [Federation of Gynecology and
Obstetrics stage IIIb (7)] underwent
definitive radiotherapy in January 2013 at Gunma University
Hospital (Gunma, Japan). The Eastern Cooperative Oncology
Group/World Health Organization performance status (PS) (8) of the patient was 1. At the time of
diagnosis, magnetic resonance imaging (MRI; Signa HDxt 1.5T; GE
Healthcare Japan, Tokyo, Japan) revealed a bulky tumor (66×56×45
mm) at the uterine cervix with right parametrial invasion reaching
the right pelvic wall. Computed tomography (CT; Aquilion ONE/ViSION
Edition; Toshiba Medical Systems, Tochigi, Japan) and fluorine-18
fluorodeoxyglucose positron emission tomography (PET; Aquiduo
PCA-7000B; Toshiba Medical Systems) indicated no evidence of
metastasis, with the exception of an enlarged right obturator lymph
node. Laboratory tests demonstrated elevated levels (110.0 µg/l;
normal range, <3.5 µg/l) of serum SCC antigen. Radiotherapy
(ONCOR Impression Plus; Siemens Japan, Tokyo, Japan) consisted of
external beam radiotherapy and intracavitary brachytherapy. For
external beam radiotherapy, whole pelvic irradiation of 50 Gy was
delivered in 25 fractions over 5 weeks (the final 20 Gy dose was
delivered using the central shielding technique), followed by boost
irradiation to the right obturator lymph node of 6 Gy in 3
fractions at Gunma University Hospital. Weekly high-dose rate
intracavitary brachytherapy using iridium-192 (Chiyoda Technol
Corporation, Tokyo, Japan) delivered 24 Gy to point A (2 cm along
the tandem from the external cervical os and 2 cm lateral to the
tandem) in 4 fractions (over a duration of 7 weeks). Chemotherapy
was not performed due to the advanced age of the patient. Five
months after completion of the treatment, gynecologic examination
of the uterine cervix and total body CT examination revealed no
evidence of recurrence or metastasis. In addition, serum SCC
antigen had decreased to levels of 0.8 µg/l, which are within the
normal limit.
In April 2014, the patient was admitted to our
hospital with epigastric discomfort and general malaise, rapidly
worsening over 3 days. The patient had a PS of 2, in addition to
high blood pressure (152/115 mmHg; normal range, <140/90 mmHg)
and tachycardia (101 beats/min; normal range, 60–90 beats/min).
Chest X-ray (RADSpeed Safire; Shimadzu Corporation, Kyoto, Japan)
revealed enlargement of the heart (cardiothoracic ratio, 65%;
normal range, <50%). These findings suggested heart failure.
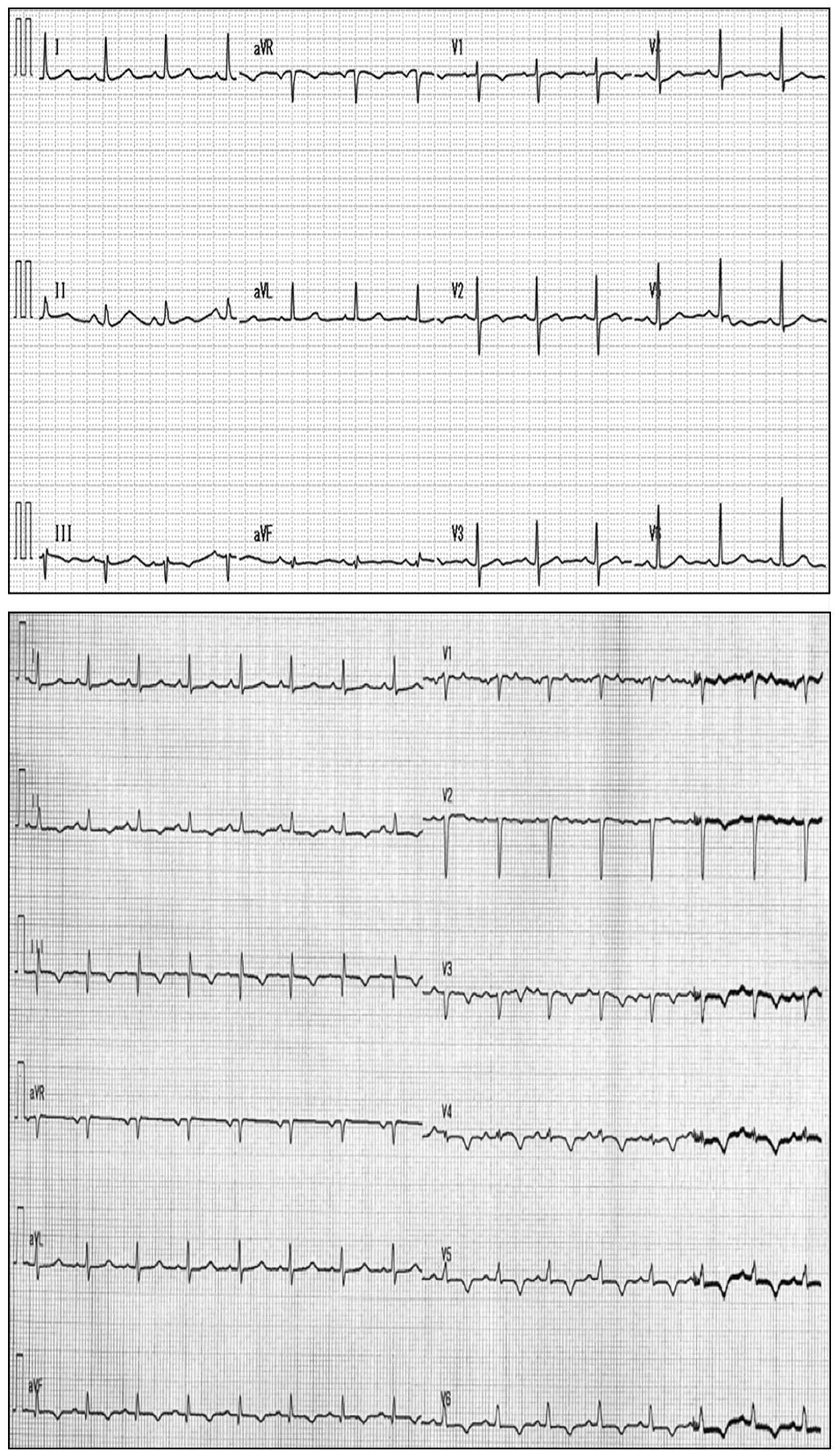
Electrocardiogram (Vivid E9; Fukuda M-E Kogyo Co., Ltd., Tokyo,
Japan) displayed low-voltage amplitudes in leads V1-V6 and T-wave
inversion in leads V3-V6 (Fig. 1),
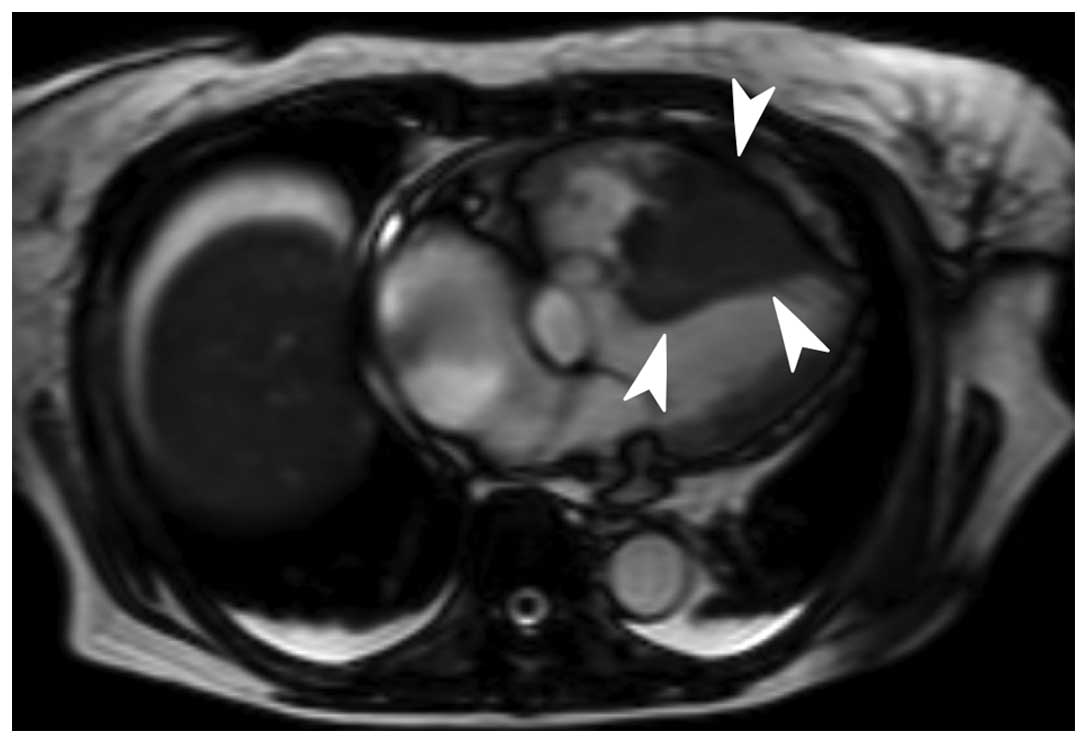
suggesting myocardial dysfunction. Transthoracic echocardiography
(Cardisuny 630; GE Healthcare Life Sciences) revealed the presence
of a mass occupying the right ventricle and pericardial effusion,
while cine MRI demonstrated a filling defect in the right ventricle
(Fig. 2). These findings suggested
the presence of a tumor in the right ventricle. A transcatheter
biopsy from the right ventricle confirmed SCC. The levels of serum
SCC antigen had elevated to 40.8 µg/l. Total body CT examination
indicated no evidence of local recurrence or metastasis to sites
other than the heart. Taken together, these findings led to the
diagnosis of solitary cardiac metastasis of uterine cervical
cancer. Elevated levels of fibrin degradation products (>20.0
µg/ml; normal range, 0–4.0 µg/ml), alongside thrombocytopenia
(1.1×104 cells/µl; normal range, 16–35×104
cells/µl) suggested disseminated intravascular coagulation (DIC)
(9). Following admission, the
hemodynamic status of the patient worsened gradually. Despite
aggressive medical therapy, including intravenous administration of
dobutamine (Shionogi, Inc., Osaka, Japan), noradrenaline (Daiichi
Sankyo, Tokyo, Japan) and thrombomodulin alpha (Asahi Kasei, Tokyo,
Japan), and transfusion of platelets and fresh frozen plasma
(Japanese Red Cross Society, Tokyo, Japan) for a week, the patient
succumbed to disease 31 days after admission to hospital.
Permission for an autopsy was not granted at the time of mortality,
although the patient had provided written informed consent for
publication of the present case.
Discussion
In the present study, a case of solitary cardiac
metastasis of uterine cervical cancer diagnosed antemortem is
reported. To the best of our knowledge, there have been only 18
cases of cardiac metastasis of uterine cervical cancer reported in
the literature thus far (Table I,
Fig. 3) (1,6,10–24). The
number of cases showing solitary metastasis to the heart, as in the
present case, is even smaller; with only nine cases reported to
date (6,10,14,16–18,22–24).
The clinical stage at the time of initial diagnosis varied widely
among the case reports published in the literature, ranging from
stage I to IV (1,6,10–24). Cardiac metastasis occurred within 1
year after completion of the initial treatment in 63% of patients,
and within 2 years in 84% of patients (1,6,10–24). This
indicates that the 2 years subsequent to the completion of the
initial treatment is a critical period during which uterine
cervical cancer patients should be carefully monitored for symptoms
of cardiac metastasis. Dyspnea and chest pain were frequently
reported as chief complaints in patients with cardiac metastasis
(1,6,11–13,16,18,20–23).
Electrocardiogram frequently exhibited low voltages and T-wave
abnormalities in chest leads, which is indicative of myocardial
disability and/or pericardial effusion (10,13,14,17,19,21–23).
Echocardiography revealed a right ventricular mass in the majority
of cases (1,6,10–12,14,16–18,20–24).
In the present case, it was not obvious to suspect cardiac
metastasis from the complaints of epigastric discomfort and general
malaise exhibited by the patient. Electrocardiogram revealed
low-voltage amplitudes and T-wave inversion in chest leads, and
echocardiograpy detected a mass in the right ventricle, which
enabled to reach a diagnosis of cardiac metastasis. However, based
on the current case and previous cases reported in the literature,
no particular characteristics of solitary metastasis to the heart
could be identified. Recent translational research indicates that
molecules such as matrix metalloproteinase (MMP)-2 and MMP-9, and
molecules associated with epithelial-mesenchymal transition such as
Snail and vimentin, participate in cancer metastasis (25–28), which
may be further elucidated via immunohistochemical analysis of these
proteins. Taken together, the current case and the previous cases
reported in the literature suggest that: i) Cardiac metastasis
should be included in the differential diagnosis of patients with a
history of uterine cervical cancer (particularly if diagnosed
within the previous 2 years) who present with nonspecific
complaints such as epigastric discomfort and general malaise; and
ii) electrocardiogram and echocardiography are convenient and
effective modalities for the diagnosis of cardiac metastasis.
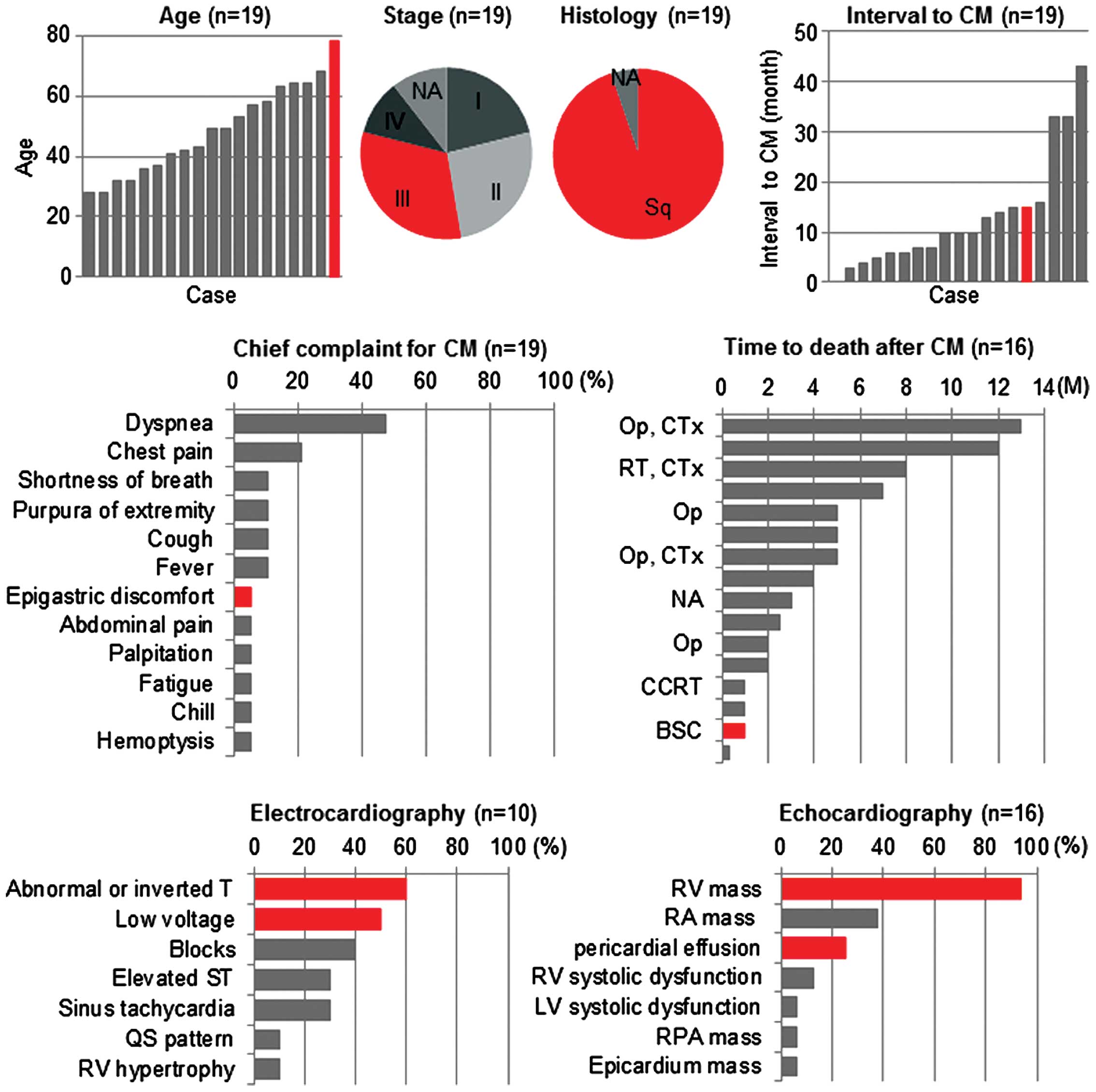 | Figure 3.Graphical representation of the
current and previously reported cases of cardiac metastasis of
uterine cervical cancer diagnosed antemortem, indicating the
patients' characteristics, examination findings, treatment modality
and prognosis. Detailed information is described in Table I. The current case is indicated in
red. NA, not available; Sq, squamous cell carcinoma; CM, cardiac
metastasis; Op, operation; CTx, chemotherapy; RT, radiation
therapy; CCRT, concurrent chemoradiotherapy; BSC, best supportive
care; RV, right ventricle; RA, right atrium; LV, left ventricle;
RPA, right pulmonary artery; M, months. |
 | Table I.Review of the literature reporting
cardiac metastasis of uterine cervical cancer diagnosed
antemortem. |
Table I.
Review of the literature reporting
cardiac metastasis of uterine cervical cancer diagnosed
antemortem.
| Age (years) | Histology | Stage | Primary Tx | Time to CM
(months) | Chief complaint for
CM |
Electrocardiogram | Echocardiography | Metastatic site other
than the heart | Biopsy method for
CM | Recurrence Tx | Time to mortality
from CM (months) | Refs. |
|---|
| 64 | Sq | IB | Op, CCRT | 7 | Dyspnea, cough | NA | RA mass, RV mass,
pericardial efffusion | Uterine cervix,
mediastinum, abdominal wall |
Pericardiocentesis | CCRT | 2.0 | (1) |
| 32 | Sq | IIA | Op, CCRT | 15 | Dyspnea, purpura of
extremity | NA | RA mass, RV mass | – | Op | Op, CTx | 13.0 | (6) |
| 28 | Sq | IIB | Op, RT | 10 | – | ST elevation (V1-V4),
T-wave inversion (III) | RV mass, pericardial
effusion | – | Percutaneous
myocardial biopsy | NA | 3.0 | (10) |
| 28 | Sq | NA | Op, CCRT | 16 | Dyspnea, chest
pain | NA | RV mass,
pericardial effusion | Mediastinal LN | Autopsy | CTx |
1.0 |
(11) |
| 32 | Sq | IIB | CTx | 4 | Dyspnea,
hemoptysis, chill, fever | Right ventricular
hypertrophy | RA mass, RV
mass | Pleura | Op | Op | NA | (12) |
| 36 | Sq | IB | Op, CTx | 33 | Chest pain | CRBBB, ST elevation
(II, III, aVF, V1-V6), T-wave inversion (V3-V4) | NA | Lung, paraaortic
LN | Percutaneous
myocardial biopsy | CTx | NA | (13) |
| 37 | Sq | IIIB | CCRT | 3 | – | Sinus tachycardia,
low voltage, T-wave abnormality | RV mass, epicardial
mass | – | – | RT, CTx | >8.0 | (14) |
| 41 | Sq | IIB | Op, RT | 12 | Abdominal pain | IRBBB | NA | Uterine cervix | CT-guided
biopsy | CTx |
5.0 | (15) |
| 42 | Sq | IVB | RT | 6 | Chest pain | NA | RA mass, RV mass,
RV outflow obstruction | – | Op | Op | NA | (16) |
| 43 | Sq | IIB | RT | 5 | Ventricular
fibrillation | Sinus tachycardia,
AV block-I, IRBBB, T-wave abnormality | RV mass, RV/LV
systolic dysfunction | – | Percutaneous
myocardial biopsy | CTx | NA | (17) |
| 49 | Sq | IIIB | RT | 6 | Dyspnea | NA | RV mass | – | – | CCRT |
7.0 | (18) |
| 53 | Sq | IB | RT, Op | 14 | Dyspnea | NA | RV mass | Lung | Autopsy | CCRT |
1.0 | (18) |
| 49 | Sq | IVB | CCRT | 0 | Cough, fever | Sinus tachycardia,
low voltage (limb leads), T-wave inversion (V1-V4) | NA | Abdominal LN | Percutaneous
myocardial biopsy | CCRT |
2.5 | (19) |
| 57 | Sq | IIIB | CCRT | 10 | Shortness of
breath, chest pain | NA | RV mass | Paraaortic LN | Op | Op |
2.0 | (20) |
| 58 | Sq | IB | Op, CTx | 43 | Dyspnea, purpura of
extremity | Low voltages (limb
and chest leads), SI/QIII/TIII pattern | RA mass, RV mass,
RPA mass | Paraaortic LN | Op | Op |
4.0 | (21) |
| 63 | NA | NA | Op, CCRT | 33 | Dyspnea,
fatigue | Low voltage, T-wave
inversion (V3, V4) | RV mass, RV
mobility reduction | – | Op | Op | >5.0 | (22) |
| 64 | Sq | IIIB | RT | 7 | Dyspnea | Low voltage | RA mass, RV
mass | – | Autopsy | BSC |
0.3 | (23) |
| 68 | Sq | IIIB | RT | 10 | Shortness of
breath, palpitation | NA | RV mass | – | Op | Op, CTx |
5.0 | (24) |
| 78 | Sq | IIIB | RT | 15 | Epigastric
discomfort | Low voltage (chest
leads), T-wave abnormality (V3-V6) | RV mass,
pericardial effusion | – | Percutaneous
myocardial biopsy | BSC |
1.0 | Current case |
The treatment strategy for cardiac metastasis of
uterine cervical cancer has not been standardized to date, which is
probably due to the extremely low incidence and the unfavorable
prognosis of this disease (1). A
review of the relevant literature suggests that the efficacy of
aggressive treatment is controversial (1,6,10–24).
Several reports suggest that aggressive treatment may prolong the
patients' survival time (6,18). For example, Byun et al
(6) reported that a 32-year-old woman
who underwent an open excision of an intracardiac tumor, followed
by chemotherapy using carboplatin and paclitaxel, survived for 13
months after the diagnosis of cardiac metastasis. Lemus et
al (18) reported that a
49-year-old woman who received 60 Gy of radiotherapy for an
intracardiac tumor, combined with concurrent administration of
5-fluorouracil and cisplatin, survived for 7 months after the
diagnosis of cardiac metastasis. By contrast, there are also
reports indicating that aggressive treatment of cardiac metastasis
does not always prolong the survival time of patients (Fig. 3) (1,18,19). In several cases, intense concurrent
chemoradiotherapy resulted in a survival time of only 3 months
(1,18,19). Thus,
aggressive treatment to cardiac metastasis may not prolong the
survival time when the patient develops systemic metastasis,
although aggressive treatment could be beneficial if the cardiac
metastasis is solitary (1,6,18,19). Recent advances in diagnostic
modalities, such as CT and PET, and their widespread use may
increase the diagnostic yield of antemortem cardiac metastases,
which may be controlled by aggressive treatment. In the present
case, aggressive treatment such as surgery, radiotherapy or
chemotherapy could not be performed due to the patient's unstable
hemodynamic status and DIC. Therefore, the treatment strategy for
cardiac metastasis of uterine cervical cancer should be carefully
considered on a case-by-case basis.
In summary, the current case and the review of the
literature conducted in the present study indicate that cardiac
metastasis should be included in the differential diagnosis of
patients with nonspecific complaints such as epigastric discomfort
and general malaise, particularly if the patient has a previous
history of uterine cervical cancer. In such cases,
electrocardiogram and echocardiography may be convenient and
effective modalities for the diagnosis of cardiac metastasis.
Acknowledgements
The present study was supported by the Strategic
Young Researcher Overseas Visits Program for Accelerating Brain
Circulation of the Japan Society for the Promotion of Science
(Tokyo, Japan).
References
|
1
|
Kim HS, Park NH and Kang SB: Rare
metastases of recurrent cervical cancer to the pericardium and
abdominal muscle. Arch Gynecol Obstet. 278:479–482. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Badib AO, Kurohara SS, Webster JH and
Pickren JW: Metastasis to organs in carcinoma of the uterine
cervix. Influence of treatment on incidence and distribution.
Cancer. 21:434–439. 1968. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Peeples WJ, Inalsingh CH, Hazra TA and
Graft D: The occurrence of metastasis outside the abdomen and
retroperitoneal space in invasive carcinoma of the cervix. Gynecol
Oncol. 4:307–310. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Klatt EC and Heitz DR: Cardiac metastases.
Cancer. 65:1456–1459. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Greenwald EF, Breen JL and Gregori CA:
Cardiac metastases associated with gynecologic malignancies.
Gynecol Oncol. 10:75–83. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Byun SW, Park ST, Ki EY, Song H, Hong SH
and Park JS: Intracardiac metastasis from known cervical cancer: A
case report and literature review. World J Surg Oncol. 11:1072013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Oken MM, Creech RH, Tormey DC, et al:
Toxicity and response criteria of the Eastern Cooperative Oncology
Group. Am J Clin Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wada H, Gabazza EC, Asakura H, et al:
Comparison of diagnostic criteria for disseminated intravascular
coagulation (DIC): Diagnostic criteria of the International Society
of Thrombosis and Hemostasis and of the Japanese Ministry of Health
and Welfare for overt DIC. Am J Hematol. 74:17–22. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kountz DS: Isolated cardiac metastasis
from cervical carcinoma: Presentation as acute anteroseptal
myocardial infarction. South Med J. 86:228–230. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Senzaki H, Uemura Y, Yamamoto D, et al:
Right intraventricular metastasis of squamous cell carcinoma of the
uterine cervix: An autopsy case and literature review. Pathol Int.
49:447–452. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Krivokapich J, Warren SE, Child JS, et al:
M-mode and cross-sectional echocardiographic diagnosis of right
ventricular cavity masses. J Clin Ultrasound. 9:5–10. 1981.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shimotsu Y, Ishida Y, Fukuchi K, et al:
Fluorine-18-fluorodeoxyglucose PET identification of cardiac
metastasis arising from uterine cervical carcinoma. J Nucl Med.
39:2084–2087. 1998.PubMed/NCBI
|
|
14
|
Feys A, Herregods MC and Ector H: Cardiac
metastasis from a stage IIIb cervix carcinoma. Acta Cardiol.
60:73–75. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ando K, Kashihara K, Harada M, Kasem I,
Nishitani H, Sano N and Ohtani T: Carcinoma of the uterine cervix
with myocardial metastasis. Gynecol Oncol. 65:169–172. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Borsaru AD, Lau KK and Solin P: Cardiac
metastasis: A cause of recurrent pulmonary emboli. Br J Radiol.
80:e50–e53. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Batchelor WB, Butany J, Liu P and Silver
MD: Cardiac metastasis from primary cervical squamous cell
carcinoma: Three case reports and a review of the literature. Can J
Cardiol. 13:767–770. 1997.PubMed/NCBI
|
|
18
|
Lemus JF, Abdulhay G, Sobolewski C and
Risch VR: Cardiac metastasis from carcinoma of the cervix: Report
of two cases. Gynecol Oncol. 69:264–268. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Iwaki T, Kanaya H, Namura M, et al: Right
ventricular metastasis from a primary cervical carcinoma. Jpn Circ
J. 65:761–763. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nakao Y, Yokoyama M, Yasunaga M, et al:
Metastatic tumor extending through the inferior vena cava into the
right atrium: A case report of carcinoma of the uterine cervix with
para-aortic lymph node metastases. Int J Gynecol Cancer.
16:914–916. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Inamura K, Hayashida A, Kaji Y, et al:
Recurrence of cervical carcinoma manifesting as cardiac metastasis
three years after curative resection. Am J Med Sci. 328:167–169.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ferraz JG, Martins AL, de Souza JF, Matos
A, Canto AP and Martins AM: Metastatic tumor of squamous cell
carcinoma from uterine cervix to heart: Ante-mortem diagnosis. Arq
Bras Cardiol. 87:e104–e107. 2006.(In English, Portuguese).
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mohammed S and Khodadoust K: Carcinoma of
the cervix causing massive intracardiac embolus. Gynecol Oncol.
56:294–297. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Saitoh Y, Aota M, Koike H, Nakane T, Iwasa
Y and Konishi Y: Isolated right ventricular metastasis of uterine
cervical carcinoma. Jpn J Thorac Cardiovasc Surg. 53:645–648. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang C, Ma HX, Jin MS, et al: Association
of matrix metalloproteinase (MMP)-2 and −9 expression with
extra-gastrointestinal stromal tumor metastasis. Asian Pac J Cancer
Prev. 15:4187–4192. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chen L, Zhou Q, Xu B, Liu J, Shi L, Zhu D,
Wu C and Jiang J: MT2-MMP expression associates with tumor
progression and angiogenesis in human lung cancer. Int J Clin Exp
Pathol. 7:3469–3477. 2014.PubMed/NCBI
|
|
27
|
Lee MY and Shen MR: Epithelial-mesenchymal
transition in cervical carcinoma. Am J Transl Res. 4:1–13.
2012.PubMed/NCBI
|
|
28
|
Chen Z, Li S, Huang K, Zhang Q, Wang J, Li
X, Hu T, Wang S, Yang R, Jia Y, et al: The nuclear protein
expression levels of SNAI1 and ZEB1 are involved in the progression
and lymph node metastasis of cervical cancer via the
epithelial-mesenchymal transition pathway. Hum Pathol.
44:2097–2105. 2013. View Article : Google Scholar : PubMed/NCBI
|