Introduction
Lung cancer is the leading cancer in terms of
mortality and morbidity in the world, and adenocarcinomas are
common histological types of lung cancer (1,2). The
International Society for the Study of Lung Cancer (IASLC), the
American Thoracic Society and the European Respiratory Society
jointly published a histological classification of lung
adenocarcinomas in 2011 (3). The main
interest of such classification is its prognostic value, since
histological type is closely associated with clinical, pathological
and molecular parameters (4,5).
Mucinous adenocarcinoma is the rarest type of lung
adenocarcinoma (6). According to a
recent classification (3), mucinous
adenocarcinoma includes mucinous adenocarcinoma in situ,
minimally invasive adenocarcinoma and invasive mucinous
adenocarcinoma. These tumors tend to present KRAS mutations and
commonly lack thyroid transcription factor-1 expression, and
computed tomography (CT) usually indicates nodules of consolidation
with air bronchograms that are generally multinodular and
multilobular in distribution (5).
Mucinous adenocarcinoma of the lung is morphologically
characterized by tall columnar cells with abundant cytoplasm that
contain varying amounts of mucin (6,7). Mucus
secreted by cancer cells can commonly be discharged as sputum.
However, if airway obstruction happens, obstructive pneumonia
occurs immediately, since the mucus fails to drain (8–10).
Case report
The patient was a 60-year-old female. On October
2011, the patient developed fever, with a temperature fluctuation
between 37.5 and 39.0°C, in addition to cough and yellow sputum,
but no chills or shivering, abdominal pain or diarrhea, sore
throat, urinary frequency or urgency, or dysuria. In the Hospital
of Traditional Chinese Medicine, a CT scan of the chest revealed a
right lung space-occupying lesion, and the effect of anti-infective
therapy was poor. On April 16, 2012, when the patient was referred
to Zhengzhou People's Hospital (Zhengzhou, China), cough seriously
affected her daily life. Fiberoptic bronchoscope examination
revealed a mucinous membrane with black spots in the right upper
lobe anterior segmental bronchus. Bronchial brush cytology revealed
well differentiated respiratory epithelial cells and sporadic
neutrophilic granulocytes without malignant cells. Sputum
examination revealed gram-negative bacillus and gram-positive
cocci, no fungus spores or hypha, and no malignant cells. Sputum
culture identified Escherichia coli but no fungus. Thus,
anti-infective therapy (cefoperazone combined with levofloxacin)
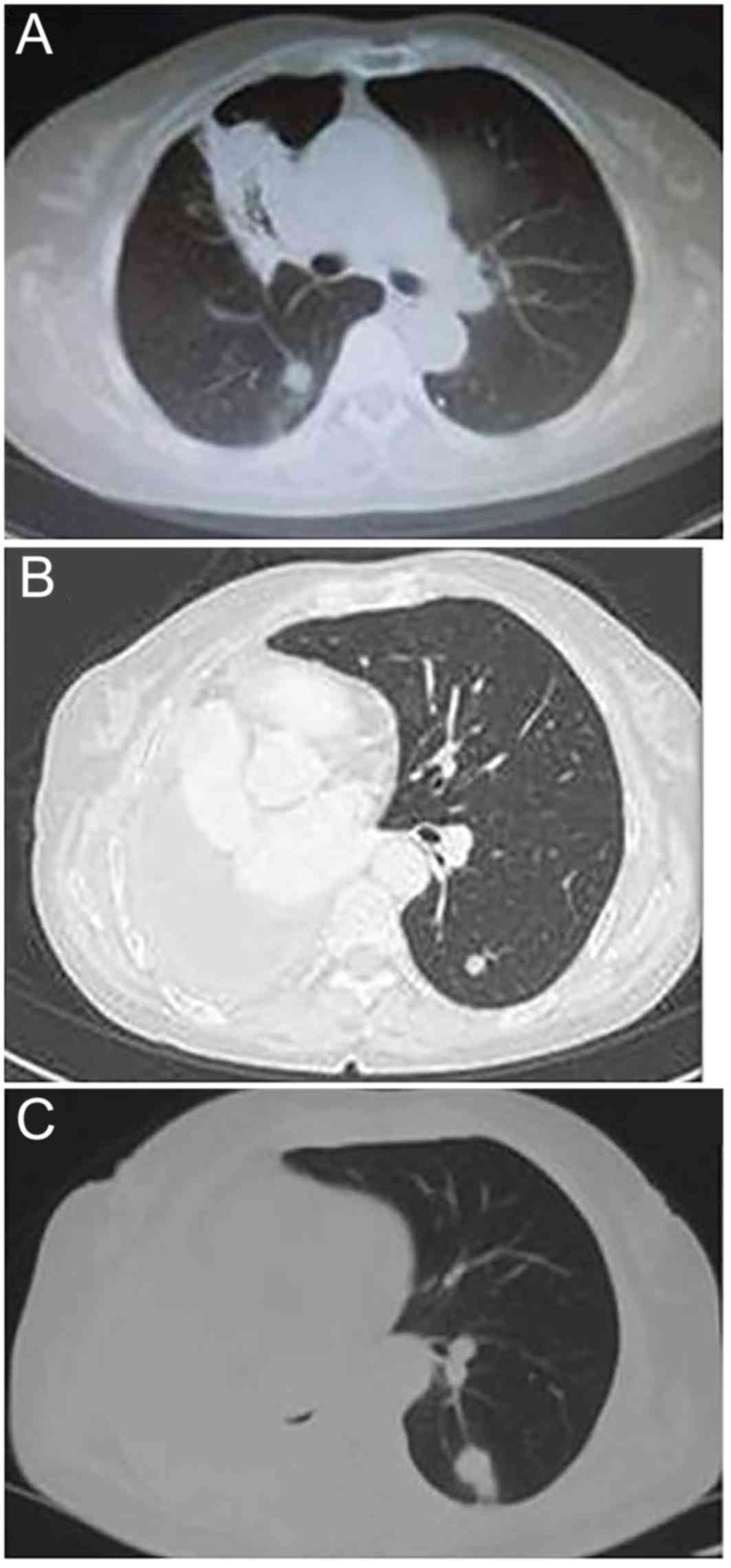
was administered for 2 weeks, but its effect was poor. Following
treatment, chest CT scans (Fig. 1A)
revealed that the right lung was characterized by large sheets,
multiple nodular high-density shadows, and the limited patchy
shadow was unchanged compared with that prior to treatment.
Purified protein derivative, acid-fast stain test of sputum smear
and T-SPOT.TB assays (Oxford Immunotec Ltd., Abingdon, UK;
performed according to the manufacturer's protocol) were all
negative. The respiratory symptoms became increasingly severe.
Thoracic surgeons suggested a thoracic exploratory operation. The
patient received a routine preoperative examination, and in May
2012, the patient underwent surgical treatment. The findings of the
operation revealed that the whole right lung was distributed
diffusely by a space-occupying lesion. Therefore, a right
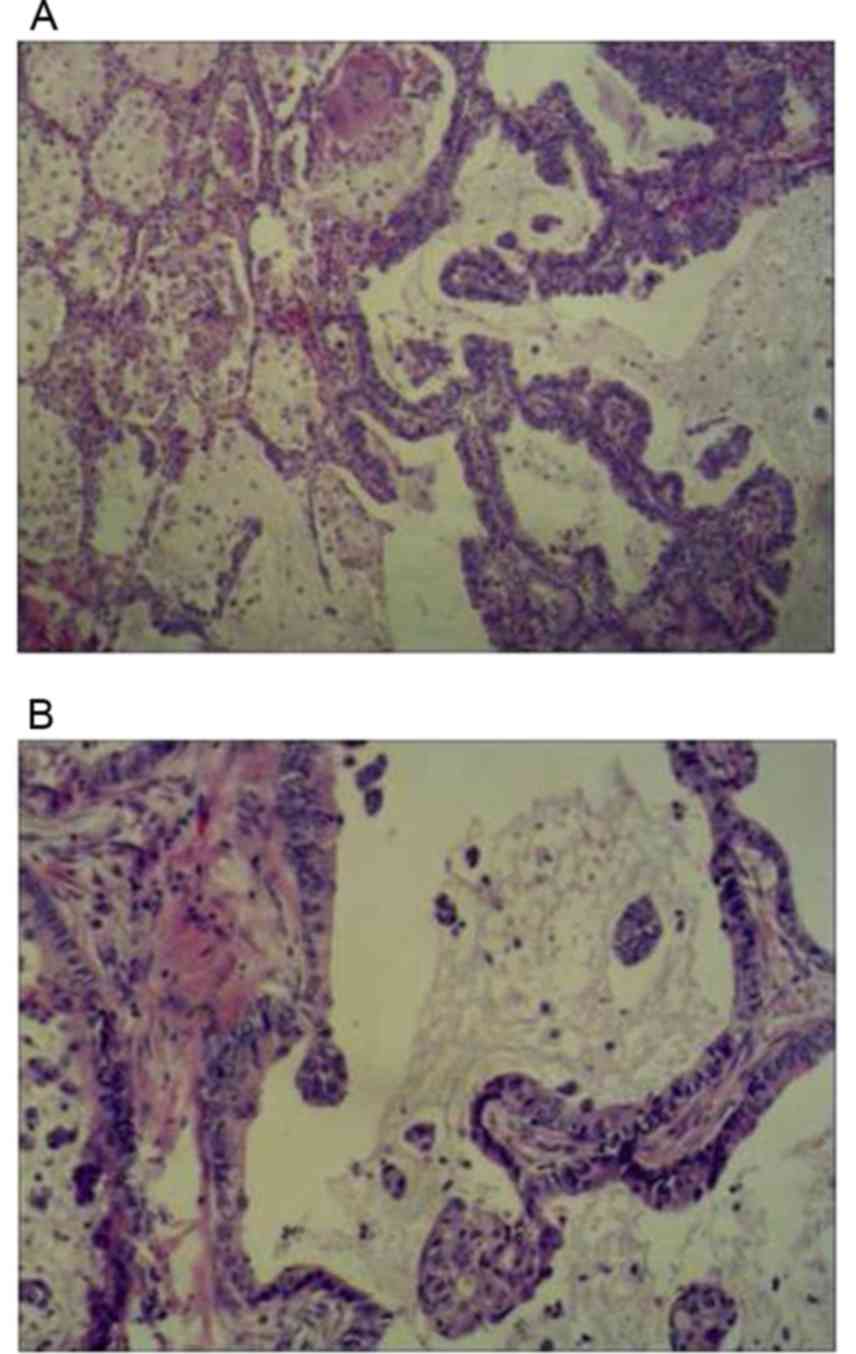
pneumonectomy was performed. Postoperative pathology demonstrated
lung mucinous adenocarcinoma. The histopathology also revealed no
mutations in epidermal growth factor receptor (EGFR). According to
the 2009 tumor-node-metastasis classification by the IASLC
(11–13), the pathological stage was determined
to be cT4N0M0, IIIA (Fig. 2). The
Eastern Cooperative Oncology Group performance status was 1.
Adjuvant postoperative chemotherapy included four cycles of taxol
(135 mg/m2 on day 1) and cisplatin (75 mg/m2
on days 1–4). The patient experienced grade II bone marrow
suppression and grade III gastrointestinal reaction. The last
administration of taxol and cisplatin chemotherapy was on September
7, 2012. In December 2012, chest CT re-examination revealed
metastasis in the left lung (Fig.
1B). The patient received two cycles of chemotherapy based on
pemetrexed and cisplatin as second-line treatment. The last
administration of pemetrexed and cisplatin chemotherapy happened on
January 12, 2013. Subsequently, the patient terminated chemotherapy
and initiated treatment with Chinese herbs. On May 13, 2013, the
patient received a chest CT re-examination (Fig. 1C). On August 27, 2013, a re-examining
chest CT revealed metastasis in the left lung, which developed
slowly (Fig. 3A and B). The symptom
of a cough with white phlegm gradually appeared. The patient
experienced tightness in the chest in March 2014, and re-examining
chest CT revealed multiple metastases in the left lung (Fig. 3C and D). Therefore, the patient
received treatment consisting of two cycles of chemotherapy with
pemetrexed and cisplatin. The symptom of tightness in the chest
disappeared following chemotherapy. Anti-tumor therapy was
terminated again due to the financial situation of the patient's
family. The patient was re-examined on June 12, 2014 (Fig. 3E and F), November 10, 2014 (Fig. 3G and H), February 6, 2015 (Fig. 4A), February 16, 2015 (Fig. 4B), March 5, 2015 (Fig. 4C and D) and March 25, 2015 (Fig. 4E and F). Metastasis outside the left
lung did not appear. The patient succumbed to disease on May 18,
2015. Consent was obtained from the family of the patient.
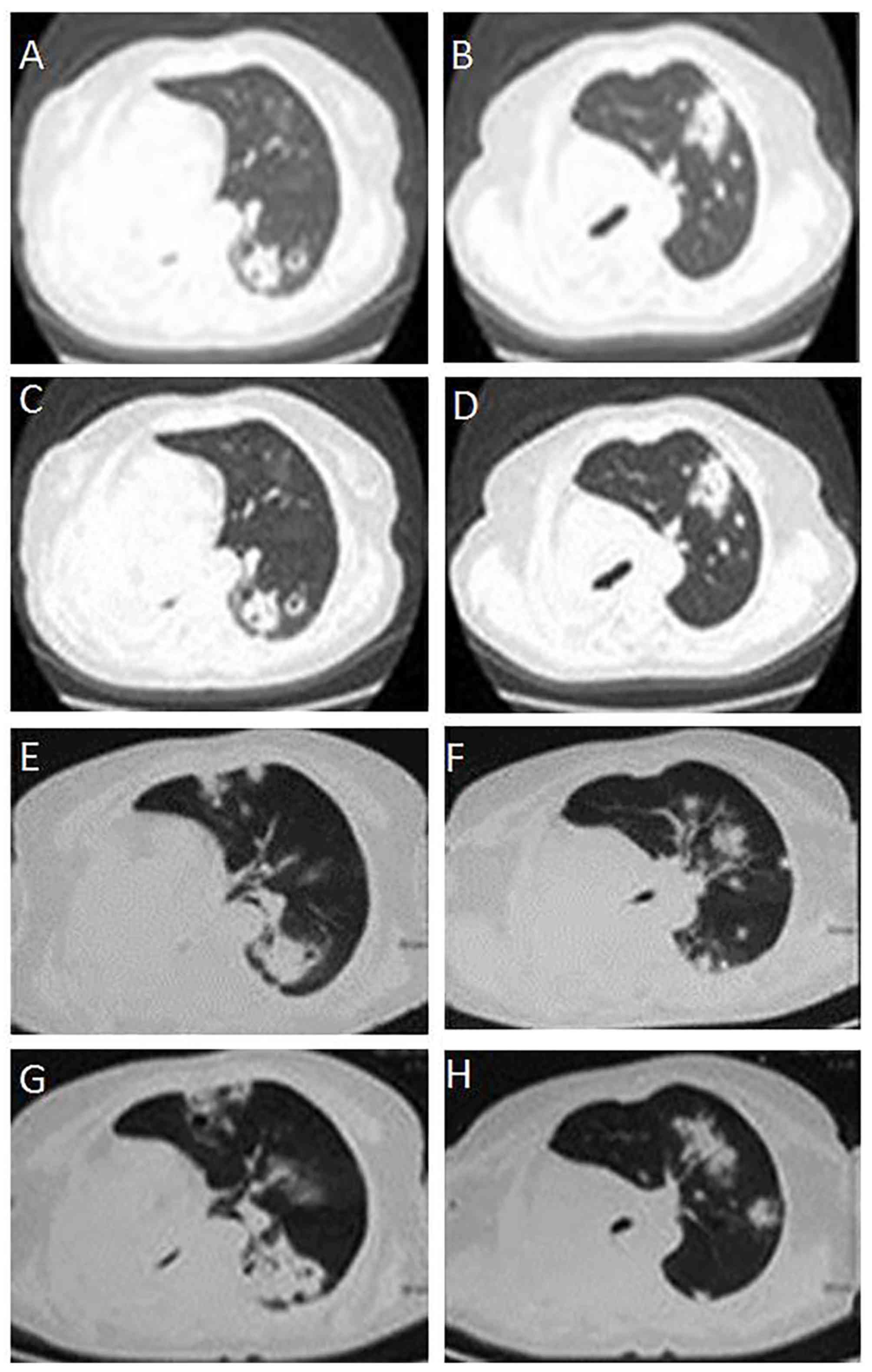 | Figure 3.CT scans of the development of
multiple metastases of the left lung in a patient with primary
mucinous adenocarcinoma. (A, B) Thoracic CT scans following surgery
in August 27, 2013, revealing multiple metastases of the left lung.
(C, D) Thoracic CT scans following surgery in March, 2014,
revealing that the metastases of left lung were stable. (E, F)
Thoracic CT scan following surgery in June 12, 2014, revealing an
increase in the number of metastases of the left lung. (G, H)
Thoracic CT scan following surgery on November 10, 2014, revealing
further increases in the number of metastases of the left lung. CT,
computer tomography. |
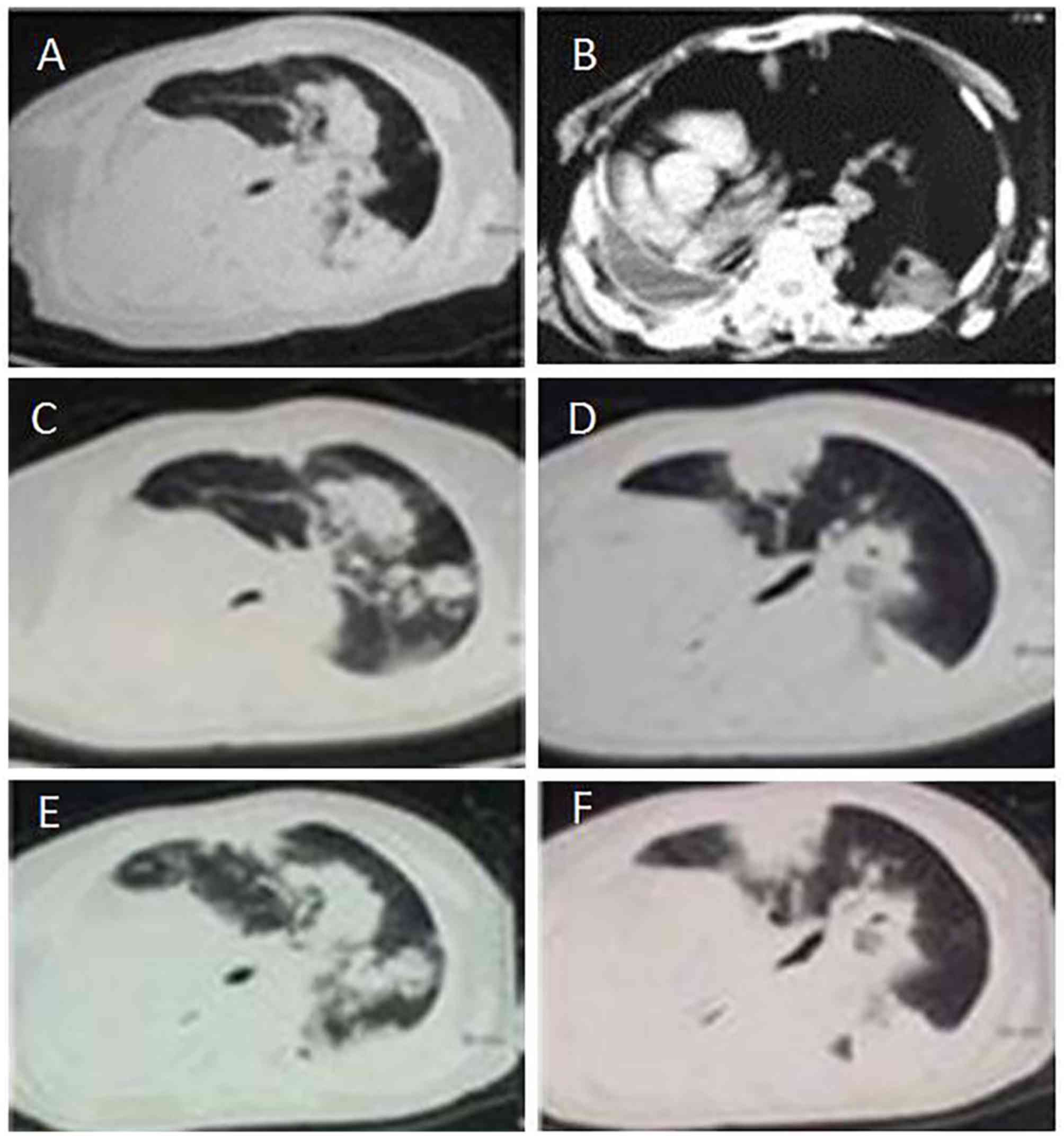 | Figure 4.CT scans of a patient with primary
mucinous adenocarcinoma from 2015. (A) Thoracic CT scan following
surgery on February 6, 2015, revealing a further increase in the
number of metastases of the left lung; (B) Thoracic CT scan
following surgery on February 16, 2015, revealing a pleural
effusion of the right lung and a severe right deviation of the
mediastinum; (C, D) CT scans following surgery on March 5, 2015,
revealing a further increased number of metastases of the left
lung; (E, F) CT scans following surgery on March 25, 2015,
revealing a further increased number of metastases of the left
lung. CT, computed tomography. |
Discussion
Mucinous adenocarcinoma is an uncommon histological
subtype of primary lung adenocarcinoma. Mucus production is a
typical feature of mucinous adenocarcinoma, which originates in
stem cells with the potential of multidirectional differentiation
and secrets mucus with different properties according to the
differentiation microenvironment (6).
Usually, the mucus secreted by cancer cells can be discharged as
sputum, but if the growth of cancer cells is uncontrolled, it may
cause excessive production of mucus, which obstructs the upper
airways. In consequence, obstructive pneumonia may arise (14).
A retrospective review of the medical history of the
patient of the present study revealed certain clinical features of
lung mucinous adenocarcinoma: i) During the course of the disease,
the patient recurrently coughed with abundant white phlegm, despite
the fact that the patient had no history of tobacco smoking or
respiratory diseases, and sputum examination was negative. Thus,
abundant white phlegm is associated with large quantities of mucus
secreted by cancer cells. This feature reflects the consistency of
the clinical symptoms with the biological behavior of cancer cells.
ii) Pemetrexed was an effective second-line chemotherapy for the
patient, since the symptom of chest tightness disappeared following
two cycles of chemotherapy with pemetrexed and cisplatin, although
cough and expectoration remained. Mucinous adenocarcinoma is a
histological type of lung adenocarcinoma, and pemetrexed is used as
first-line chemotherapy in patients with lung adenocarcinoma.
Therefore, the variation of the clinical symptoms prior to and
following treatment was associated with histopathology. iii) In the
present patient, the lesions were confined to the lungs from the
time of initial detection to mortality, and there was no metastasis
to extrapulmonary organs. iv) The time span from diagnosis to
mortality was >3.5 years, and the survival time was long despite
the eight-cycle chemotherapy received by the patient. v) The rate
of EGFR mutations is low in lung mucinous adenocarcinoma, as the
patient had no mutation in EGFR from exons 18 to 21. vi) The
clinical characteristics of the patient were cough, expectoration,
fever, chest distress, no hemoptysis and pain.
The survival time of the patient was >3.5 years,
as a result of a joint effort of the Departments of Oncology, Chest
Surgery, Pathology and Imaging at Zhengzhou People's Hospital,
which reflects the multidisciplinary team nature of
oncotherapy.
In conclusion, lung mucinous adenocarcinoma is
uncommon, but its prognosis is poor. Through the present case
report, the clinical characteristics of lung mucinous
adenocarcinoma were reviewed. Further understanding of this disease
will help to improve the diagnosis and treatment. The
identification of novel medicines and therapeutic methods for lung
mucinous adenocarcinoma is urgent.
References
|
1
|
Ma NQ, Liu LL, Min J, Wang JW, Jiang WF,
Liu Y, Feng YG, Su HC, Feng YM and Zhang HL: The effect of down
regulation of calcineurin Aα by lentiviral vector-mediated RNAi on
the biological behavior of small-cell lung cancer and its bone
metastasis. Clin Exp Metastasis. 28:765–778. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liu Y, Zhang Y, Min J, Liu LL, Ma NQ, Feng
YM, Liu D, Wang PZ, Huang DD, Zhuang Y and Zhang HL: Calcineurin
promotes proliferation, migration, and invasion of small cell lung
cancer. Tumour Biol. 31:199–207. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Travis WD, Brambilla E, Noguchi M,
Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ,
Van Schil PE, et al: IInternational association for the study of
lung cancer/american thoracic society/european respiratory society
international multidisciplinary classification of lung
adenocarcinoma. J Thorac Oncol. 6:244–285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mansuet-Lupo A, Bobbio A, Blons H, Becht
E, Ouakrim H, Didelot A, Charpentier MC, Bain S, Marmey B, Bonjour
P, et al: The new histologic classification of lung primary
adenocarcinoma subtypes is a reliable prognostic marker and
identifies tumors with different mutation status: The experience of
a French cohort. Chest. 146:633–643. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen Z, Liu X, Zhao J, Yang H and Teng X:
Correlation of EGFR mutation and histological subtype according to
the IASLC/ATS/ERS classification of lung adenocarcinoma. Int J Clin
Exp Pathol. 7:8039–8045. 2014.PubMed/NCBI
|
|
6
|
Marchetti A, Buttitta F, Pellegrini S,
Chella A, Bertacca G, Filardo A, Tognoni V, Ferreli F, Signorini E,
Angeletti CA and Bevilacqua G: Bronchioloalveolar lung carcinomas:
K-ras mutations are constant events in the mucinous subtype. J
Pathol. 179:254–259. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Travis WD, Brambilla E and Riely GJ: New
pathologic classification of lung cancer: Relevance for clinical
practice and clinical trials. J Clin Oncol. 31:992–1001. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Marchetti A, Buttitta F, Pellegrini S,
Chella A, Bertacca G, Filardo A, Tognoni V, Ferreli F, Signorini E,
Angeletti CA and Bevilacqua G: Bronchioloalveolar lung carcinomas:
K-ras mutations are constant events in the mucinous subtype. J
Pathol. 179:254–259. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nakaoku T, Tsuta K, Ichikawa H, Shiraishi
K, Sakamoto H, Enari M, Furuta K, Shimada Y, Ogiwara H, Watanabe S,
et al: Druggable oncogene fusions in invasive mucinous lung
adenocarcinoma. Clin Cancer Res. 20:3087–3093. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cai D, Li H, Wang R, Li Y, Pan Y, Hu H,
Zhang Y, Gong R, Pan B, Sun Y and Chen H: Comparison of clinical
features, molecular alterations, and prognosis in morphological
subgroups of lung invasive mucinous adenocarcinoma. Onco Targets
Ther. 7:2127–2132. 2014.PubMed/NCBI
|
|
11
|
Goldstraw P: The 7th Edition of TNM in
Lung Cancer: What now? J Thorac Oncol. 4:671–673. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Giroux DJ, Rami-Porta R, Chansky K,
Crowley JJ, Groome PA, Postmus PE, Rusch V, Sculier JP, Shepherd
FA, Sobin L, et al: The IASLC lung cancer staging project: Data
elements for the prospective project. J Thorac Oncol. 4:679–683.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rusch VW, Asamura H, Watanabe H, Giroux
DJ, Rami-Porta R and Goldstraw P: Members of IASLC Staging
Committee: The IASLC lung cancer staging project: a proposal for a
new international lymph node map in the forthcoming seventh edition
of the TNM classification for lung cancer. J Thorac Oncol.
4:568–577. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Higashiyama M, Doi O, Kodama K, Yokouchi H
and Tateishi R: Cystic mucinous adenocarcinoma of the lung. Two
cases of cystic variant of mucus-producing lung adenocarcinoma.
Chest. 101:763–766. 1992. View Article : Google Scholar : PubMed/NCBI
|