Introduction
Prostate cancer (PCa) is the most common cancer
among men in the US (1). Use of the
prostate-specific antigen (PSA) test in PCa screening is
controversial, due to uncertainty surrounding its benefits and
risks (2); the PSA test can identify
asymptomatic, indolent tumors, leading to unnecessary treatments
and significant side effects associated with these treatments
(1,3).
The prevalence of clinically indolent tumors has been estimated to
range from 30 to 70% in men aged >60 years (4,5).
Therefore, a reliable method for distinguishing between indolent
and aggressive PCa is urgently required.
Multiple pre-treatment risk stratification systems
have been developed for patients with PCa (6). Among them, the D'Amico risk
stratification is the most widely used; it groups patients with
localized PCa into three strata (low-, intermediate- and
high-risk), based on total Gleason score, clinical stage and PSA
levels at diagnosis (7). However,
this existing three-group risk stratification system is
insufficient to predict tumor aggressiveness as each risk group,
particularly the intermediate-risk group, remains heterogeneous
with regard to prognosis and treatment management (6). Current research is actively exploring
new markers to enable better distinction between indolent and
aggressive disease and to minimize unnecessary treatment (1).
Testosterone is essential for the normal growth,
cytodifferentiation and maintenance of prostate tissue (8). High testosterone levels were previously
considered to lead to the potential development of PCa and more
rapid growth of the tumor (9,10). However, studies on the association
between testosterone and PCa risk have produced conflicting results
(8,9).
Numerous studies have demonstrated that low, rather than high,
testosterone levels at diagnosis were associated with various
markers of poor prognosis, including an advanced pathological
stage, higher Gleason scores, higher PSA levels, seminal vesicle
invasion and positive surgical margins (11–25). Few
studies have further investigated whether low levels of
testosterone predict poor prognosis.
The present study investigated whether low levels of
total serum testosterone at diagnosis were associated with
aggressive features of PCa. In addition, the study further
investigated whether low levels of testosterone could predict poor
clinical outcomes, including disease progression, mortality from
any cause and PCa-specific mortality, independently of the commonly
used clinical parameters.
Materials and methods
Study population and data
collection
The present study was approved by Institutional
Review Board of the University of Texas MD Anderson Cancer Center
(Houston, TX, USA) and informed consent was obtained from all
individual participants included in the study. Recruitment and data
collection for the present study was conducted as previously
described (26,27). Briefly, a total of 762 non-Hispanic
Caucasian men with previously untreated, newly diagnosed PCa, who
were treated at The University of Texas MD Anderson Cancer Center
between September 2000 and February 2012 and who had total serum
testosterone measured were included in the current study. The
morning total serum testosterone levels were measured as part of a
standard panel of tests evaluating patients' overall baseline
condition prior to treatment. Information on demographics, body
mass index (BMI) and smoking history was collected at patient
registration using self-administered questionnaires. Clinical data,
including diagnosis date, PSA level at diagnosis, biopsy-proven
Gleason score, tumor-node-metastasis classification and treatments,
was abstracted by a chart review of the patients' medical records.
Data regarding disease progression was abstracted for 453 patients
who had a localized tumor and received active treatments. For
patients with locally advanced (T3a, T3b or T4) or metastatic
tumors, follow-up PSA tests were performed every 3–6 months for 5
years. Following definitive therapy, PSA tests were performed every
3–6 months for the first 5 years, every 6–12 months for the
subsequent 5 years, and annually thereafter.
Definition of tumor aggressiveness and
clinical outcomes
Aggressiveness of localized tumors was defined as
follows based on the D'Amico risk criteria (7): Low-risk (total Gleason score ≤6;
clinical tumor classification of T1-T2a; PSA ≤10 ng/ml);
intermediate-risk (Gleason score equal to 7; and/or clinical tumor
classification of T2b; and/or PSA level >10 and ≤20 ng/ml); and
high-risk (Gleason score ≥8; or clinical tumor classification of
T2c-T4; or PSA >20 ng/ml). In addition, metastatic tumors were
defined as the most aggressive form of PCa, as they confer a poor
prognosis (28). Disease progression
in patients with localized tumors was defined as the presence of
biochemical recurrence (BCR), local recurrence or distant
metastasis (whichever was recorded first), as local recurrence or
distant metastasis may occur with no record of an increase in PSA
in certain cases. According to the American Urological Association
Prostate Cancer Guidelines Panel (29), BCR in patients treated with radical
prostatectomy is defined as a PSA ≥0.2 ng/ml with a second
confirmatory level of PSA >0.2 ng/ml. The Radiation Therapy
Oncology Group-American Society for Therapeutic Radiology and
Oncology (30) defines BCR in
patients with PCa who received radiotherapy as a rise in PSA of ≥2
ng/ml above the lowest level following treatment (the nadir).
Statistical analysis
According to an international consensus statement
(31), patients were categorized into
the following three groups based on total serum testosterone
levels: Low (<230 ng/dl), intermediate (230–350 ng/dl) and
normal (>350 ng/dl). The distribution of selected
characteristics of the three testosterone groups were compared
using the nonparametric K-sample test on the equality of medians
for continuous variables and the Chi-squared test for categorical
variables. Odds ratios (ORs) with 95% confidence intervals (CIs)
were calculated to measure the association between serum
testosterone levels and PCa aggressiveness, using multinomial
logistic regression with the low-risk form of PCa as the reference
outcome, following adjustment for potential confounding variables,
including age, BMI and smoking status. In addition, a restricted
cubic spline was used to model the non-linear association between
serum testosterone levels and PCa aggressiveness. Four knots were
used for this model and the 95th percentile (675 ng/dl) was chosen
as the reference level.
The ‘time to event’ of the clinical outcomes was
defined as the length of time between diagnosis and the clinical
outcome of interest (mortality) or the last follow-up. Kaplan-Meier
estimator survival curves and log-rank tests were used to assess
the association between serum testosterone levels and clinical
outcomes across the three testosterone groups. A multivariate Cox
proportional hazards model was used to estimate hazard ratios (HRs)
and 95% CIs, following adjustment for age, tumor aggressiveness
(low-, intermediate- or high-risk, or metastatic) and
treatment.
All statistical analyses were performed using Stata
software (version 13; StataCorp, College Station, TX, USA) and all
tests were two-tailed. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
Specific characteristics of the patients, overall
and by total serum testosterone levels, are summarized in Table I. The majority of the participants had
a total Gleason score of 7, T1 tumor stage, and PSA <10 ng/ml at
diagnosis, and were treated with radiotherapy. Between the three
testosterone groups, patients differed significantly in terms of
BMI at diagnosis, total Gleason score, clinical tumor
classification, lymphatic metastasis at diagnosis, distant
metastasis at diagnosis, clinicopathological characteristics, PSA
levels at diagnosis and initial primary treatment (P<0.001). In
particular, nearly half (47.9%) of the patients with low serum
testosterone had tumors with a total Gleason score of ≥8 compared
with only 11.7% of patients with normal serum testosterone levels.
Distant metastases at diagnosis were present in 19.5% of patients
in the low serum testosterone group compared with 1.8% in the
normal serum testosterone group.
 | Table I.Characteristics of the patients with
prostate cancer in the present study. |
Table I.
Characteristics of the patients with
prostate cancer in the present study.
|
|
| Total serum
testosterone levels |
|
|---|
|
|
|
|
|
|---|
| Characteristic | All groups | Low | Intermediate | Normal | P-value |
|---|
| Total number of
patients | 762 | 316 | 162 | 284 | – |
| Age at diagnosis,
years | 65.0
(31.0–90.0) | 65.0
(43.0–82.0) | 64.0
(43.0–84.0) | 65.0
(31.0–90.0) | 0.32 |
| BMI at
diagnosisa,
kg/m2 | 28.7
(19.8–54.4) | 29.2
(20.9–54.4) | 29.3
(20.9–47.0) | 27.3
(19.8–42.8) | <0.001 |
| Follow-up
timeb, months | 44.4
(0.7–156.8) | 45.3
(0.9–118.9) | 41.5
(0.8–137.3) | 44.2
(0.7–156.8) | 0.53 |
| Smoking status at
diagnosis |
|
|
|
| 0.44 |
|
Non-smoker | 332 (44.0) | 133 (42.1) | 71 (44.7) | 128 (45.7) |
|
| Former
smoker | 364 (48.2) | 158 (50.0) | 80 (50.3) | 126 (45.0) |
|
| Current
smoker | 59 (7.8) | 25 (7.9) | 8 (5.0) | 26 (9.3) |
|
| Total Gleason
score |
|
|
|
| <0.001 |
| ≤6 | 255 (34.0) | 42 (13.7) | 72 (44.4) | 141 (50.0) |
|
| 7 | 295 (39.3) | 118 (38.4) | 69 (42.6) | 108 (38.3) |
|
| ≥8 | 201 (26.8) | 147 (47.9) | 21 (13.0) | 33 (11.7) |
|
| Clinical tumor
classification |
|
|
|
| <0.001 |
| T1 | 415 (54.5) | 109 (34.5) | 107 (66.0) | 199 (70.1) |
|
| T2 | 216 (28.3) | 115 (36.4) | 39 (24.1) | 62 (21.8) |
|
|
T3-T4 | 102 (13.4) | 69 (21.8) | 14 (8.6) | 19 (6.7) |
|
| Tx | 29 (3.8) | 23 (7.3) | 2 (1.2) | 4 (1.4) |
|
| Presence of
lymphatic metastasis at diagnosis |
|
|
|
| <0.001 |
|
Yes | 55 (7.5) | 52 (17.3) | 2 (1.3) | 1 (0.4) |
|
| No | 680 (92.5) | 248 (82.7) | 154 (98.7) | 278 (99.6) |
|
| Presence of distant
metastasis at diagnosis |
|
|
|
| <0.001 |
|
Yes | 70 (9.3) | 61 (19.5) | 4 (2.5) | 5 (1.8) |
|
| No | 683 (90.7) | 252 (80.5) | 155 (97.5) | 276 (98.2) |
|
| PSA at diagnosis,
ng/ml |
|
|
|
| <0.001 |
|
<10 | 585 (77.1) | 207 (65.7) | 139 (85.8) | 239 (84.8) |
|
|
10–20 | 73 (9.6) | 39 (12.4) | 13 (8.0) | 21 (7.4) |
|
|
>20 | 101 (13.3) | 69 (21.9) | 10 (6.2) | 22 (7.8) |
|
| Initial primary
treatment |
|
|
|
| <0.001 |
| Radical
prostatectomy | 152 (20.0) | 57 (18.0) | 43 (26.5) | 52 (18.3) |
|
|
Radiotherapy | 293 (38.5) | 154 (48.7) | 54 (33.3) | 85 (29.9) |
|
| Hormone
therapy | 78 (10.2) | 69 (21.8) | 1 (0.6) | 8 (2.8) |
|
|
Surveillance or
unknownc | 230 (30.2) | 30 (9.5) | 61 (37.7) | 139 (48.9) |
|
| Other
treatmentd | 9 (1.2) | 6 (1.9) | 3 (1.9) | 0 (0) |
|
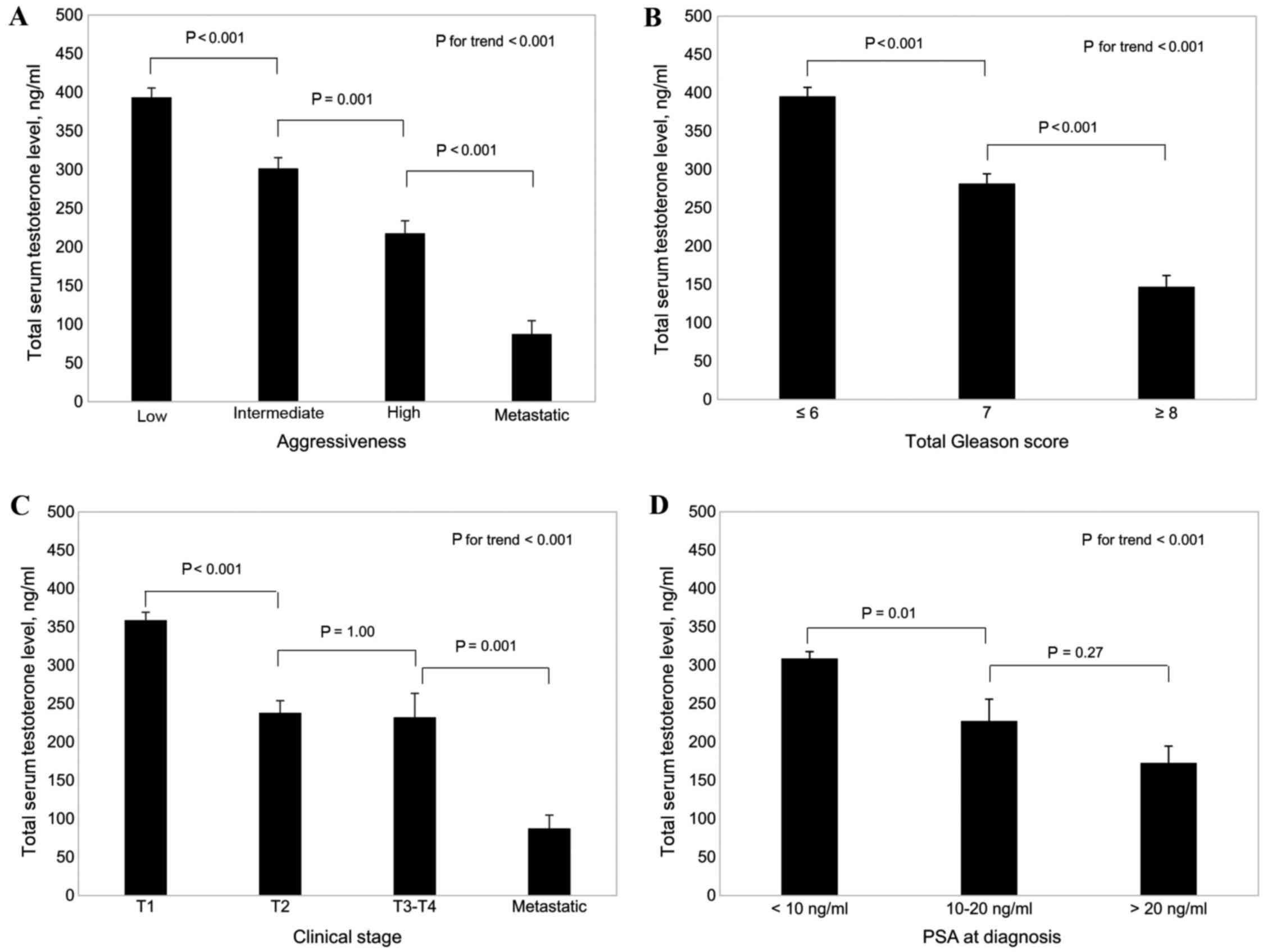
Association between total serum
testosterone levels and PCa aggressiveness
As shown in Fig. 1A,
total serum testosterone levels decreased as aggressiveness
increased (P<0.001). In addition, total serum testosterone
levels decreased with increases in the total Gleason score of the
tumor (P<0.001; Fig. 1B), clinical
tumor stage (P<0.001; Fig. 1C) and
PSA level at diagnosis (P<0.001; Fig.
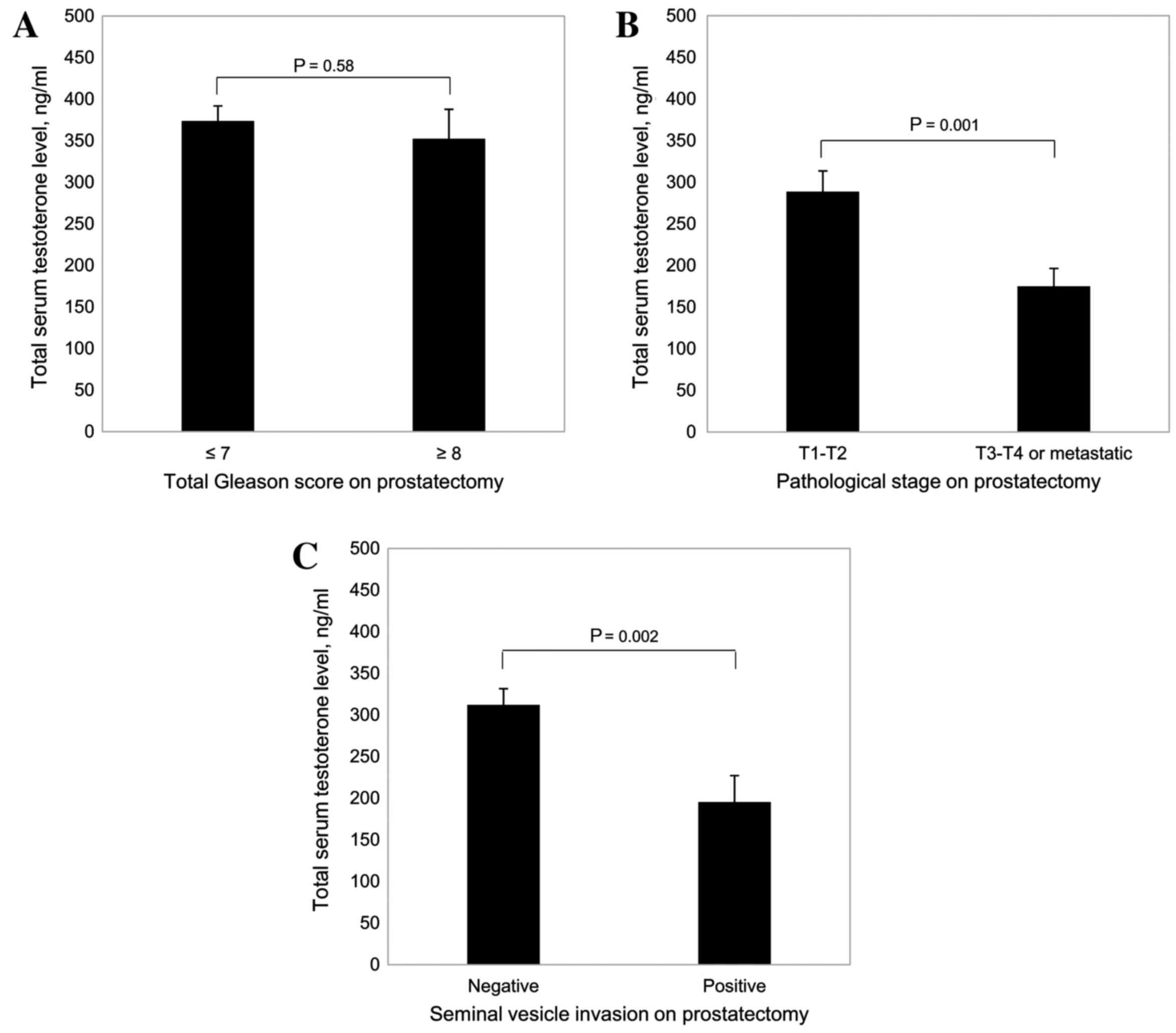
1D). Furthermore, among patients with PCa who underwent radical
prostatectomy (Fig. 2), there were
significantly lower total serum testosterone levels in patients
with advanced pathological stage tumors (T3-T4 or metastatic)
(P=0.001 vs. T1-T2; Fig. 2B) and in
patients with positive seminal vesicle invasion (P=0.002 vs.
negative; Fig. 2C).
Table II shows the
adjusted associations between total serum testosterone levels and
tumor aggressiveness. Patients with low total serum testosterone
levels had statistically significant 2.9-fold (OR, 2.92; 95% CI,
1.74–4.90; P<0.001), 5.6-fold (OR, 5.63; 95% CI, 3.14–10.12;
P<0.001) and 72.4-fold (OR, 72.40; 95% CI, 20.89–250.89;
P<0.001) increased risks of having intermediate-risk, high-risk
and metastatic form of PCa, respectively, compared with patients
with normal total serum testosterone levels. Intermediate levels of
total serum testosterone were not significantly associated with PCa
aggressiveness.
| Table II.Association between total serum
testosterone levels at diagnosis and PCa aggressiveness. |
Table II.
Association between total serum
testosterone levels at diagnosis and PCa aggressiveness.
|
| Testosterone
levels |
|
|---|
|
|
|
|
|---|
| PCa
aggressiveness | Normal | Intermediate | Low | P-value for
trend |
|---|
| Low-risk localized
PCa, number of patients (%) | 128 (54.7) | 67 (28.6) | 39 (16.7) | – |
| Intermediate-risk
localized PCa |
|
|
|
|
| Number
of patients (%) | 101 (40.1) | 58 (23.0) | 93 (36.9) | – |
|
Adjusteda OR (95% CI) | Reference | 1.03
(0.63–1.71) | 2.92
(1.74–4.90)b | <0.001 |
| High-risk localized
PCa |
|
|
|
|
| Number
of patients (%) | 49
(27.2) | 32 (17.8) | 99 (55.0) | – |
|
Adjusteda OR (95% CI) | Reference | 1.23
(0.67–2.28) | 5.63
(3.14–10.12)b | <0.001 |
| Metastatic PCa |
|
|
|
|
| Number
of patients (%) | 6
(6.3) | 5 (5.2) | 85 (88.5) | – |
|
Adjusteda OR (95% CI) | Reference | 2.27
(0.48–10.69) | 72.40
(20.89–250.89)b | <0.001 |
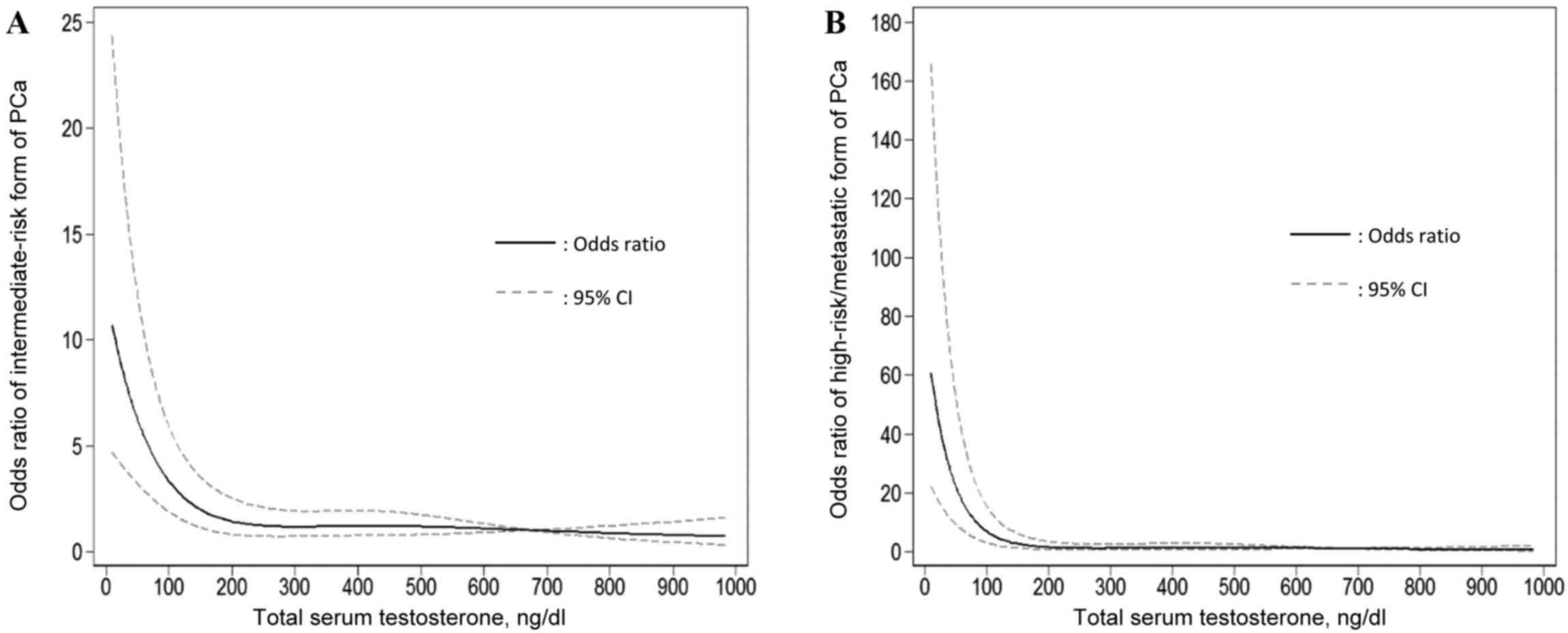
A restricted cubic spline was used to model the
association between total serum testosterone levels and the
intermediate- or high-risk/metastatic forms of PCa (Fig. 3). As shown in Fig. 3A, total serum testosterone levels
>200 ng/dl were not significantly associated with the
intermediate-risk form of PCa; however, total serum testosterone
levels <200 ng/dl were significantly associated with
intermediate-risk form of PCa. A similar association was found
between total serum testosterone levels and high-risk/metastatic
PCa (Fig. 3B); however, when total
serum testosterone levels reached >150 ng/dl an association was
notable.
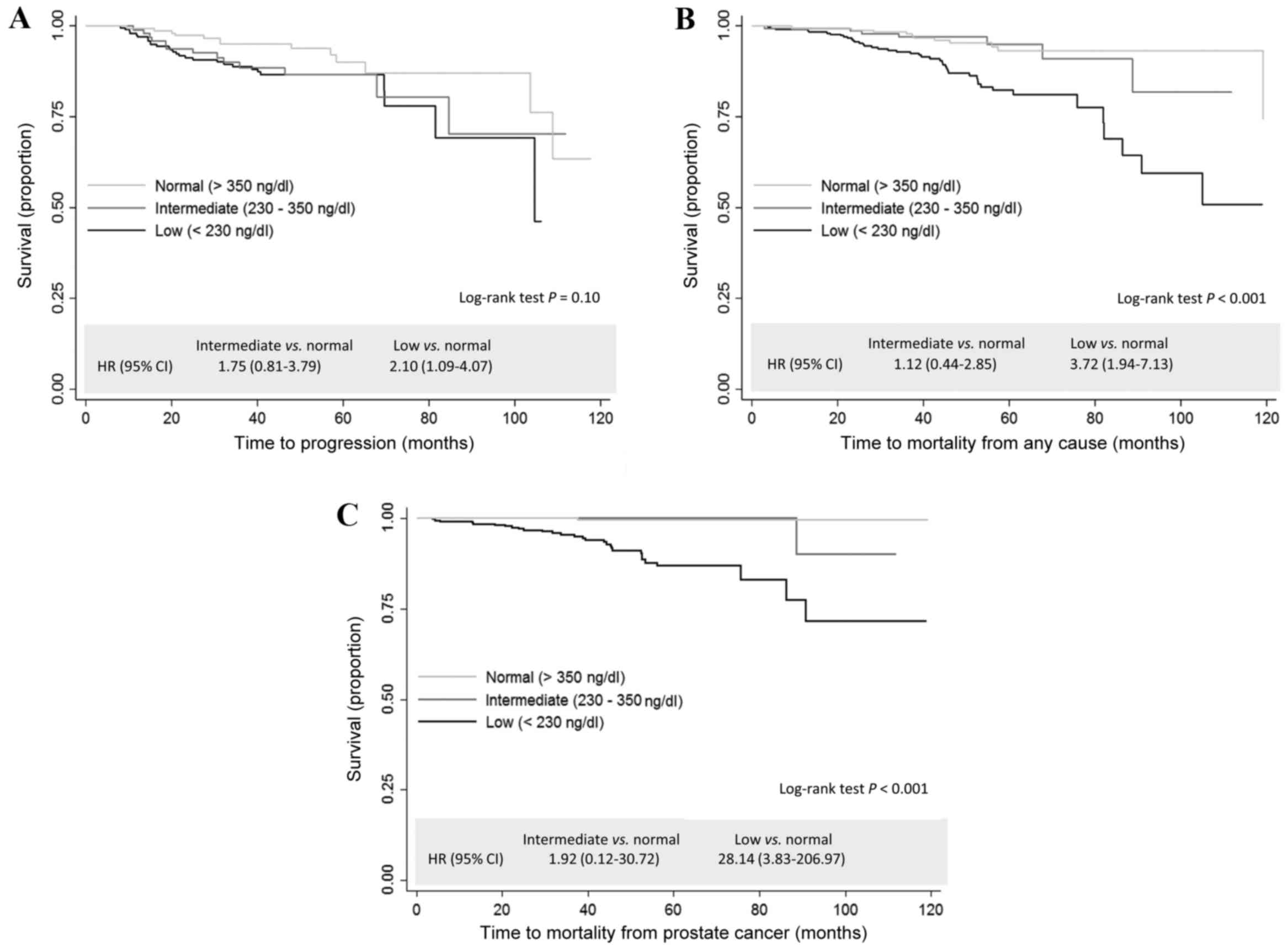
Association between total serum
testosterone levels and clinical outcomes
As shown in Fig. 4,
compared with the group with normal levels of total serum
testosterone, the group with low levels had a significantly
increased risk of disease progression (HR, 2.10; 95% CI, 1.09–4.07;
P=0.03; Fig. 4A), mortality from all
causes (HR, 3.80; 95% CI, 1.99–7.28; P<0.001; Fig. 4B) and mortality due to PCa (HR, 28.14;
95% CI, 3.83–206.97; P<0.001; Fig.
4C). Table III shows the
multivariate adjusted results. Compared with normal testosterone
levels, low levels of testosterone were associated with a
non-significant 1.9-fold (HR, 1.90; 95% CI, 0.89–4.03; P=0.10)
increased risk of mortality from all causes and a significant
10.7-fold (HR, 10.68; 95% CI, 1.35–84.44; P=0.03) increased risk of
death due to PCa.
| Table III.Total serum testosterone levels at
diagnosis and clinical outcomes of PCa patients. |
Table III.
Total serum testosterone levels at
diagnosis and clinical outcomes of PCa patients.
|
| Testosterone
levels |
|
|---|
|
|
|
|
|---|
| Event
occurrence | Normal | Intermediate | Low | P-value for
trend |
|---|
| Disease
progressiona |
|
|
|
|
| Yes, n
(%) | 13 (8.4) | 13
(13.1) | 29
(14.6) | – |
| No, n
(%) | 142 (91.6) | 86
(86.9) | 170 (85.4) | – |
| HR (95%
CI) | Reference | 1.74
(0.79–3.89) | 1.14
(0.51–2.52) | 0.69 |
|
P-value | N/A | 0.17 | 0.75 | – |
| Mortality from any
cause |
|
|
|
|
| Yes, n
(%) | 13 (4.6) | 7
(4.3) | 47
(14.9) | – |
| No, n
(%) | 271 (95.4) | 155 (95.7) | 269 (85.1) | – |
| HR (95%
CI) | Reference | 1.17
(0.45–3.03) | 1.90
(0.89–4.03) | 0.09 |
|
P-value | N/A | 0.75 | 0.1 | – |
| Mortality from
PCa |
|
|
|
|
| Yes, n
(%) | 1
(0.4) | 1
(0.6) | 30 (9.5) | – |
| No, n
(%) | 283 (99.6) | 161 (99.4) | 286 (90.5) | – |
| HR (95%
CI) | Reference | 1.84
(0.11–31.92) | 10.68
(1.35–84.44) | 0.02 |
|
P-value | N/A | 0.81 | 0.03 | – |
Discussion
In a cohort of 762 patients with PCa, the present
study observed that low levels of total serum testosterone at
diagnosis were associated with aggressive features of PCa.
Furthermore, the results of the current study indicate that low
total serum testosterone levels predict poor PCa-specific survival
(i.e., mortality due to PCa). To the best of our knowledge, this is
the first study to show an association between total serum
testosterone levels and PCa-specific mortality.
The present study demonstrated that, compared with
high levels of total serum testosterone at the time of diagnosis,
low total serum testosterone levels at the time of diagnosis were
associated with aggressive features of PCa, which is consistent
with the results of previous studies (11–25). A
previous pooled analysis of 18 prospective studies identified that
pre-diagnosis serum testosterone levels were not associated with
the high-risk form of PCa (32);
however, the testosterone levels in this analysis were measured
years prior to PCa diagnosis and a different definition of
high-risk form of PCa was used.
The results of the current study suggest that low
total serum testosterone levels predict poor prognosis in patients
with PCa. Three previous studies (33–35), of
which two had small sample sizes (34,35), have
investigated this association in patients with metastatic PCa
patients. Consistent with the present study, the results of these
studies indicated that lower testosterone levels predicted poor
overall (33,34) and progression-free (35) survival times in patients with
metastatic PCa. Two previous studies investigated the association
between testosterone levels and BCR in patients with PCa who
received radical prostatectomy, with inconsistent results; one
study (36) indicated that lower
testosterone levels predicted BCR, while the other study (24) showed no association between these
factors (24). In addition, low
testosterone has been demonstrated to be an independent risk factor
for disease progression/reclassification in patients with PCa on
active surveillance (37).
The molecular mechanisms underlying the association
demonstrated in the present study between low total serum
testosterone levels at diagnosis and PCa aggressiveness or poor
prognosis is unclear. One possibility is that low total serum
testosterone levels may induce or select for molecular features
that are indicative of more aggressive PCa or drug resistance
(38). A previous study using
NKX3-1/PTEN mutant mice suggested that prolonged exposure to low
testosterone levels led to accelerated PCa progression and elevated
expression of well-characterized markers of cancer progression,
such as extracellular signal-regulated kinase/mitogen-activated
protein kinase (39). Further gene
expression profiling suggested that NKX3-1/PTEN mutant PCa mice
with low testosterone levels and NKX3-1/PTEN mutant mice with
androgen-independent PCa shared markedly similar gene expression
profiles (39). The overlapping
cluster included genes such as androgen receptor (AR),
matrix metalloproteinase 9, ETS1, runt-related transcription factor
1 and Vav guanine nucleotide exchange factor 3, which are
associated with human PCa progression and hormone-refractory PCa
(39). Previous human studies
identified that patients with metastatic PCa with low serum
testosterone levels had a worse response to endocrine therapy
compared with patients with high serum testosterone levels
(33,38). Notably, data from the present study is
consistent with the general model of oncogene derepression as a
mechanism of PCa progression (40).
In this model, inhibition of AR function can lead to derepression
of oncogenes that are normally repressed by the fully functional
AR, leading to PCa progression. It is conceivable that low serum
testosterone may lead to activation of oncogenic pathways through
this general mechanism.
The results of the present study have important
clinical implications for the management and treatment of patients
with PCa. The results indicate that pre-treatment total serum
testosterone levels could serve as a marker to distinguish between
indolent and aggressive PCa. Notably, total serum testosterone
levels could predict prognosis beyond the existing D'Amico
three-group risk stratification (7)
based on total Gleason score, clinical stage and PSA. If the
findings of the current study are replicated and validated,
clinicians may consider testing total serum testosterone routinely
at diagnosis, in order to minimize over-treatment of indolent PCa
and under-treatment of aggressive PCa.
The present study had several limitations. Firstly,
despite the relatively large sample size, there was little data for
clinical outcome due to the fact that the majority of the patients
had localized disease. The association between total serum
testosterone levels and PCa-specific survival was statistically
significant despite the small number of events; however, there was
insufficient statistical power for the other two clinical outcomes
(disease progression and mortality from all causes). Secondly, the
study group consisted of a heterogeneous population, including
patients with localized and metastatic tumors. The strengths of the
current study were the systematic assessment of a large group of
patients with PCa for a series of clinical outcomes, including
disease progression, mortality from all causes and PCa-specific
mortality, which provided a comprehensive assessment of the
association between total serum testosterone levels and PCa
prognosis. In addition, all serum testosterone assays,
histopathological diagnoses, treatment procedures and collection of
covariates were performed in a standard and consistent way across
all patients. In future, studies with a larger sample size and
measurements of bioavailable/free serum testosterone and other
androgens, such dihydrotestosterone and androstenedione, are
warranted.
In conclusion, the results of the present study
using a large cohort support the mounting evidence of an
association between low total serum testosterone levels at
diagnosis and PCa aggressiveness. In addition, the results indicate
that low total serum testosterone levels predict poor prognosis.
Further observational studies are warranted to validate these
results in a larger and more diverse population.
Acknowledgements
The present study was supported by the National
Cancer Institute (National Institutes of Health, Bethesda, MA, USA;
grant no. CA140388), the Cancer Prevention and Research Institute
of Texas (Austin, TX, USA; grant no. RP140556) and the Center for
Translational and Public Health Genomics (University of Texas MD
Anderson Cancer Center, Houston, TX, USA).
Glossary
Abbreviations
Abbreviations:
|
PCa
|
prostate cancer
|
|
PSA
|
prostate-specific antigen
|
|
BMI
|
body mass index
|
|
OR
|
odds ratio
|
|
CI
|
confidence interval
|
|
HR
|
hazard ratio
|
|
BCR
|
biochemical recurrence
|
References
|
1
|
American Cancer Society, . Cancer Facts
& Figures 2015. American Cancer Society; Atlanta, GA: 2015
|
|
2
|
Barry MJ: Screening for prostate
cancer-the controversy that refuses to die. N Engl J Med.
360:1351–1354. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Welch HG and Albertsen PC: Prostate cancer
diagnosis and treatment after the introduction of prostate-specific
antigen screening: 1986–2005. J Natl Cancer Inst. 101:1325–1329.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zlotta AR, Egawa S, Pushkar D, Govorov A,
Kimura T, Kido M, Takahashi H, Kuk C, Kovylina M, Aldaoud N, et al:
Prevalence of prostate cancer on autopsy: Cross-sectional study on
unscreened Caucasian and Asian men. J Natl Cancer Inst.
105:1050–1058. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Welch HG and Black WC: Overdiagnosis in
cancer. J Natl Cancer Inst. 102:605–613. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rodrigues G, Warde P, Pickles T, Crook J,
Brundage M, Souhami L and Lukka H: Genitourinary Radiation
Oncologists of Canada: Pre-treatment risk stratification of
prostate cancer patients: A critical review. Can Urol Assoc J.
6:121–127. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
D'Amico AV, Whittington R, Malkowicz SB,
Schultz D, Blank K, Broderick GA, Tomaszewski JE, Renshaw AA,
Kaplan I, Beard CJ and Wein A: Biochemical outcome after radical
prostatectomy, external beam radiation therapy, or interstitial
radiation therapy for clinically localized prostate cancer. JAMA.
280:969–974. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Isbarn H, Pinthus JH, Marks LS, Montorsi
F, Morales A, Morgentaler A and Schulman C: Testosterone and
prostate cancer: Revisiting old paradigms. Eur Urol. 56:48–56.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Klap J, Schmid M and Loughlin KR: The
relationship between total testosterone levels and prostate cancer:
A review of the continuing controversy. J Urol. 193:403–413. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Morgentaler A: Testosterone and prostate
cancer: An historical perspective on a modern myth. Eur Urol.
50:935–939. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
García-Cruz E, Piqueras M, Huguet J, Peri
L, Izquierdo L, Musquera M, Franco A, Alvarez-Vijande R, Ribal MJ
and Alcaraz A: Low testosterone levels are related to poor
prognosis factors in men with prostate cancer prior to treatment.
BJU Int. 110:E541–E546. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Morgentaler A: Turning conventional wisdom
upside-down: Low serum testosterone and high-risk prostate cancer.
Cancer. 117:3885–3888. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Imamoto T, Suzuki H, Fukasawa S, Shimbo M,
Inahara M, Komiya A, Ueda T, Shiraishi T and Ichikawa T:
Pretreatment serum testosterone level as a predictive factor of
pathological stage in localized prostate cancer patients treated
with radical prostatectomy. Eur Urol. 47:308–312. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schatzl G, Madersbacher S, Thurridl T,
Waldmüller J, Kramer G, Haitel A and Marberger M: High-grade
prostate cancer is associated with low serum testosterone levels.
Prostate. 47:52–58. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yano M, Imamoto T, Suzuki H, Fukasawa S,
Kojima S, Komiya A, Naya Y and Ichikawa T: The clinical potential
of pretreatment serum testosterone level to improve the efficiency
of prostate cancer screening. Eur Urol. 51:375–380. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Massengill JC, Sun L, Moul JW, Wu H,
McLeod DG, Amling C, Lance R, Foley J, Sexton W, Kusuda L, et al:
Pretreatment total testosterone level predicts pathological stage
in patients with localized prostate cancer treated with radical
prostatectomy. J Urol. 169:1670–1675. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Isom-Batz G, Bianco FJ Jr, Kattan MW,
Mulhall JP, Lilja H and Eastham JA: Testosterone as a predictor of
pathological stage in clinically localized prostate cancer. J Urol.
173:1935–1937. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Teloken C, Da Ros CT, Caraver F, Weber FA,
Cavalheiro AP and Graziottin TM: Low serum testosterone levels are
associated with positive surgical margins in radical retropubic
prostatectomy: Hypogonadism represents bad prognosis in prostate
cancer. J Urol. 174:2178–2180. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
San Francisco IF, Regan MM, Dewolf WC and
Olumi AF: Low age adjusted free testosterone levels correlate with
poorly differentiated prostate cancer. J Urol. 175:1341–1346. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Leon P, Seisen T, Cussenot O, Drouin SJ,
Cattarino S, Compérat E, Renard-Penna R, Mozer P, Bitker MO and
Rouprêt M: Low circulating free and bioavailable testosterone
levels as predictors of high-grade tumors in patients undergoing
radical prostatectomy for localized prostate cancer. Urol Oncol.
33:384.r21-e27. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Salonia A, Gallina A, Briganti A, Abdollah
F, Suardi N, Capitanio U, Colombo R, Freschi M, Rigatti P and
Montorsi F: Preoperative hypogonadism is not an independent
predictor of high-risk disease in patients undergoing radical
prostatectomy. Cancer. 117:3953–3962. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ide H, Yasuda M, Nishio K, Saito K,
Isotani S, Kamiyama Y, Muto S and Horie S: Development of a
nomogram for predicting high-grade prostate cancer on biopsy: The
significance of serum testosterone levels. Anticancer Res.
28:2487–2492. 2008.PubMed/NCBI
|
|
23
|
Dai B, Qu Y, Kong Y, Ye D, Yao X, Zhang S,
Wang C, Zhang H and Yang W: Low pretreatment serum total
testosterone is associated with a high incidence of Gleason score
8–10 disease in prostatectomy specimens: Data from ethnic Chinese
patients with localized prostate cancer. BJU Int. 110:E667–E672.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lane BR, Stephenson AJ, Magi-Galluzzi C,
Lakin MM and Klein EA: Low testosterone and risk of biochemical
recurrence and poorly differentiated prostate cancer at radical
prostatectomy. Urology. 72:1240–1245. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Botto H, Neuzillet Y, Lebret T, Camparo P,
Molinie V and Raynaud JP: High incidence of predominant Gleason
pattern 4 localized prostate cancer is associated with low serum
testosterone. J Urol. 186:1400–1405. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
He Y, Gu J, Strom S, Logothetis CJ, Kim J
and Wu X: The prostate cancer susceptibility variant rs2735839 near
KLK3 gene is associated with aggressive prostate cancer and can
stratify gleason score 7 patients. Clin Cancer Res. 20:5133–5139.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tu H, Gu J, Meng QH, Kim J, Davis JW, He
Y, Wagar EA, Thompson TC, Logothetis CJ and Wu X: Mitochondrial DNA
copy number in peripheral blood leukocytes and the aggressiveness
of localized prostate cancer. Oncotarget. 6:41988–41996.
2015.PubMed/NCBI
|
|
28
|
Howlader N, Noone AM, Krapcho M, Garshell
J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,
et al: SEER Cancer Statistics, Review 1975–2011. http://seer.cancer.gov/csr/1975_2013/Accessed.
September 12–2016.
|
|
29
|
Cookson MS, Aus G, Burnett AL,
Canby-Hagino ED, D'Amico AV, Dmochowski RR, Eton DT, Forman JD,
Goldenberg SL, Hernandez J, et al: Variation in the definition of
biochemical recurrence in patients treated for localized prostate
cancer: The American Urological Association Prostate Guidelines for
Localized Prostate Cancer Update Panel report and recommendations
for a standard in the reporting of surgical outcomes. J Urol.
177:540–545. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Roach M III, Hanks G, Thames H Jr,
Schellhammer P, Shipley WU, Sokol GH and Sandler H: Defining
biochemical failure following radiotherapy with or without hormonal
therapy in men with clinically localized prostate cancer:
Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int
J Radiat Oncol Biol Phys. 65:965–974. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang C, Nieschlag E, Swerdloff R, Behre
HM, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B,
Morales A, et al: Investigation, treatment, and monitoring of
late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA and ASA
recommendations. J Androl. 30:1–9. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Endogenous Hormones and Prostate Cancer
Collaborative Group, ; Roddam AW, Allen NE, Appleby P and Key TJ:
Endogenous sex hormones and prostate cancer: A collaborative
analysis of 18 prospective studies. J Natl Cancer Inst.
100:170–183. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ryan CJ, Molina A, Li J, Kheoh T, Small
EJ, Haqq CM, Grant RP, de Bono JS and Scher H: Serum androgens as
prognostic biomarkers in castration-resistant prostate cancer:
Results from an analysis of a randomized phase III trial. J Clin
Oncol. 31:2791–2798. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ribeiro M, Ruff P and Falkson G: Low serum
testosterone and a younger age predict for a poor outcome in
metastatic prostate cancer. Am J Clin Oncol. 20:605–608. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Imamoto T, Suzuki H, Akakura K, Komiya A,
Nakamachi H, Ichikawa T, Igarashi T and Ito H: Pretreatment serum
level of testosterone as a prognostic factor in Japanese men with
hormonally treated stage D2 prostate cancer. Endocr J. 48:573–578.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yamamoto S, Yonese J, Kawakami S, Ohkubo
Y, Tatokoro M, Komai Y, Takeshita H, Ishikawa Y and Fukui I:
Preoperative serum testosterone level as an independent predictor
of treatment failure following radical prostatectomy. Eur Urol.
52:696–701. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
San Francisco IF, Rojas PA, DeWolf WC and
Morgentaler A: Low free testosterone levels predict disease
reclassification in men with prostate cancer undergoing active
surveillance. BJU Int. 114:229–235. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Furuya Y, Nozaki T, Nagakawa O and Fuse H:
Low serum testosterone level predicts worse response to endocrine
therapy in Japanese patients with metastatic prostate cancer.
Endocr J. 49:85–90. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Banach-Petrosky W, Jessen WJ, Ouyang X,
Gao H, Rao J, Quinn J, Aronow BJ and Abate-Shen C: Prolonged
exposure to reduced levels of androgen accelerates prostate cancer
progression in Nkx3.1; Pten mutant mice. Cancer Res. 67:9089–9096.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Karantanos T, Evans CP, Tombal B, Thompson
TC, Montironi R and Isaacs WB: Understanding the mechanisms of
androgen deprivation resistance in prostate cancer at the molecular
level. Eur Urol. 67:470–479. 2015. View Article : Google Scholar : PubMed/NCBI
|