Introduction
Primary glioblastoma (GBM) is the de novo
presentation of World Health Organization (WHO) grade IV glioma
without a preexisting lower grade tumor, and is the most frequent
glioma subtype, with aggressive progression and a poor prognosis
(1–3).
Genetic alterations, including mutations in epidermal growth factor
receptor (EGFR), altered AKT and mammalian target of rapamycin
signaling pathways, and environmental factors such as
cytomegalovirus infections, have been associated with an increased
risk of glioblastoma, but little is known about the induction of
the tumor (4,5). As GBM is one of the most resistant
tumors to radiation and chemotherapy (6–8), the most
effective treatment option is currently limited to surgical
resection; however, complete surgical removal of the tumor is
extremely difficult, since tumor cells invade the surrounding brain
(9). Better therapeutic approaches
are therefore urgently required.
To overcome the limitations of conventional
treatments, the emerging field of immunotherapy has been
investigated in GBM as a treatment option. Since mutant versions of
EGFR are frequently found in GBM tumors, specific peptides
contained in EGFR mutations have been investigated for use in
vaccines (10,11). However, a number of significant
challenges remain. GBM patients are profoundly immunosuppressive,
both locally within the tumor and systemically (12). Multiple mechanisms exist to suppress
effective immune responses targeted toward the tumor, including the
blood-brain barrier that restricts lymphocyte trafficking (13), the local production of
immunosuppressive cytokine transforming growth factor β (14,15), the
increased expression of B7-H1 in glioma and the induction of T-cell
apoptosis (16,17), the increased frequency of circulating
regulatory T cells (18) and
defective T-cell priming by microglial cells (19). On the other hand, stronger immune
responses are associated with lower glioma incidences and/or
increased survival. The incidence of glioma is inversely associated
with allergies (20–22). Patient survival has been positively
associated with the infiltration of effector T cells (23,24).
Coexpression network analysis has also linked a series of
immune-associated genes with GBM pathology and/or patient survival
(25). Together, these studies
suggest that an effective immune response mediated by
tumor-infiltrating cells in the immune system can positively impact
GBM outcome, but the manner in which to overcome the
immunosuppressive microenvironment in GBM tumors remains a
significant challenge for developing T-cell-based
immunotherapies.
The present study examined the functions of
tumor-infiltrating cluster of differentiation 3 (CD3)+ T
cells in resected GBM tumors. It was found that compared with
autologous peripheral blood CD3+ T cells,
tumor-infiltrating CD3+ T cells were highly refractory
to direct T-cell receptor stimulation by anti-CD3 antibodies, and
that using autologous blood antigen-presenting cells (APCs) did not
rescue the tumor T-cell responses. The study then investigated a
number of strategies to improve the tumor T-cell response in
vitro, and found that long-term interleukin (IL)-2 stimulation,
as well as depletion of IL-10 in culture, can rescue
tumor-infiltrating CD3+ T-cell proliferation in a subset
of GBM patients. The study also examined whether stimulating APCs
with Toll-like receptor (TLR) 4 ligand lipopolysaccharide (LPS) can
improve APC stimulation, and found that LPS stimulation on
autologous blood APCs did not improve the proliferation of the
tumor-infiltrating T cells. These results provided a viable
strategy for improving tumor-infiltrating CD3+ T-cell
responses in GBM patients.
Materials and methods
Subjects
A total of 23 GBM patients, graded according to the
WHO classification (2), were
recruited for the study, including 16 males between 33 and 52 years
of age, and 7 females between 35 and 55 years of age. No patients
were taking any other forms of medication at the time. All patients
provided written informed consent. The study was approved by the
Ethical Board of the General Hospital of Shenyang Military Area
Command of the Chinese People's Liberation Army (Shenyang,
Liaoning, China). Not all patients were included in all experiments
due to the low numbers of tumor-infiltrating T cells. Peripheral
blood samples were obtained on the day of diagnosis prior to any
treatment, and resected tumors were obtained by surgery. Efforts
were made by the neurosurgeon to preserve healthy brain tissues
during surgery, so small amounts of normal brain tissues were
available in only 5 patients. Peritumoral tissues were not
characterized as normal brain. Tumor and brain tissues were
inspected intraoperatively by experienced neurosurgeons to confirm
their identity prior to laboratory submission.
Sample preparation
Freshly isolated tumor tissue was mechanically
dissociated and passed through a 70-mm pore size mesh, followed by
collagenase digestion to obtain a single-cell suspension (19). For harvesting the brain/tumor
mononuclear cells, homogenized brain/tumor cells were centrifuged
across a 70–30% Percoll gradient at 500 × g for 30 min at 18°C, as
previously described (26). Efficacy
was confirmed by flow cytometry (Fig.
1A). For peripheral blood mononuclear cell (PBMC) isolation,
heparinized blood was subjected to Ficoll-Hypaque gradient
centrifugation. Purified peripheral blood APCs were obtained using
a Pan Monocyte Isolation kit following the manufacturer's
instructions (Miltenyi Biotec Inc., Cambridge, MA, USA) (27). Only fresh samples were used. The
culture medium used was RPMI 1640 supplemented with 10% fetal
bovine serum, 100 U/ml penicillin, 100 µg/ml streptomycin and 2mM
L-glutamine, unless otherwise specified.
Antibodies
For flow cytometry, cells were first labeled with
Fixable Violet Dead Cell Stain (Thermo Fisher Scientific Inc.,
Waltham, MA, USA), and then stained with fluorescently-labeled
anti-human CD3 [clone HIT3a; mouse immunoglobulin (Ig)G2aκ; catalog
no. 555339], CD4 (clone RPA-T4; mouse IgG1κ; catalog no. 560650)
and/or CD8 (clone RPA-T8; mouse IgG1κ; catalog no. 555369)
monoclonal antibodies obtained from BD Biosciences (Franklin Lakes,
NJ, USA), at 2 µg per 1 million cells. Forward scatter, side
scatter and surface antigen expression was assessed by FACS Calibur
(BD Biosciences). For stimulation, unlabeled anti-human CD3
monoclonal antibody (clone OKT3; mouse IgG2aκ; catalog no. 555329),
anti-human CD28 monoclonal antibody (clone CD28.2; mouse IgG1κ;
catalog no. 556620), anti-human IL-10 monoclonal antibody (clone
JES3-9D7; rat IgG1, catalog no. 554495) and isotype control (clone
R3-34; rat IgG1κ; catalog no. 554682) were added accordingly.
Proliferation assay
PBMCs or tumor leukocytes were labeled with
carboxyfluorescein succinimidyl ester (CFSE) according to the
manufacturer's protocol (Thermo Fisher Scientific Inc.), and then
placed in a 96-well plate at 105 cells per well in 200
µl culture medium. The cells were incubated for 6 days at 37°C in
5% CO2. Upon harvesting, the cells were stained with
surface antibodies, and the percentage of proliferating cells,
a.k.a., CFSElo cells, in all CD3+ T cells was
measured using FlowJo software (version 10.0.7r2; FlowJo LLC,
Ashland, OR, USA). For IL-2 pre-incubation, recombinant human IL-2
protein (Thermo Fisher Scientific Inc.) was added accordingly in
culture medium prior to CFSE-labeling. IL-2-containing medium was
replaced every 3 days for time course experiments for a maximum of
9 days. For LPS stimulation of APCs, purified peripheral blood APCs
were first incubated in culture medium with 2 µg/ml LPS for 3 days,
after which the APCs were washed and added to the CFSE-labeled
tumor cells.
Statistical analysis
Unequal variance t-tests were used for comparison
between two groups. One-way analysis of variance was used for
comparisons between multiple groups, and if the groups were
significantly different, Tukey's multiple comparisons test or
Dunnett's test was used. Paired tests were used for comparisons
between different conditions on the same sample from the same
subject. All statistical analyses were performed using Prism 6.0
software (GraphPad Software Inc., La Jolla, CA, USA). Bars
represent the mean ± standard deviation. P<0.05 was considered
to indicate a statistically significant difference.
Results
Tumor-infiltrating CD3+ T
cells are rare in GBM tumors and exhibit a lower CD8-to-CD4 ratio
than their peripheral blood counterparts
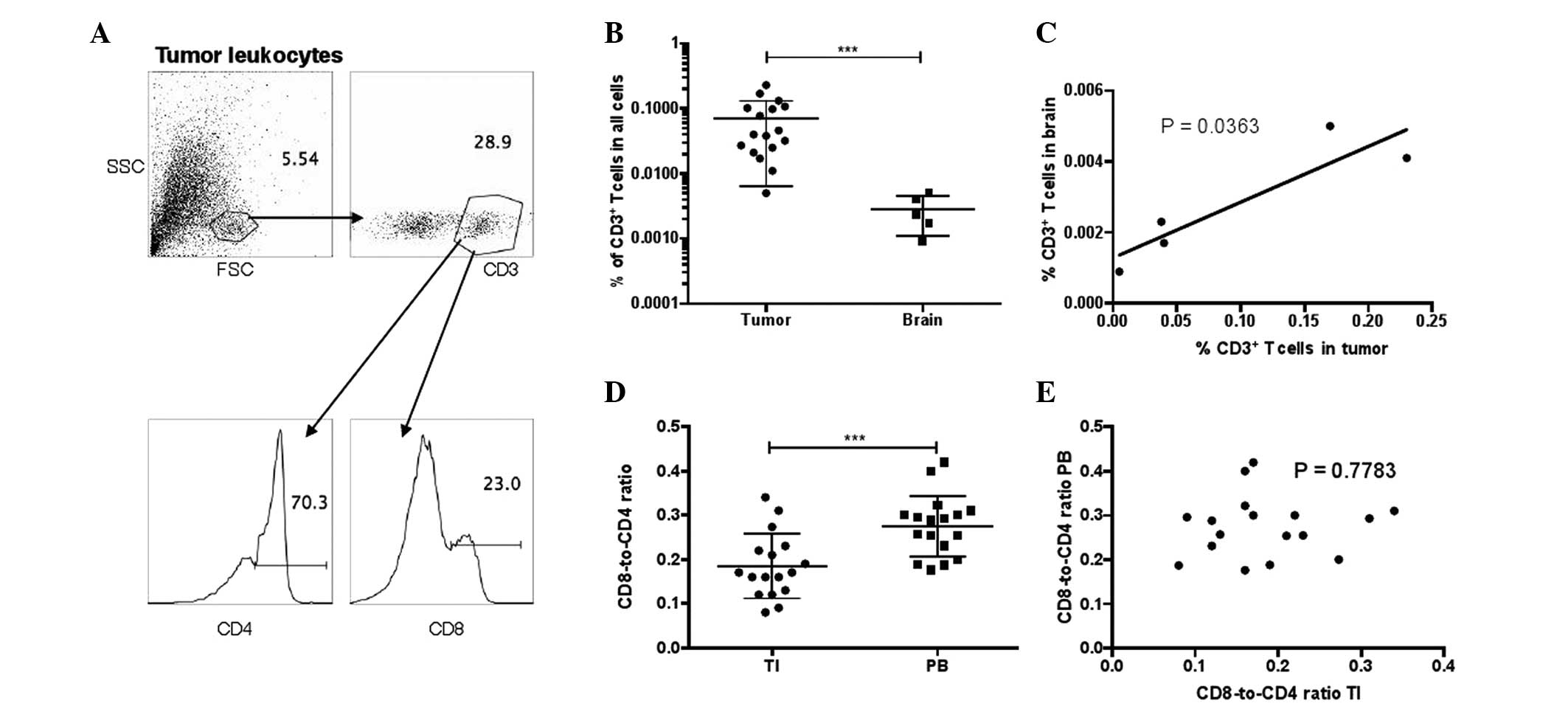
First, the lymphocyte composition was examined in
resected tumors from 17 GBM patients by flow cytometry. Surrounding
normal brain tissues attached to the tumor resection were also
obtained in 5 out of 17 patients. It was found that CD3+
T cells represent a rare population in tumors and normal brain
tissues, accounting for 0.005–0.23% of all tumor cells and
0.0009–0.005% of brain cells (Fig. 1A and
B). In the 5 GBM patients with tumor and brain samples, the
frequencies of tumor-infiltrating CD3+ T cells were
directly correlated with that in the normal brain (Fig. 1C). CD3+ T cells can be
categorized into CD8+ T cells, which are primarily
recognized as cytotoxic T cells and are assessed in various
immunotherapeutic strategies to eliminate cancerous cells, and
CD4+ T cells, which are primarily known as helper T
cells. Notably, within the CD3+ T-cell compartment, the
CD8-to-CD4 ratio was significantly downregulated in the tumors
compared with that in the autologous blood of GBM patients
(Fig. 1D). The CD8-to-CD4 ratios in
the tumor and blood samples of the same patient were not correlated
(Fig. 1E).
Tumor-infiltrating CD3+ T
cells in GBM are highly refractory to proliferation by anti-CD3
stimulation, independent of APC stimulation
Due to the low numbers of T cells observed in the
resected tumors, proliferation responses in tumor T cells and
peripheral blood T cells were then examined by CFSE staining. It
was found that peripheral blood T cells and tumor T cells have
significantly increased proportions of CFSElo cells
following 6 days of stimulation by anti-CD3 monoclonal antibodies
(Fig. 2A and B). Although no
significant background differences were observed between tumor T
cells and peripheral blood T cells when incubated in medium, the
peripheral blood T cells exhibited significantly higher proportions
of CFSElo cells than the tumor T cells following
anti-CD3 stimulation.
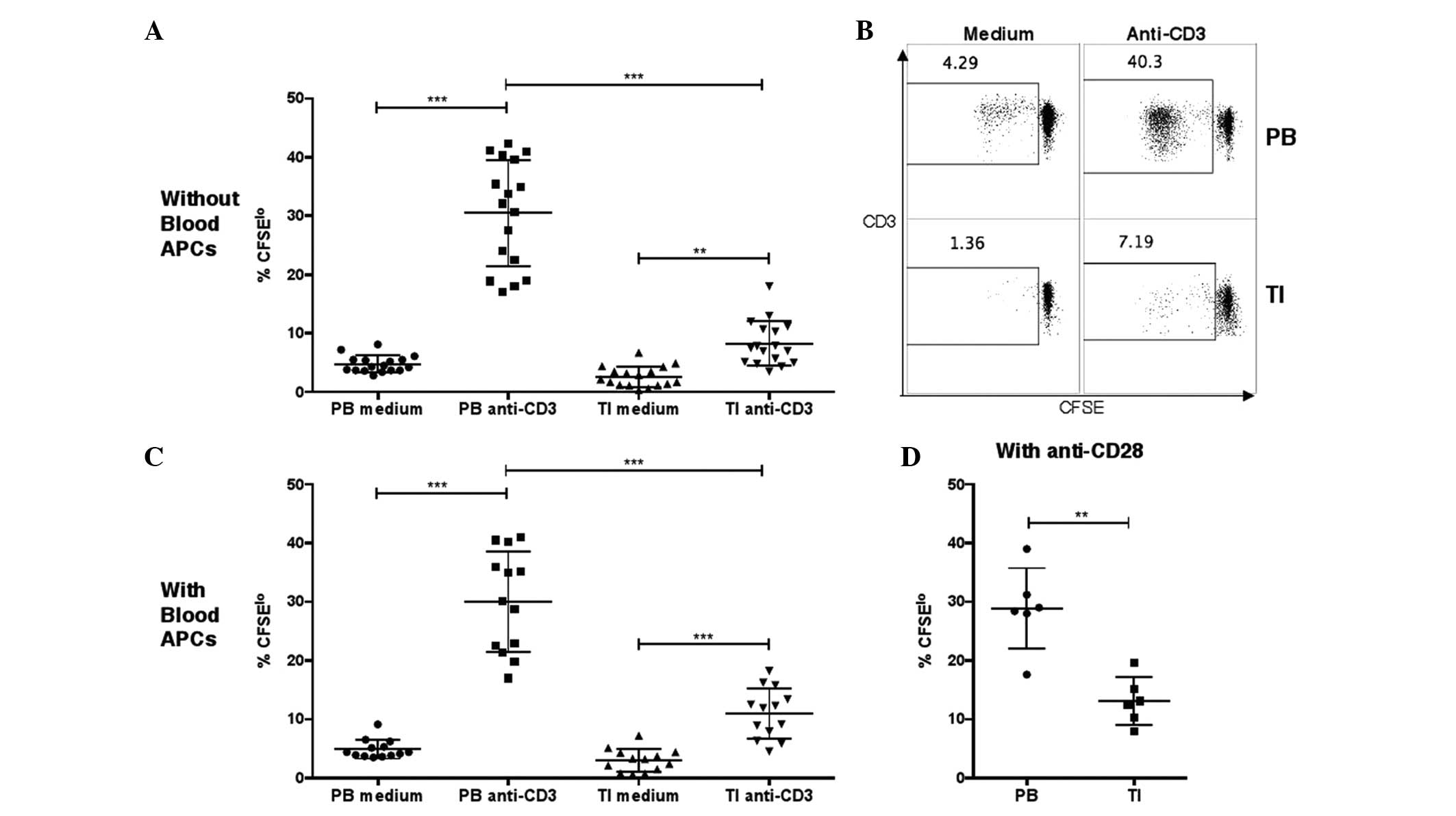 | Figure 2.Proliferation of T cells in PB or TI
cells, as measured by CFSE staining. (A and B) Percentages of
CFSElo cells in PB or TI CD3+ T cells in
unstimulated medium or after stimulation with anti-CD3 antibodies.
PB mononuclear cells or tumor leukocytes were labeled with CFSE and
then incubated in medium without or with 2 µg/ml anti-human CD3
monoclonal antibody at 105 cells per well in a 96-well
plate. The cells were harvested at day 6 and the percentages of
CFSElo cells among the CD3+ cells were
examined by flow cytometry (one-way analysis of variance, followed
by Tukey's multiple comparisons test; ***P<0.001 and
**P<0.01). (C) Percentages of CFSElo cells in PB or
TI T cells in unstimulated medium or after stimulation with
anti-CD3 antibodies, with addition of purified APCs from autologous
PB samples. Purified autologous APCs were added prior to CFSE
labeling (one-way analysis of variance, followed by Tukey's
multiple comparisons test; ***P<0.001). (D) Percentages of
CFSElo cells in PB or TI T cells after stimulation with
anti-CD3 and anti-CD28 monoclonal antibodies. The anti-human CD28
monoclonal antibodies were added together with anti-CD3 antibodies
(unequal variances t-test; **P<0.01). GBM, glioblastoma; CD,
cluster of differentiation; TI, tumor-infiltrating; PB, peripheral
blood; CFSE, carboxyfluorescein succinimidyl ester; APC,
antigen-presenting cell. |
It was hypothesized that the lower proliferation of
tumor-infiltrating T cells in GBM patients may be due to
ineffective stimulation by tumor APCs in the tumor cell culture,
since previously, glioma-infiltrating microglia cells were shown to
be defective at stimulating allogeneic T cells, possibly due to low
expression levels of costimulatory molecules CD80/CD86 and CD40
(19). To test this hypothesis, APCs
were first isolated from 13 peripheral blood samples, and then
autologous APCs were added into tumor leukocyte or PBMC cultures at
1-to-1 APC-to-tumor leukocyte or PBMC ratios. Again, it was found
that the tumor-infiltrating T cells underwent significantly less
proliferation following anti-CD3 stimulation compared with the
autologous peripheral blood T cells in the same patient (Fig. 2C). Furthermore, since CD80/CD86
signaling acts by clustering CD28 molecules expressed on the T-cell
surface, in a separate experiment, anti-CD28 antibodies were added
together with anti-CD3 antibodies during incubation, and it was
found that tumor T cells still underwent less proliferation than
blood T cells from the same patient (Fig.
2D).
In conclusion, a defect in proliferative responses
was observed following anti-CD3 stimulation in tumor-infiltrating T
cells in GBM patients. This defect was independent of APCs and of
stimulation by anti-CD28 antibodies.
Tumor-infiltrating T-cell
proliferation can be rescued by long-term IL-2 stimulation and with
IL-10 neutralization
Next, an attempt was made to rescue
tumor-infiltrating T-cell proliferation in GBM patients. IL-2
provides survival and proliferation signals to activated T cells
through IL-2 receptor signaling (28). Resected tumor leukocytes were obtained
from 6 newly recruited GBM patients and were cultured in medium
supplemented with different concentrations (from 0–20 U/ml) of
recombinant IL-2 for 3 days, after which the cells were stained
with CFSE and stimulated with anti-CD3 antibody for 6 days. It was
found that tumor-infiltrating T-cell proliferation was
significantly higher when the T cells were pre-incubated with 20
U/ml IL-2 compared with 0 U/ml (Fig.
3A). The study also examined the effect of pre-incubation time
in rescuing tumor-infiltrating T-cell responses, and found that the
longest pre-incubation period with 20 U/ml IL-2 (9 days) most
effectively increased the proliferation of the tumor-infiltrating T
cells, although pre-incubation for 3 or 6 days also enhanced
proliferation (Fig. 3B).
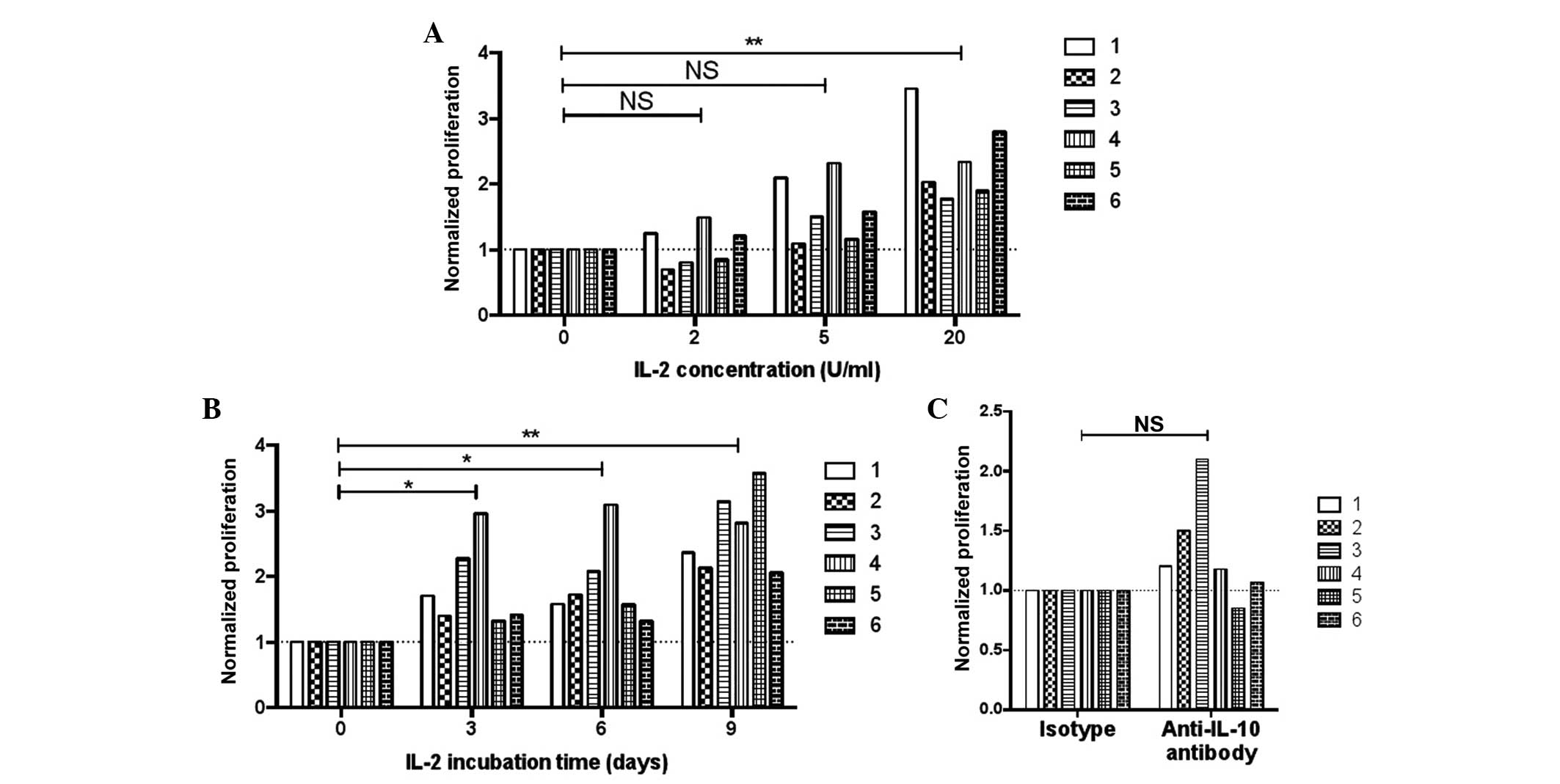 | Figure 3.Proliferation of tumor-infiltrating T
cells in various conditions. Six patients were included and each
bar represents one subject. (A) Effect of pre-incubating with
various concentrations of IL-2 on the proliferation of tumor T
cells. Tumor leukocytes were pre-incubated with 0, 2, 5 or 20 U/ml
IL-2 for 3 days in culture medium, and then the cells were washed,
stained with CFSE, washed again and stimulated with 2 µg/ml
anti-CD3 antibody. After 6 days, the cells were harvested and the
percentages of CFSElo cells in CD3+ cells
were examined by flow cytometry. Data were normalized against the
results with 0 U/ml IL-2 in each patient (repeated measures one-way
analysis of variance, followed by Dunnett's test; **P<0.01). (B)
Effect of the lengths of pre-incubation with IL-2 on the
proliferation of tumor T cells. Tumor leukocytes were pre-incubated
with 20 U/ml IL-2 for 0, 3, 6, or 9 days in culture medium, and
then the cells were stained with CFSE and stimulated with 2 µg/ml
anti-CD3 antibody. The percentages of CFSElo cells were
examined after 6 days. Data were normalized against the results
without IL-2 pre-incubation (0 day) in each patient (repeated
measures one-way analysis of variance, followed by Dunnett's test;
**P<0.01 and *P<0.05). (C) Proliferation of
tumor-infiltrating T cells without or with IL-10 depletion. Tumor
leukocytes were stained with CFSE and stimulated with 2 µg/ml
anti-CD3 antibody for 6 days. Concurrent with the addition of
anti-CD3 antibodies, 2 µg/ml anti-human IL-10 monoclonal antibody
or isotype control antibody were added (paired t-test). NS, not
significant; IL, interleukin; CD, cluster of differentiation; CFSE,
carboxyfluorescein succinimidyl ester. |
Previous studies found that IL-10 production by
tumor-infiltrating microglia cells was elevated in the serum and
microglia cells of glioma patients compared with healthy controls
(29,30). In the present study, in order to
reduce potential inhibition by IL-10, an attempt was made to
sequester the IL-10 in culture by adding anti-IL-10 monoclonal
antibodies. It was found that in 5 out of 6 patients, proliferation
was enhanced with the addition of anti-IL-10 antibodies (Fig. 3C), but this result was not
statistically significant.
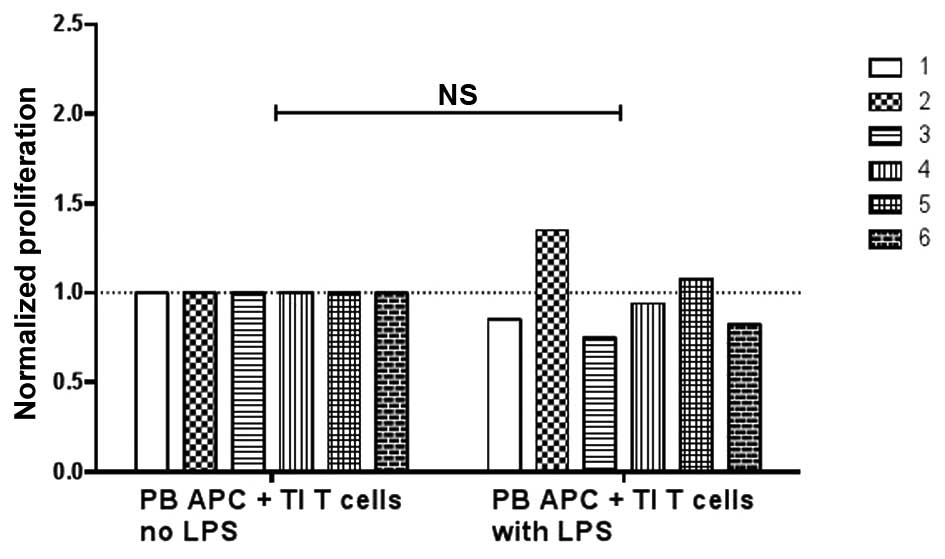
Treatment with LPS does not improve
APC-stimulation of tumor-infiltrating T cells
It has been shown that LPS stimulation of blood
APCs, but not glioma-infiltrating microglia cells, could enhance
the proliferation of allogeneic T cells (19). The present study examined whether the
LPS stimulation of peripheral blood APCs could enhance the
proliferation of autologous tumor-infiltrating T cells under
anti-CD3 stimulation. Unexpectedly, in 4 out of 6 subjects,
pre-treatment with LPS on peripheral blood APCs reduced the
proliferation of the tumor-infiltrating T cells (Fig. 4). It was therefore not found that LPS
could enhance peripheral blood APC-mediated stimulation of
tumor-infiltrating T-cell proliferation.
Discussion
Current treatment of GBM is limited by the
resistance of the tumor to radiation and chemotherapy. Moreover,
surgical removal of the tumor often fails to completely remove
tumor tissues, since tumor cells invade the surrounding normal
brain tissues (6–9). To resolve these difficulties,
therapeutic options using tumor antigen-specific T cells have been
investigated, but their application has been a daunting challenge
due to the existence of the blood-brain barrier and the
immunosuppressive microenvironment inside the tumor. The main goal
of the present study was to examine various options to enhance
tumor-infiltrating T-cell responses in GBM. It was first observed
that the number of tumor-infiltrating T cells was extremely low in
the resected tumor and the surrounding normal brain tissues. Also,
although peripheral blood T cells were previously described as
exhibiting immunosuppression with increased percentages of
regulatory T cells (18), the present
found that the tumor-infiltrating T cells were more suppressed than
their peripheral counterparts in terms of proliferation following
anti-CD3 stimulation. Local activation of infiltrating T cells by
tumor antigens and their subsequent proliferation are considered
beneficial for anti-tumor responses; therefore, the present study
examined a number of strategies to enhance the proliferation by
tumor-infiltrating T cells. It was found that by manipulating IL-2
concentrations and their pre-incubation time in the cell culture,
tumor-infiltrating T-cell proliferation could be effectively
enhanced. Sequestering IL-10 by anti-IL-10 antibodies also improved
tumor-infiltrating T-cell proliferation in 5 out of 6 patients. In
conclusion, the present data showed that although
tumor-infiltrating T cells were more refractory to anti-CD3
stimulation, strategies exist to rescue their responses, such as
the addition of IL-2 and the sequestration of IL-10.
Previous studies have shown that the capacity of
glioma-infiltrating microglia cells to be stimulated by TLRs, to
secrete cytokines and to upregulate costimulatory molecules are
impaired; thus, these cells are less effective at stimulating and
supporting T-cell responses (19).
The present study found that the lower proliferation did not appear
to be solely due to the ineffective stimulation by tumor microglia,
since the addition of blood APCs in the cell culture did not
resolve the difference in the proliferative response between tumor
T cells and autologous blood T cells. A previous study has also
shown that LPS-stimulated peripheral blood APCs can induce
allogeneic T-cell proliferation more effectively than unstimulated
APCs (19). In the present study,
however, it was found that tumor T cells from 4 out of 6 subjects
actually underwent less proliferation when the autologous blood
APCs were stimulated with LPS. This discrepancy may have resulted
from the fact that in the present assay, LPS were added for 3 days
and were washed away prior to the APC T-cell coculture, while in
the previous study (19), LPS were
added concurrently during the coculture, and therefore, direct
stimulation on the allogeneic T cells by LPS cannot be ruled out.
More importantly, since LPS stimulation of APCs was found to
increase IL-10 production under certain conditions (31), we speculate that in GBM patients,
where systemic immune suppression has been observed (12), LPS may have further enhanced the
regulatory phenotype of patient APCs.
Further studies are required to examine the activity
of APCs in GBM patients under various stimulatory conditions and to
assess their efficacy in stimulating autologous T-cell responses
for potential T-cell-mediated immunotherapy.
Acknowledgements
This study was supported by the Natural Science
Foundation of Liaoning Province (grant no. 2013020195).
References
|
1
|
Gladson CL, Prayson RA and Liu WM: The
pathobiology of glioma tumors. Annu Rev Pathol. 5:33–50. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kleihues P, Louis DN, Scheithauer BW,
Rorke LB, Reifenberger G, Burger PC and Cavenee WK: The WHO
classification of tumors of the nervous system. J Neuropathol Exp
Neurol. 61:215–229. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ohgaki H and Kleihues P: Population-based
studies on incidence, survival rates, and genetic alterations in
astrocytic and oligodendroglial gliomas. J Neuropathol Exp Neurol.
64:479–489. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yoshimoto K, Dang J, Zhu S, Nathanson D,
Huang T, Dumont R, Seligson DB, Yong WH, Xiong Z, Rao N, et al:
Development of a real-time RT-PCR assay for detecting EGFRvIII in
glioblastoma samples. Clin Cancer Res. 14:488–493. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mitchell DA, Xie W, Schmittling R, Learn
C, Friedman A, McLendon RE and Sampson JH: Sensitive detection of
human cytomegalovirus in tumors and peripheral blood of patients
diagnosed with glioblastoma. Neuro Oncol. 10:10–18. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Masui K, Cloughesy TF and Mischel PS:
Review: Molecular pathology in adult high-grade gliomas: From
molecular diagnostics to target therapies. Neuropathol Appl
Neurobiol. 38:271–291. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dunn GP, Rinne ML, Wykosky J, Genovese G,
Quayle SN, Dunn IF, Agarwalla PK, Chheda MG, Campos B, Wang A, et
al: Emerging insights into the molecular and cellular basis of
glioblastoma. Genes Dev. 26:756–784. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stupp R, Mason WP, van den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: Radiotherapy plus concomitant and adjuvant temozolomide
for glioblastoma. N Engl J Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Park JK, Hodges T, Arko L, Shen M, Dello
Iacono D, McNabb A, Olsen Bailey N, Kreisl TN, Iwamoto FM, Sul J,
et al: Scale to predict survival after surgery for recurrent
glioblastoma multiforme. J Clin Oncol. 28:3838–3843. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sampson JH, Archer GE, Mitchell DA,
Heimberger AB and Bigner DD: Tumor-specific immunotherapy targeting
the EGFRvIII mutation in patients with malignant glioma. Semin
Immunol. 20:267–275. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sampson JH, Archer GE, Mitchell DA,
Heimberger AB, Herndon JE II, Lally-Goss D, McGehee-Norman S,
Paolino A, Reardon DA, Friedman AH, et al: An epidermal growth
factor receptor variant III-targeted vaccine is safe and
immunogenic in patients with glioblastoma multiforme. Mol Cancer
Ther. 8:2773–2779. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dix AR, Brooks WH, Roszman TL and Morford
LA: Immune defects observed in patients with primary malignant
brain tumors. J Neuroimmunol. 100:216–232. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wilson EH, Weninger W and Hunter CA:
Trafficking of immune cells in the central nervous system. J Clin
Invest. 120:1368–1379. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kuppner MC, Hamou MF, Sawamura Y, Bodmer S
and de Tribolet N: Inhibition of lymphocyte function by
glioblastoma-derived transforming growth factor beta 2. J
Neurosurg. 71:211–217. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bodmer S, Strommer K, Frei K, Siepl C, de
Tribolet N, Heid I and Fontana A: Immunosuppression and
transforming growth factor-beta in glioblastoma. Preferential
production of transforming growth factor-beta 2. J Immunol.
143:3222–3229. 1989.PubMed/NCBI
|
|
16
|
Parsa AT, Waldron JS, Panner A, Crane CA,
Parney IF, Barry JJ, Cachola KE, Murray JC, Tihan T, Jensen MC, et
al: Loss of tumor suppressor PTEN function increases B7-H1
expression and immunoresistance in glioma. Nat Med. 13:84–88. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dong H, Strome SE, Salomao DR, Tamura H,
Hirano F, Flies DB, Roche PC, Lu J, Zhu G, Tamada K, et al:
Tumor-associated B7-H1 promotes T-cell apoptosis: A potential
mechanism of immune evasion. Nat Med. 8:793–800. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fecci PE, Mitchell DA, Whitesides JF, Xie
W, Friedman AH, Archer GE, Herndon JE II, Bigner DD, Dranoff G and
Sampson JH: Increased regulatory T-cell fraction amidst a
diminished CD4 compartment explains cellular immune defects in
patients with malignant glioma. Cancer Res. 66:3294–3302. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hussain SF, Yang D, Suki D, Aldape K,
Grimm E and Heimberger AB: The role of human glioma-infiltrating
microglia/macrophages in mediating antitumor immune responses.
Neuro Oncol. 8:261–279. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhou M, Wiemels JL, Bracci PM, Wrensch MR,
McCoy LS, Rice T, Sison JD, Patoka JS and Wiencke JK: Circulating
levels of the innate and humoral immune regulators CD14 and CD23
are associated with adult glioma. Cancer Res. 70:7534–7542. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schlehofer B, Blettner M, PrestonMartin S,
Niehoff D, Wahrendorf J, Arslan A, Ahlbom A, Choi WN, Giles GG,
Howe GR, et al: Role of medical history in brain tumour
development. Results from the international adult brain tumour
study. Int J Cancer. 82:155–160. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lachance DH, Yang P, Johnson DR, Decker
PA, Kollmeyer TM, McCoy LS, Rice T, Xiao Y, AliOsman F, Wang F, et
al: Associations of high-grade glioma with glioma risk alleles and
histories of allergy and smoking. Am J Epidemiol. 174:574–581.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lohr J, Ratliff T, Huppertz A, Ge Y,
Dictus C, Ahmadi R, Grau S, Hiraoka N, Eckstein V, Ecker RC, et al:
Effector T-cell infiltration positively impacts survival of
glioblastoma patients and is impaired by tumor-derived TGF-β. Clin
Cancer Res. 17:4296–4308. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kmiecik J, Poli A, Brons NH, Waha A, Eide
GE, Enger PØ, Zimmer J and Chekenya M: Elevated CD3+ and
CD8+ tumor-infiltrating immune cells correlate with
prolonged survival in glioblastoma patients despite integrated
immunosuppressive mechanisms in the tumor microenvironment and at
the systemic level. J Neuroimmunol. 264:71–83. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Vauléon E, Tony A, Hamlat A, Etcheverry A,
Chiforeanu DC, Menei P, Mosser J, Quillien V and Aubry M: Immune
genes are associated with human glioblastoma pathology and patient
survival. BMC Med Genomics. 5:412012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pino PA and Cardona AE: Isolation of brain
and spinal cord mononuclear cells using percoll gradients. J Vis
Exp. pii:23482011.
|
|
27
|
Randolph GJ, Jakubzick C and Qu C: Antigen
presentation by monocytes and monocyte-derived cells. Curr Opin
Immunol. 20:52–60. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Malek TR: The biology of interleukin-2.
Annu Rev Immunol. 26:453–479. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Huettner C, Paulus W and Roggendorf W:
Messenger RNA expression of the immunosuppressive cytokine IL-10 in
human gliomas. Am J Pathol. 146:317–322. 1995.PubMed/NCBI
|
|
30
|
Samaras V, Piperi C, Korkolopoulou P,
Zisakis A, Levidou G, Themistocleous MS, Boviatsis EI, Sakas DE,
Lea RW, Kalofoutis A and Patsouris E: Application of the ELISPOT
method for comparative analysis of interleukin (IL)-6 and IL-10
secretion in peripheral blood of patients with astroglial tumors.
Mol Cell Biochem. 304:343–351. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rossol M, Heine H, Meusch U, Quandt D,
Klein C, Sweet MJ and Hauschildt S: LPS-induced cytokine production
in human monocytes and macrophages. Crit Rev Immunol. 31:379–446.
2011. View Article : Google Scholar : PubMed/NCBI
|