Introduction
Lung cancer is a major cause of mortality in
developed countries (1). Surgical
resection is the prominent curative treatment option for this type
of disease, particularly during the early stages of non-small cell
lung cancer (NSCLC) (1). However, the
5-year survival rate for patients with NSCLC who undergo surgery
remains ~70% (1,2). Several biomarkers have been reported as
predictors of survival and recurrence in patients with NSCLC,
including tumor-infiltrating regulatory T cells (Tregs) (3). A number of previous studies have
demonstrated that the immune microenvironment of the primary tumor
is a significant prognostic factor. Immunological biomarkers in the
tumor microenvironment are useful prognostic predictors, in
addition to promising targets for novel therapeutic approaches
(4–9).
In particular, a promising immunological biomarker may be Tregs;
the potential mechanism underlying the induction of Tregs is the
expression of cyclooxygenase-2 (Cox-2) in tumor cells (10). These findings may facilitate the
development of individualized immunomodulatory therapies to deplete
the tumor microenvironment from Tregs.
A major limitation to individualized
immunomodulatory therapies is the requirement for adequate tumor
specimens, which frequently necessitates an invasive procedure
(11). Furthermore, in patients with
recurrent disease, further tissue specimens are required; however,
rebiopsies are difficult to perform in certain cases, including
those with brain metastasis (11).
Urinary prostaglandin E2 (PGE2) metabolite
(PGE-M) is a major urinary metabolite of PGE2 and may be
used as an index of systemic PGE2 production (11). Cox-2-derived PGE2 serves
important roles in cancer progression. PGE2 is an
unstable compound that is rapidly metabolized to stable PGE-M in
vivo by the enzyme 15-hydroxyprostaglandin dehydrogenase
(12). Furthermore, the direct
quantification of PGE2 levels has been revealed to be an
unreliable indicator of a biomarker of inflammation caused by
infection or malignancy (12);
therefore, several previous studies have used measurements of
urinary PGE-M instead (13,14).
In the present study, urinary PGE2 levels
were directly quantified using a highly sensitive PGE2
ELISA kit, to investigate whether urinary PGE2 levels
were associated with the expression of Cox-2 protein or levels of
Tregs in patients with NSCLC.
Patients and methods
Study population
Urinary and paraffin-embedded tumor samples were
obtained from 21 consecutive patients with NCSLC who underwent
surgical resection at Kawasaki Medical School Hospital (Kurashiki,
Japan) between September 2014 and March 2015. None of the patients
had received radiotherapy or chemotherapy prior to surgery. This
prospective study was conducted with the approval of the
Institutional Ethics Committee of Kawasaki Medical School, and
informed consent for the use of urine and tumor specimens was
obtained from all patients. The histological diagnosis of the
tumors was based on the criteria of the World Health Organization,
and the tumor-node-metastasis (TNM) stage was determined according
to the criteria established in 2009 (15). Fluorodeoxyglucose
(18FDG)-positron emission tomography-computed tomography
scanning was used to calculate the maximal standardized uptake
value (SUVmax). Scanning was performed 60 min following intravenous
injection of 150–220 MBq of 18FDG. The regions of
interest were placed three-dimensionally over the lung cancer
nodules.
Patients were excluded from enrollment if they were
taking, or had a history of regularly taking, aspirin or other
nonsteroidal anti-inflammatory drugs (NSAID). Patients were also
ineligible if they had concurrent severe or uncontrolled medical
diseases, including active systemic infection, diabetes or renal
failure.
Measurement of urinary PGE2
and PGE-M via ELISA
The urine samples were obtained prior to surgery and
stored at −20°C following centrifugation at 500 × g for 5 min at
room temperature. The urinary PGE2 level was determined
using a Correlate-EIA™ PGE2 Enzyme
Immunoassay kit (Assay Designs; Enzo Life Sciences, Inc.,
Farmingdale, NY, USA) according to the manufacturer's instructions.
Plates were read at an absorbance wavelength of 450 nm (Varioskan®
Flash Spectral Scanning Multimode Reader; Thermo Scientific, Inc.,
Waltham, MA, USA). The urinary PGE2 level was calculated
in pg/ml, according to the protocol provided by the manufacturer of
the assay kit. In addition, measurement of urinary PGE-M levels
were performed at SRL, Inc. (Tokyo, Japan), and expressed in
pg/ml.
Immunohistochemical (IHC)
analysis
IHC analyses were performed using resected,
paraffin-embedded lung cancer tissues. Following microtome
sectioning, the tissue slides (4-µm-thick) were stained for Cox-2
and forkhead box P3 (Foxp3), a marker of Tregs, using an automated
immunostainer (NexES Special Stainer; Ventana Medical Systems,
Inc., Tucson, AZ, USA) according to the manufacturer's
instructions. Slides were de-paraffinized using EZprep solution
(Ventana Medical Systems, Inc.) for 30 min at 75°C. Epitope
retrieval was accomplished on the automated stainer with cell
conditioning 1 solution (Ventana Medical Systems, Inc.) for 60 min
at 95°C. The antibodies were transferred with diluent to
user-fillable dispensers for use on the automated stainer. Slides
were developed using the Optiview DAB IHC detection kit (Ventana
Medical Systems, Inc.). Briefly, the slides were treated with the
inhibitor included was for 4 min, the multimer for 12 min,
DAB/peroxide for 8 min and copper solution for 4 min at 37°C.
Slides were subsequently counterstained with hematoxylin II
(Ventana Medical Systems, Inc.) for 4 min at 37°C.
Primary antibodies directed against Cox-2 (dilution,
1:50; catalog no., CX-294; Dako; Agilent Technologies, Inc., Santa
Clara, CA, USA) and Foxp3 (dilution, 1:100; catalog no., 22510;
Abcam, Cambridge, UK) were used at 37°C according to the
manufacturer's protocol. Secondary antibody (Discovery Universal
Secondary Antibody, Ventana Medical Systems, Inc.; catalog no.,
760-4205) was used at 37°C according to the manufacturer's
protocol. The expression levels of each marker protein were
examined and evaluated according to a previously reported original
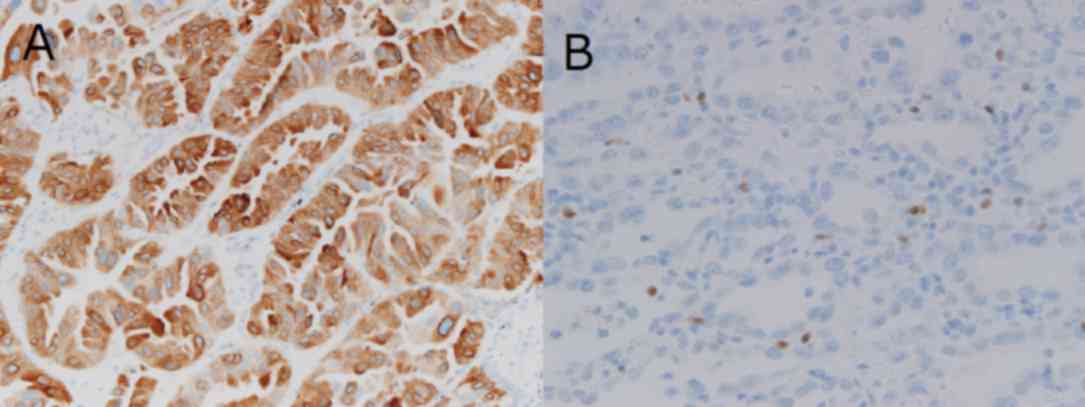
protocol (16,17). For Cox-2, the slides were scored
according to the intensity of staining (0–3) and the percentage of
positively stained cells (0, 0%; 1, 1–9%; 2, 10–49%; and 3,
50–100%). The IHC score (0–9) was calculated as the product of
multiplying the intensity and percentage scores. Cox-2 expression
was considered positive when the IHC score was ≥4 (16). To evaluate the immunostaining of the
Tregs, digital high-power field (HPF) images of the tumor area were
taken using a light microscope (Axiophot microscope; Carl Zeiss AG,
Oberkochen, Germany), of which 10 were selected and the absolute
number of Foxp3+ lymphocytes in these images determined
(17). The number of immunostained
Foxp3 cells was then determined as the mean count from the images
and used to obtain the tumor-infiltrating Foxp3+ Treg
count (Treg score; 0–24). IHC staining demonstrated high levels of
Cox-2 expression (Fig. 1A) and
Foxp3+ Tregs (Fig.
1B).
Statistical analysis
All statistical analyses were performed using SPSS
software (version 17.0; SPSS, Inc., Chicago, IL, USA). The
χ2 test and Fisher's exact test were used to examine the
association between urinary PGE2 or PGE-M levels and
various clinicopathological parameters of the patients. P<0.05
was considered to indicate a statistically significant
difference.
Results
Patient clinicopathological
characteristics
Clinicopathological characteristics of the patients
are summarized in Table I. The
patients ranged in age from 40–83 years old (mean, 69.1 years), and
included 8 males and 13 females. Adenocarcinoma was detected in 18
patients (85.7%) and squamous cell carcinoma was observed in 3
patients (14.3%). Pathological lymph node N0 disease was detected
in 17 patients (80.9%), and N1 or N2 disease in 4 patients (19.1%).
Pathological stage I disease was observed in 15 patients (71.5%),
and stage II or stage IIIA disease was detected in 6 patients
(28.5%).
 | Table I.Clinicopathological characteristics of
the patients (n=21). |
Table I.
Clinicopathological characteristics of
the patients (n=21).
| Clinicopathological
characteristic | No. of patients
(%) |
|---|
| Age |
|
<70 | 11 (52.4) |
|
≥70 | 10 (47.6) |
|
Sex |
|
|
Male | 8
(38.0) |
|
Female | 13 (62.0) |
| Tumor
histology |
|
Adenocarcinoma | 18 (85.7) |
|
Squamous cell carcinoma | 3
(14.3) |
| Tumor stage |
| T1 | 11 (52.2) |
| T2 | 9
(43.0) |
| T3 | 1 (4.8) |
| Pathological lymph
node status |
| N0 | 17 (80.9) |
| N1 | 1 (4.8) |
| N2 | 3
(14.3) |
| Pathological tumor
stage |
| IA | 10 (47.7) |
| IB | 5 (9.5) |
| II
(A+B) | 2
(23.8) |
|
IIIA | 4
(19.0) |
| Surgical procedure
undergone |
|
Lobectomy | 20 (95.2) |
| Wedge
resection | 1 (4.8) |
Association between
clinicopathological characteristics and urinary
PGE2/PGE-M levels
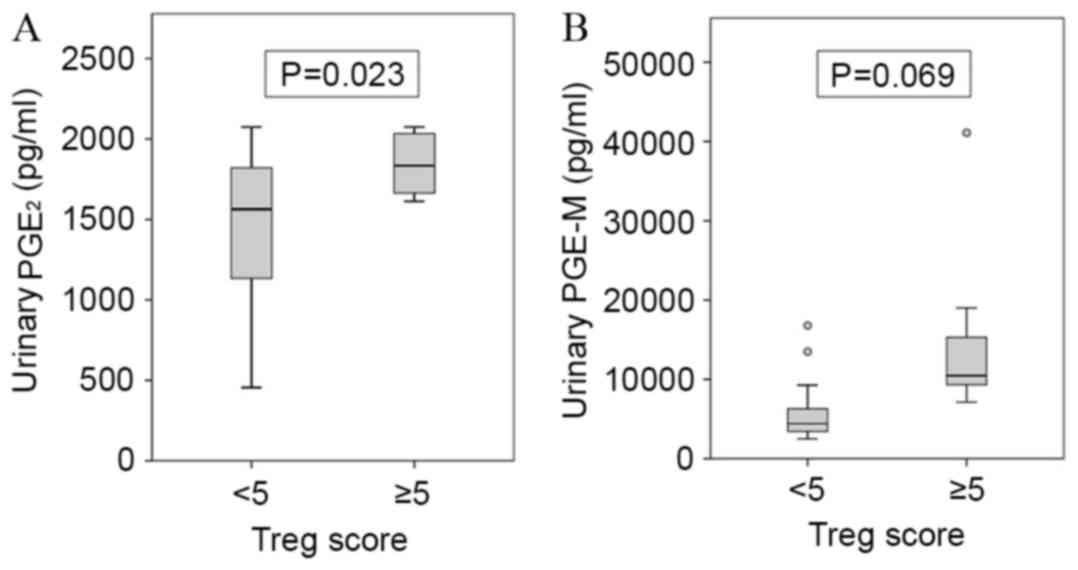
No significant correlation was observed between the
urinary PGE2 and PGE-M levels (r=0.372; P=0.097; data
not shown). However, urinary PGE2 levels (P=0.023), but
not the urinary PGE-M levels (P=0.069), were significantly
positively correlated with Treg score (Fig. 2 and Table
II). The mean value of the urinary PGE2 level was
1467±478 pg/ml in the group with a Treg score <5 (n=13) and
1844±204 pg/ml in the group with a Treg score ≥5 (n=8) (Table II). No significant association was
observed between the urinary PGE2 levels and the Cox-2
IHC score (P=0.986; Table II). In
addition, no significant associations were identified between
urinary PGE2 and any of the other clinicopathological
characteristics examined, including age (P=0.863), sex (P=0.265),
smoking history (P=0.465), histology (P=0.094), tumor size
(P=0.524), nodal status (P=0.395), disease stage (P=0.680) and the
SUVmax (P=0.308) (Table II).
| Table II.Association of urinary
PGE2 and PGE-M levels with the clinicopathological
characteristics of patients with non-small cell lung cancer. |
Table II.
Association of urinary
PGE2 and PGE-M levels with the clinicopathological
characteristics of patients with non-small cell lung cancer.
| Clinicopathological
characteristic | No. of
patients | Urinary
PGE2 (pg/ml) | P-value | Urinary PGE-M
(pg/ml) | P-value |
|---|
| Age |
|
| 0.863 |
| 0.177 |
|
<70 | 11 | 1,594±384 |
| 6,818±3,225 |
|
|
≥70 | 10 | 1,629±501 |
| 12,349±11,651 |
|
| Sex |
|
| 0.265 |
| 0.423 |
|
Female | 13 | 1,529±451 |
| 8,400±10,278 |
|
|
Male | 8 | 1,744±392 |
| 11,161±5,076 |
|
| Smoking
history |
|
| 0.465 |
| 0.785 |
| Never
smoked | 14 | 1,561±450 |
| 9,157±10,274 |
|
|
Smoker | 7 | 1,709±409 |
| 10,041±4,285 |
|
| Histology |
|
| 0.094 |
| 0.854 |
|
Adenocarcinoma | 18 | 1,581± 77 |
| 9,334±9,095 |
|
|
Squamous cell carcinoma | 3 | 1,788±392 |
| 10,160±6,247 |
|
| Tumor size |
|
| 0.524 |
| 0.741 |
| T1 | 11 | 1,672±295 |
| 10,052±10,920 |
|
|
T2-3 | 10 | 1,543±557 |
| 8,792±5,628 |
|
| Pathological nodal
status |
|
| 0.395 |
| 0.271 |
| N0 | 17 | 1,679±335 |
| 10,329±9,132 |
|
|
N1+2 | 4 | 1,321±715 |
| 5,725±5,260 |
|
| Pathological
stage |
|
| 0.680 |
| 0.332 |
| I | 15 | 1,645±342 |
| 10,354±9,757 |
|
|
II+IIIA | 6 | 1,525±640 |
| 7,197±4,701 |
|
| SUVmax |
|
| 0.308 |
| 0.693 |
|
<5 | 10 | 1,506±458 |
| 8,607±1,1652 |
|
| ≥5 | 11 | 1,705±406 |
| 10,220±5,004 |
|
| Cox-2 score |
|
| 0.986 |
| 0.657 |
|
<4 | 14 | 1,609±416 |
| 9,924±10,312 |
|
| ≥4 | 7 | 1,613±499 |
| 8,509±3,963 |
|
| Treg score |
|
| 0.023 |
| 0.069 |
|
<5 | 13 | 1,467±478 |
| 6,162±4,468 |
|
| ≥5 | 8 | 1,844±204 |
| 14,799±11,192 |
|
The mean urinary PGE-M level was 6,162±4,468 pg/ml
in the group with a Treg score <5 (n=13), and 14,799±11,192
pg/ml in the group with a Treg score ≥5 (n=8) (Table II). No significant association was
observed between the urinary PGE-M levels and the Cox-2 IHC scores
(P=0.657) or any of the other clinicopathological characteristics
examined (Table II).
Discussion
In 2010, it was demonstrated that the
tumor-infiltrating Foxp3+ Treg count (Treg score) was
positively correlated with intratumoral Cox-2 expression, and was
also associated with recurrence-free survival, particularly in
patients with lymph node-negative NSCLC (10). In the present study, the association
of urinary PGE2 levels with the Cox-2 IHC score and Treg
score were examined in 21 consecutive patients with NSCLC who
underwent surgical tumor resection at Kawasaki Medical School
Hospital. The results revealed a significant association between
the urinary PGE2 levels and Treg score. In addition, to
the best of our knowledge, the current study was the first to use
the urinary PGE2 level, and not the PGE-M level, for the
assessment of prognosis in patients with NSCLC.
Tregs were initially characterized as possessing a
CD4+CD25+ phenotype and are considered to
modulate the antitumor immune response (18). Tregs are able to suppress the activity
of cytotoxic T cells through direct cell-to-cell contact or via the
release of cytokines (19). The most
specific Treg cell marker currently identified is the nuclear
transcription factor Foxp3 (19,20). A
high density of tumor-infiltrating Foxp3+ Tregs has been
reported to be associated with a higher risk of recurrence and a
poorer overall survival in patients with NSCLC (21). Sharma et al (22) demonstrated that tumor-derived
Cox-2/PGE2 induces the expression of Foxp3 and increases
Treg activity in lung cancer.
Cox-2-derived PGE2 has been demonstrated
to be important in cancer progression (23). Previous studies have suggested that
the majority of PGE2 formed in vivo is derived
from Cox-2 (24,25). Urinary PGE-M levels in healthy
patients or patients with lung cancer are suppressed significantly
by nonselective Cox inhibitors, including aspirin, and by
Cox-2-selective inhibitors (25). As
the antitumor effects of NSAIDs depend on the inhibition of Cox-2
and subsequent reduction in the quantity of PGE2
produced, urinary PGE-M levels may serve as a valuable intermediate
marker of the pharmacological activity of NSAIDs. A previous phase
II clinical trial revealed that patients with NSCLC exhibiting
complete and partial responses to adjuvant therapy with
carboplatin, paclitaxel and celecoxib had significantly decreased
urinary PGE-M levels (26). In
another phase II clinical trial of combined treatment with
celecoxib and docetaxel, patients with recurrent NSCLC with the
greatest proportional decline in urinary PGE-M levels exhibited a
longer survival time, compared with patients with no change or an
increase in urinary PGE-M levels (27). These findings indicate that urinary
PGE-M is a potential biomarker for predicting the efficacy of Cox-2
inhibitors in adjuvant therapies.
Depleting Tregs via targeting C-C motif chemokine
receptor 4 (CCR4) may be a potential cancer immunotherapy, as CCR4
is highly expressed on the surface of type 2 helper T cells and
Tregs (28). Mogamulizumab, a
humanized anti-CCR4 monoclonal antibody, has been demonstrated to
reduce the numbers of CCR4+ malignant T cells and Tregs
in cutaneous T-cell lymphoma (28).
However, to the best of our knowledge, no previous studies have
examined whether urinary PGE2 may serve as a potential
biomarker for predicting the efficacy of Treg-targeting
therapy.
There were several limitations of the current study.
Firstly, the sample size was small compared with previous studies.
Secondly, urinary PGE2 levels were directly quantified
in the current study, whilst previous studies have evaluated the
urinary PGE-M levels in patients with cancer (11–14). To
the best of our knowledge, this is the first study to utilize the
direct quantification of urinary PGE2 levels. The direct
quantification of PGE2 levels has been revealed to be an
unreliable indicator, however, the optimal method for the
assessment and use of this marker remains to be established
(12).
In the current study, urinary PGE2 levels
were not associated with tumor Cox-2 expression levels. Numerous
single nucleotide polymorphisms (SNPs) in the Cox-2 gene have been
identified, which may contribute to divergent Cox-2 expression
levels and PGE2 activities in patients with cancer
(29). Compared with patients with
esophageal tumors harboring the Cox-2-1195G, carriers of the
Cox2-1195AA variant exhibit significantly increased Cox-2
expression levels (29). In 2012 it
was reported that Cox-2 SNPs contributed significantly to increased
tumor infiltration by Tregs (30).
The results from a previous study revealed that the AA genotype
group exhibited a significantly higher Treg score compared with the
GA/GG group, independent of the intratumoral Cox-2 expression
levels (30). The results of the
present study revealed that urinary PGE2 levels were
positively correlated with tumor Treg expression, but not Cox-2
expression. This may be attributable to SNPs in the Cox-2 gene.
In conclusion, that present study demonstrated that
urinary PGE2 levels were positively correlated with
intratumoral Treg count in patients with NSCLC. In addition,
urinary PGE2 levels may be an improved biomarker,
relative to PGE-M, for the prediction of intratumoral Treg
expression. Additional studies in larger patient populations are
required to evaluate the efficacy of urinary PGE2 as a
biomarker in this regard.
Acknowledgements
The authors would like to thank Mrs. Kiyomi Maitani
(Department of General Thoracic Surgery, Kawasaki Medical School,
Okayama, Japan) for providing technical assistance. This work was
supported in part by a research project grant from Kawasaki Medical
School (grant no. 26-64).
References
|
1
|
Asamura H, Goya T, Koshiishi Y, Sohara Y,
Eguchi K, Mori M, Nakanishi Y, Tsuchiya R, Shimokata K, Inoue H, et
al: A Japanese lung cancer registry study: Prognosis of 13,010
resected lung cancers. J Thorac Oncol. 3:46–52. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sawabata N, Miyaoka E, Asamura H,
Nakanishi Y, Eguchi K, Mori M, Nomori H, Fujii Y, Okumura M and
Yokoi K: Japanese Joint Committee for Lung Cancer Registration:
Japanese lung cancer registry study of 11,663 surgical cases in
2004: Demographic and prognosis changes over decade. J Thorac
Oncol. 6:1229–1235. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shimizu K, Okita R and Nakata M: Clinical
significance of the tumor microenvironment in non-small cell lung
cancer. Ann Transl Med. 1:202013.PubMed/NCBI
|
|
4
|
Dieu-Nosjean MC, Antoine M, Danel C,
Heudes D, Wislez M, Poulot V, Rabbe N, Laurans L, Tartour E, de
Chaisemartin L, et al: Long-term survival for patients with
non-small-cell lung cancer with intratumoral lymphoid structures. J
Clin Oncol. 26:4410–4417. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Al-Shibli K, Al-Saad S, Donnem T, Persson
M, Bremnes RM and Busund LT: The prognostic value of
intraepithelial and stromal innate immune system cells in non-small
cell lung carcinoma. Histopathology. 55:301–312. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dai F, Liu L, Che G, Yu N, Pu Q, Zhang S,
Ma J, Ma L and You Z: The number and microlocalization of
tumor-associated immune cells are associated with patient's
survival time in non-small cell lung cancer. BMC Cancer.
10:2202010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takanami I, Takeuchi K and Naruke M: Mast
cell density is associated with angiogenesis and poor prognosis in
pulmonary adenocarcinoma. Cancer. 88:2686–2692. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Al-Shibli KI, Donnem T, Al-Saad S, Persson
M, Bremnes RM and Busund LT: Prognostic effect of epithelial and
stromal lymphocyte infiltration in non-small cell lung cancer. Clin
Cancer Res. 14:5220–5227. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wakabayashi O, Yamazaki K, Oizumi S,
Hommura F, Kinoshita I, Ogura S, Dosaka-Akita H and Nishimura M:
CD4+ T cells in cancer stroma, not CD8+ T cells in cancer cell
nests, are associated with favorable prognosis in human non-small
cell lung cancers. Cancer Sci. 94:1003–1009. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shimizu K, Nakata M, Hirami Y, Yukawa K,
Maeda A and Tanemoto K: Tumor-infiltrating Foxp3+ regulatory T
cells are correlated with cyclooxygenese-2 expression and are
associated with recurrence in resected non-small cell lung cancer.
J Thorac Oncol. 5:585–590. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ferretti A, Flanagan VP and Roman JM:
Quantitative analysis of 11
alpha-hydroxy-9,15-dioxo-2,3,4,5,20-pentanor-19-carboxyprostanoic
acid, the major urinary metabolite of E prostaglandins in man. Anal
Biochem. 128:351–358. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang D and DuBois RN: Urinary PGE-M: A
promising cancer biomarker. Cancer Prev Res (Phila). 6:507–510.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cai Q, Gao YT, Chow WH, Shu XO, Yang G, Ji
BT, Wen W, Rothman N, Li HL, Morrow JD and Zheng W: Prospective
study of urinary prostaglandin E2 metabolite and colorectal cancer
risk. J Clin Oncol. 24:5010–5016. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dong LM, Shu XO, Gao YT, Milne G, Ji BT,
Yang G, Li HL, Rothman N, Zheng W, Chow WH and Abnet CC: Urinary
prostaglandin E2 metabolite and gastric cancer risk in the Shanghai
women's health study. Cancer Epidemiol Biomarkers Prev.
18:3075–3078. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Goldstraw P, Crowley J, Chansky K, Giroux
DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V and Sobin L:
International Association for the Study of Lung Cancer
International Staging Committee; Participating Institutions: The
IASLC lung cancer staging project: Proposals for the revision of
the TNM stage groupings in the forthcoming (seventh) edition of the
TNM Classification of malignant tumours. J Thorac Oncol. 2:706–714.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Edelman MJ, Watson D, Wang X, Morrison C,
Kratzke RA, Jewell S, Hodgson L, Mauer AM, Gajra A, Masters GA, et
al: Eicosanoid modulation in advanced lung cancer: Cyclooxygenase-2
expression is a positive predictive factor for celecoxib+
chemotherapy -cancer and leukemia group B trial 30203. J Clin
Oncol. 26:848–855. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Perrone G, Ruffini PA, Catalano V, Spino
C, Santini D, Muretto P, Spoto C, Zingaretti C, Sisti V,
Alessandroni P, et al: Intratimoural FOXP3-positive regulatory T
cells are associated with adverse prognosis in radically resected
gastric cancer. Eur J Cancer. 44:1875–1882. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Curiel TJ: Tregs and rethinking cancer
immunotherapy. J Clin Invest. 117:1167–1174. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim JM and Rudensky A: The role of the
transcription factor Foxp3 in the development of regulatory T
cells. Immunol Rev. 212:86–98. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hori S, Nomura T and Sakaguchi S: Control
of regulatory T cell development by the transcription factor Foxp3.
Science. 299:1057–1061. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Petersen RP, Campa MJ, Sperlazza J, Conlon
D, Joshi MB, Harpole DH Jr and Patz EF Jr: Tumor infiltrating
Foxp3+ regulatory T-cells are associated with reccurence in
pathologic stage l NSCLC patients. Cancer. 107:2866–2872. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sharma S, Yang SC, Zhu L, Reckamp K,
Gardner B, Baratelli F, Huang M, Batra RK and Dubinett SM: Tumor
cyclooxygenase-2/prostaglandin E2-dependent promotion of FOXP3
expression and CD4+CD25+ T regulatory cell activities in lung
cancer. Cancer Res. 65:5211–5220. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang D and Dubois RN: Eicosanoids and
cancer. Nat Rev Cancer. 10:181–193. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Morris PG, Zhou XK, Milne GL, Goldstein D,
Hawks LC, Dang CT, Modi S, Fornier MN, Hudis CA and Dannenberg AJ:
Increased levels of urinary PGE-M, a biomarker of inflammation,
occur in association with obesity, aging and lung metastases in
patients with breast cancer. Cancer Prev Res (Philla). 6:428–436.
2013. View Article : Google Scholar
|
|
25
|
Murphey LJ, Williams MK, Sanchez SC, Byrne
LM, Csiki I, Oates JA, Johnson DH and Morrow JD: Quantification of
the major urinary metabolite of PGE2 by a liquid
chromatographic/mass spectrometric assay: Determination of
cyclooxygenase-specific PGE2 synthesis in healthy humans and those
with lung cancer. Anal Biochem. 334:266–275. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mutter R, Lu B, Carbone DP, Csiki I,
Moretti L, Johnson DH, Morrow JD, Sandler AB, Shyr Y, Ye F and Choy
H: A phase II study of celecoxib in combination with paclitaxel,
carboplatin and radiotherapy for patients with inoperable stage
IIIA/B non-small cell lung cancer. Clin Cancer Res. 15:2158–2165.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Csiki I, Morrow JD, Sandler A, Shyr Y,
Oates J, Williams MK, Dang T, Carbone DP and Johnson DH: Targeting
cyclooygenase-2 in recurrent non-small cell lung cancer: A phase II
trial of celecoxib and docetaxel. Clin Cancer Res. 11:6634–6640.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kurose K, Ohue Y, Sato E, Yamauchi A,
Eikawa S, Isobe M, Nishio Y, Uenaka A, Oka M and Nakayama E:
Increase in activated Treg in TIL in lung cancer and in vitro
depletion of Treg by ADCC using an antihuman CCR4 mAb (KM2760). J
Thorac Oncol. 10:74–83. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang X, Miao X, Tan W, Ning B, Liu Z,
Hong Y, Song W, Guo Y, Zhang X, Shen Y, et al: Identification of
functional genetic variants in cyclooxygenase-2 and their
association with risk of esophageal cancer. Gastroenterology.
129:565–576. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yukawa T, Shimizu K, Maeda A, Yasuda K,
Saisho S, Okita R and Nakata M: Cyclooxygenaze-2 genetic variants
influence intratumoral infiltration of FoxP3-positive regulatory T
cells in non-small cell lung cancer. Oncol Rep. 33:74–80.
2015.PubMed/NCBI
|