Introduction
An aneurysmal bone cyst (ABC) is a benign, locally
destructive lesion of the bone, occurring as a primary bone cyst in
~79% of cases, or as a secondary lesion arising from other osseous
conditions in ~20% of cases (1–3). The peak
age of onset is <20 years, and ~95% of cases have been reported
to occur in the first 3 decades of life (4). ABC accounts for ~1% of all bone tumors
(5,6).
Any bone may be affected by ABC; however, these lesions
predominantly manifest in the metaphysis of long bones (65%), the
pelvis (12%) and the arch of the spine (12%) (7). The differential diagnosis associated
with this lesion includes giant cell tumor (GCT), giant cell
reparative granuloma (GCRG) and Brown tumor arising from
hyperparathyroidism (8–10). Treatment options for patients with ABC
include autogenous bone grafting, cementation or resection of the
lesion (11). The present study
reports a case of ABC localized to the metatarsal, a considerably
rare presentation of which only a few cases have been reported to
date (12).
Case report
A 27-year-old male patient with ABC presented to the
First Affiliated Hospital of Nanchang University (Nanchang, China)
in December 2014 with a history of foot swelling for ~1 year. Other
symptoms included limping and progressively increasing local pain
in his right foot. The patient and his family initially noticed the
swelling following the onset of pain caused by a mild sprain.
Thereafter, the patient reduced his activities in an effort to
alleviate the pain. He had no history of trauma, fever or general
disease.
Physical examination revealed a tender, densely
indurated, immobile mass, which measured ~6 cm in diameter and was
localized to the right forefoot. Standard foot radiographs revealed
an expansive, lytic and proliferative lesion localized to the third
metatarsal (Fig. 1A). Magnetic
resonance imaging (MRI) showed that the tumor exhibited a high
signal intensity on T2-weighted images (Fig. 1B). The patient underwent operation for
wide excision of the lesion, including the whole third toe, and an
autogenous iliac crest bone graft, along with double-plate fixation
affixed to the second and forth toes (Fig. 2). Informed consent was obtained from
the patient for the publication of the data regarding the diagnosis
and treatment.
The gross appearance of the removed tissue was a
soft, dusty-red tissue mass measuring 5.5×5×2.5 cm.
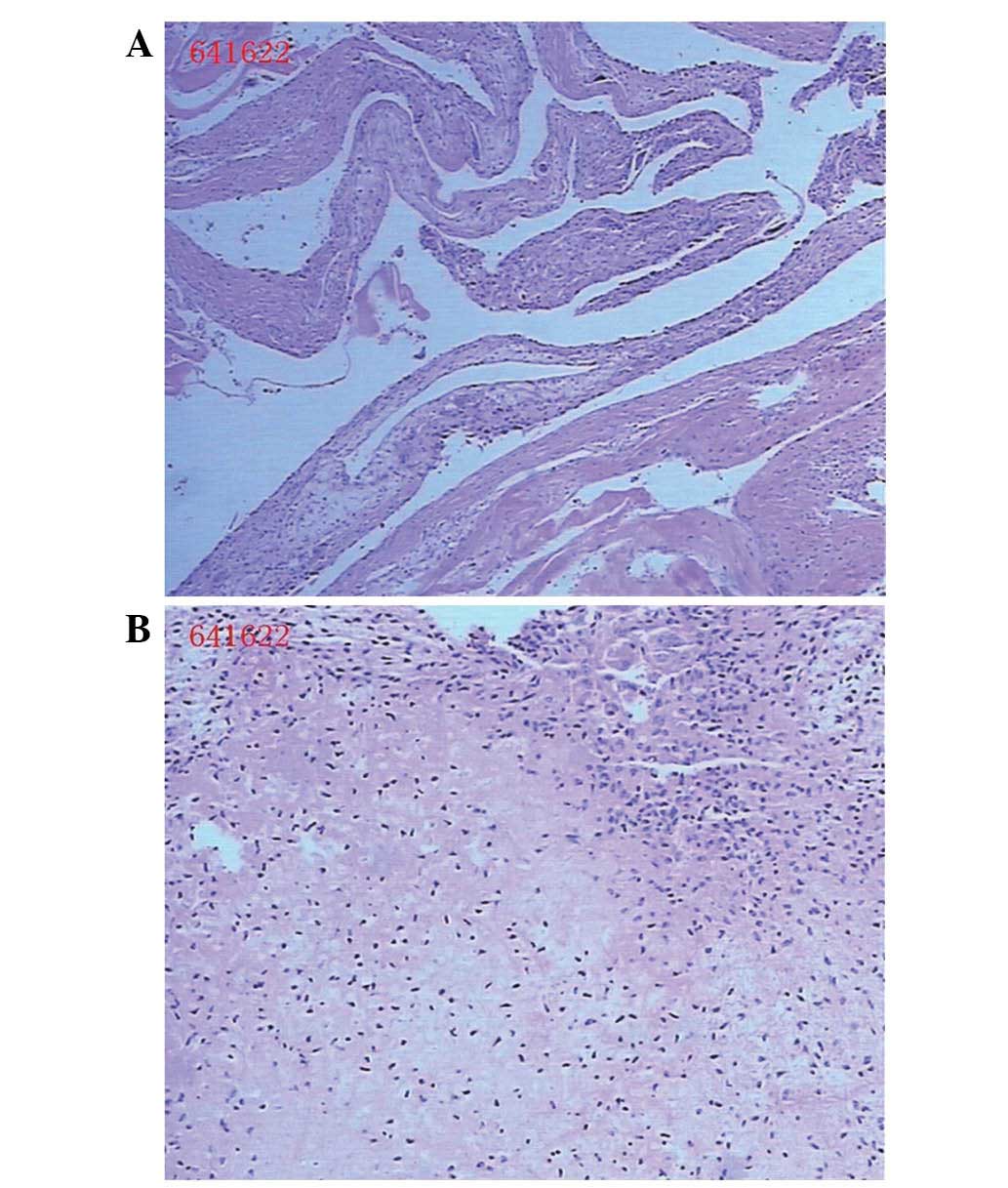
Histopathological examination was subsequently conducted. The
microscopic appearance of the resected tissue was capsule-shaped,
exhibiting large amounts of dilatation and congestion of the
associated small blood vessels, osteoblast proliferation (as
indicated by the blue particles corresponding to osteoprogenitor
cells that were detected by hematoxylin-eosin staining), fibrous
connective tissue and multinucleated giant cell proliferation, with
reactive hyperplasia and trabecular bone tissue (Fig. 3). A final diagnosis of ABC was
established based on the collective clinical information. The
treatment was successful, as no further treatment was required
during subsequent follow-ups and the patient remains healthy at
present.
Discussion
ABCs account for ~1% of all primary bone lesions
that are sampled for biopsy (13).
While the precise pathogenesis of ABC is unclear, the most widely
accepted pathogenic mechanism of ABC involves local circulatory
disturbance, which results in an increase in venous pressure and
the development of enlarged and dilated vascular components within
the affected bone (2). The
differentiation among ABC and other giant cell-containing tumors of
the bone, such as GCT, GCRG and Brown tumor, is crucial (13). GCT is composed of mononuclear and
osteoclast-like multinucleated giant cells, which have the
potential to be locally aggressive (14,15). In
GCT, the tumor is always eccentrically located in the epiphysis and
metaphysis of the bone, and exhibits lytic expansion (16). GCRG is a rare, benign, intraosseous
reactive lesion, histologically characterized by a predominance of
giant and mononuclear cells in areas of hemorrhage (17). Brown tumors have been reported to
occur in 1.5–1.7% of patients with chronic renal deficiency and to
have a considerably more lobulated architectural growth pattern; at
differential diagnosis, hyperparathyroidism can be ruled out on the
basis of serum calcium, parathyroid and phosphorus hormone levels
(18,19). ABC, on the other hand, is known to be
histologically composed of blood-filled cystic spaces separated by
fibrous septae (20).
Computed tomography and MRI scans may be helpful in
the diagnosis of ABC, since T2-weighted MRI could detect a
deformity in the involved metatarsal bone as a segmented,
expansile, multiseptated lesion with a large quantity of fluid
present (21).
Surgical removal is considered the optimal treatment
option for ABC. The lesion is removed by intralesional curettage
through a wide cortical window, and allograft bone grafting may be
used for replacement of bone defects (22). Embolotherapy has also been
successfully used for the treatment of ABCs (23). However, patients must be informed that
ABC has a high recurrence rate (24),
so that any recurrence or malignant transformation can be detected
as early as possible.
In summary, ABC is a destructive, hemorrhagic and
tumor-like lesion occurring predominantly in teenaged patients.
Radiographs and MRI scans can often confirm the diagnosis of ABC;
however, accurate histological evaluation is imperative for
diagnosis. Embolotherapy and replacement of bone defects with a
tricortical autograft are considered safe procedures with minimal
recurrence risk (25). The present
study described a rare case of a ABC in the metatarsal and
highlighted the importance of radiological and histological
examinations for the accuracy of such diagnosis.
References
|
1
|
Jaffe HL and Lichtenstein L: Solitary
unicameral bone cyst with emphasis on the roentgen picture, the
pathologic appearance and the pathogenesis. Arch Surg.
44:1004–11025. 1942. View Article : Google Scholar
|
|
2
|
Cottalorda J and Bourelle S: Modern
concepts of primary aneurismal bone cyst. Arch Orthop Trauma Surg.
127:105–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lichtenstein L: Aneurysmal bone cyst: A
pathological entity commonly mistaken for giant cell tumor and
occasionally for hemangioma and osteogenic sarcoma. Cancer.
3:279–289. 1950. View Article : Google Scholar
|
|
4
|
Singh DK, Singh N and Pant MC: Aneurysmal
bone cyst: An unusual presentation of back pain. Asian J Neurosurg.
9:105–107. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hakim DN, Pelly T, Kulendran M and Caris
JA: Benign tumours of the bone: A review. J Bone Oncol. 4:37–41.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bonakdarpour A, Levy WM and Aegerter E:
Primary and secondary aneurysmal bone cysts: A radiological study
of 75 cases. Radiology. 126:75–83. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Campanacci M, Capanna R and Picci P:
Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res.
204:25–36. 1986.PubMed/NCBI
|
|
8
|
Barnhart MD: Malignant transformation of
an aneurysmal bone cyst in a dog. Vet Surg. 31:519–524. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hsu CS, Hentz VR and Yao J: Tumours of the
hand. Lancet Oncol. 8:157–166. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Saito T, Oda Y, Kawaguchi K, Tanaka K,
Matsuda S, Sakamoto A, Iwamoto Y and Tsuneyoshi M: Five-year
evolution of a telangiectatic osteosarcoma initially managed as an
aneurysmal bone cyst. Skeletal Radiol. 34:290–2941. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ozaki T, Hillmann A, Lindner N and
Winkelmann W: Aneurysmal bone cysts in children. J Cancer Res Clin
Oncol. 122:767–769. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
De Dios AM Vergel, Bond JR, Shives TC,
McLeod RA and Unni KK: Aneurysmal bone cyst. A clinicopathologic
study of 238 cases. Cancer. 69:2921–2931. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Freiberg A, Loder R, Heidelberger K and
Hensinger RN: Aneurysmal bone cysts in young children. J Pediatr
Orthop. 14:86–91. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Foo LF and Raby N: Tumours and tumour-like
lesions in the foot and ankle. Clin Radiol. 60:308–3332. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ratner V and Dorfman HD: Giant-cell
reparative granuloma of the hand and foot bones. Clin Orthop Relat
Res. 260:251–258. 1990.PubMed/NCBI
|
|
16
|
Futamura N, Urakawa H, Tsukushi S, Arai E,
Kozawa E, Ishiguro N and Nishida Y: Giant cell tumor of bone
arising in long bones possibly originates from the metaphyseal
region. Oncol Lett. 11:2629–2634. 2016.PubMed/NCBI
|
|
17
|
Cook DL, Rosenthal DC and Shikoff MD:
Giant cell reparative granuloma of the middle phalanx of the foot:
A review and case report. J Foot Ankle Surg. 47:589–593. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hanna BG, Donthineni R, Majid K, Parekh S,
Shin JS and Lackman RD: Leg mass in a 61-year-old man. Clin Orthop
Relat Res. 406:298–307. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brindley GW, Greene JF Jr and Frankel LS:
Case reports: Malignant transformation of aneurysmal bone cysts.
Clin Orthop Rel Res. 438:282–287. 2005. View Article : Google Scholar
|
|
20
|
Gibbs PC Jr, Hefele MC, Peabody TD, Montag
AG, Aithal V and Simon MA: Aneurysmal bone cyst of the extremities.
Factors related to local recurrence after curettage with a
high-speed burr. J Bone Joint Surg Am. 81:1671–1678.
1999.PubMed/NCBI
|
|
21
|
Iltar S, Alemdaroğlu KB, Karalezli N,
Irgit K, Caydere M and Aydoğan NH: A case of an aneurysmal bone
cyst of a metatarsal: Review of the differential diagnosis and
treatment options. J Foot Ankle Surg. 48:74–79. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Boubbou M, Atarraf K, Chater L, Afifi A
and Tizniti S: Aneurysmal bone cyst primary-about eight pediatric
cases: Radiological aspects and review of the literature. Pan Afr
Med J. 15:1112013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rastogi S, Varshney MK, Trikha V, Khan SA,
Choudhury B and Safaya R: Treatment of aneurysmal bone cysts with
percutaneous sclerotherapy using polidocanol. A review of 72 cases
with long-term follow-up. J Bone Joint Surg Br. 88:1212–1216. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cugati G, Pande A, Jain PK, Symss NP,
Ramamurthi R and Vasudevan CM: Aneurysmal bone cyst of the lumbar
spine. Asian J Neurosurg. 10:216–218. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
deKleuver M, van der Heul RO and Veraart
BE: Aneurysmal bone cyst of the spine: 31 cases and the importance
of the surgical approach. J Pediatr Orthop B. 7:286–292. 1998.
View Article : Google Scholar : PubMed/NCBI
|