Introduction
Hepatocellular carcinoma (HCC) is the most common
primary malignancy of the liver with an estimated annual death
incidence of approximately 700,000 worldwide (1,2). In
Taiwan, it is the second most common cause of cancer death and
causes more than 7,500 deaths each year (3). Surgical resection remains the most
effective therapy in selected patients, but approximately 75% of
patients with HCC have advanced unresectable diseases upon
presentation. In order to improve long-term outcome of patients
with HCC, numerous efforts were made to unravel the risk factors
for and pathogenesis of poor prognosis for HCC.
Cytokeratin 19 (CK19) is a biliary epithelial cell
marker and is generally expressed in intrahepatic
cholangiocarcinoma (ICC) cells (4,5). Studies
have shown that the expression of CK19 in primary HCC is associated
with poorer outcome (6). There have
also been studies demonstrating that CK19 expression in primary HCC
is a significant risk factor for developing lymph node metastasis
(LNM) (4,7,8). Compared
with other malignancies such as lung cancer, esophageal cancer,
renal cancer, gastric cancer, and intra-hepatic cholangiocarcinoma,
the incidence of LNM in primary HCC is low, and the prognosis is
poor when LNM occurs (9–11). HCC with CK19 expression, subsequently,
may be a special subtype of HCC with distinct clinical behavior
from HCC without CK19 expression (8).
Due to its worse prognosis, it is therefore of clinical
significance to elucidate the pathogenesis of CK19-positive
[CK19(+)] HCC. In the meanwhile, cadherin-17 (CDH17) was shown to
be associated with vascular invasion and tumor metastasis in HCC
(12). Similar to α-fetoprotein
(AFP), CDH17 is present only in fetal liver and gastrointestinal
tract during embryogenesis, and the gene becomes silenced in
healthy adult liver and stomach tissues. It functions as a peptide
transporter and a cell adhesion molecule to maintain tissue
integrity in epithelia (13). To
date, there is little report to dissect the mechanistic
relationship between CK19 and CDH17 in CK19(+) HCC. As a result,
the purpose of this study was to investigate whether CDH17 is
responsible for the invasiveness and poor prognosis of CK19(+)
HCC.
Materials and methods
Patients
For the years from 2007 to 2012, records of patients
with histological proven primary HCC from the Cancer Registry of
the Cancer Center, Chang Gung Memorial Hospital (Taoyuan, Taiwan),
were retrospectively reviewed. Since hepatitis B virus (HBV)
infection remains the most common etiology of HCC in Taiwan
(11), we recruited HBV-related HCC
(HBV-HCC) first for the current study. The inclusion criteria of
current study was defined as resectable lesions without distant
metastasis by image study, including sonography, computed
tomography (CT), and angiography. Only patients who received
curative hepatectomy as initial primary treatment for HCC were
included. Patients who had unresectable disease, synchronous
cancers, recurrent cancers, distant metastasis or previous history
of other malignancy preoperatively were excluded from the study.
Their clinico-pathological data were retrieved from the
prospectively collected database. The following variables were
included in the analyses: Age, sex, cigarette smoking, alcohol
consumption, HBV infection, anti-hepatitis C virus antibody
(anti-HCV) level, alkaline phosphotase level, bilirubin level,
preoperative AFP and carcinoembryonic antigen (CEA) level,
Child-Pugh classification, tumor size, tumor-LNM status, tumor
encapsulation, histological grade, vascular invasion, tumor
rupture, daughter nodules, resection margin, and long-term
survival. The study endpoint was 30 June 2015, and tumor staging
was based on the 7th edition of American Joint Committee on Cancer
(AJCC) TNM staging system for HCC (14). This study was approved by the
Institutional Review Boards (IRB 103-2225C) of Chang Gung Memorial
Hospital.
Immunohistochemistry (IHC)
Formalin-fixed and paraffin-embedded resection
specimens were sectioned to 4 µm in thickness and deparaffininzed,
rehydrated, and processed for antigen retrieval. The slides were
further incubated with appropriate dilutions of the following
antibodies (Ab) at room temperature for 1 h (CK19 Ab; Abcam, San
Francisco, CA, USA; and CDH17 Ab; LifeSpan Biosciences, Seattle,
WA, USA). After incubation, the slides were washed 3 times in
phosphate-buffered saline (PBS), incubated with a horse reddish
peroxidase conjugated antibody polymer (Zymed; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) at room temperature for 10 min,
and then developed by treatment with 3,3′-diaminobenzidine (Roche
Diagnostics, Basel, Switzerland) at room temperature for 10 min. An
independent experienced pathologist without knowledge of patient
characteristics and outcome was asked to determine the results of
immunohistochemical staining under microscopy. A positive result
was defined as ≥10% of tumor cells stained positive for CK19 or
CDH17.
Western blot analysis
Total protein was extracted from each cell line,
boiled at 95°C for 5 min, and placed in 10% SDS-polyacrylamide gel
for electrophoresis. The protein images from the gel were
transferred to a nitrocellulose membrane and blocked with 5% nonfat
milk in PBST solution (PBS plus 0.15 Triton X-100). The membrane
was washed again and incubated again with anti-mouse immunoglobulin
G antibody conjugated with horseradish. The blots were probed with
antibodies specific for CK19 (Abcam) or CD17 (Lifespan Biosciences)
and appropriate secondary antibodies. Labeled bands were
subsequently detected by enhanced chemiluminescence (ECL;
Millipore, Bedford, MA, USA). For each sample, band intensities
were normalized to glyceraldehyde-3-phosphate dehydrogenase
(GAPDH).
Quantitative real-time PCR
(qRT-PCR)
The first-strand cDNA was synthesized from 5 µg of
total RNA, and 0.5 µl of cDNA will be mixed with Taqman probe
(Assay-on-Demand; Applied Biosystems, Foster City, CA, USA. Cat.
no. for CK19, Hs00761767_s1; for CDH17, Hs00900408_m1), RNase-free
water, and TaqMan Universal PCR Master Mix. Real-time PCR was
performed according to the manufacturer's protocol. GAPDH was used
as internal controls for gene expression. For normalized each
sample, the relative gene expression was calculated using the
differences in threshold cycles (Delta Ct, ΔCt), a calibrated ΔCt
value (ΔCt=Ct internal control-Ct sample).
For quantitation of gene expression levels between treated and
non-treated samples, the comparative Ct method (also
known as the 2−ΔΔCt method), where ΔΔCt =
ΔCt treated – ΔΔCt, non-treated,
was used.
Statistical analysis
The statistical analysis was performed with IBM SPSS
Statistics 21 (IBM Corp., Somers, NY, USA). Fisher's exact test and
Pearson's χ2 test were used to analyze categorical data.
Student's t-test was used to analyze quantitative variables.
Overall survival (OS) was defined by the time elapsing from the
date of diagnosis to either the date of death or the date of the
last contact. Disease-free survival (DFS) was calculated from the
date of surgery to the date of the first documented clinical
disease recurrence. Cases with surgical mortality, defined as death
within one month of surgery, were excluded from the survival
analyses. Kaplan-Meier analysis was used to determine the OS and
DFS. The log-rank test and Cox regression multivariate analysis
were applied to determine prognostic significance of
clinicopathological variables. Statistical significance was defined
as P<0.05.
Results
Patient demographics
A total of 114 HBV-HCC patients who underwent liver
resection were recruited for the current study. The median
follow-up time was 49.02 months (mean, 52.4 months). The mean age
of diagnosis was 55.7 year-old and about 80% patients were male. As
for preoperative liver function, 108 patients (97.3%) were
Child-Pugh A, while only 3 patients (2.7%) were Child-Pugh B. The
indocyanine green retention at 15 min (ICG-15) ≤10% were found in
75 patients (66.4%; mean ICG-15, 9.62%). The mean preoperative AFP
and CEA levels were 10,581.94 and 3.14 ng/ml, respectively. As for
pathological variables, the mean tumor size was 4.18 cm and 93
tumors (81.6%) were encapsulated. About one-fourth of tumors had
either micro- or macro-vascular invasion and 22 tumors (19.3%) had
daughter nodules. Tumor rupture was found in only 6 cases (5.3%).
R0 resection was achieved in the majority of patients (99.1%).
About half of the patients had histology-proven liver cirrhosis and
most patients (69.5%) had T1 disease. The clinico-pathological data
were summarized in Table I.
 | Table I.Demographic data of patients with
HBV-related hepatocellular carcinoma undergoing hepatectomy
(n=114). |
Table I.
Demographic data of patients with
HBV-related hepatocellular carcinoma undergoing hepatectomy
(n=114).
| A, Categorical
variables |
|---|
|
|---|
|
Variablesa | No. (%) |
|---|
| Age, ≤65 years | 90 (78.9) |
| Sex (male) | 90 (78.9) |
| Comorbidity |
|
Diabetes mellitus (yes) | 19 (16.8) |
|
Hypertension (yes) | 22 (19.3) |
|
ESRDb (yes) | 1 (0.9) |
| Smoking
(yes) | 21 (18.4) |
| Alcohol
(yes) | 16 (14.0) |
|
Child-pugh classification
(A/B/C) | 108 (97.3)/3
(2.7)/0 (0) |
|
Preoperative α-fetoprotein
(>200 ng/ml) | 54 (47.4) |
| ICG-15
(≤10%) | 75 (66.4) |
| Tumor
size (>5 cm) | 23 (20.2) |
| Tumor
encapsulation (yes) | 93 (81.6) |
| Tumor
rupture (yes) | 6 (5.3) |
|
Vascular invasion (yes) | 29 (25.4) |
|
Daughter nodules (yes) | 22 (19.3) |
|
Resection margin
(negative) | 113 (99.1) |
|
Edmonson and steiner
grade |
9(8.0)/59(52.2)/ |
|
(I/II/III/IV) |
40(35.4)/5(4.4) |
| Liver
cirrhosis (yes) | 58 (50.9) |
| Tumor
necrosis (yes) | 56 (49.1) |
| AJCC T
stage |
66(69.5)/18(18.9)/ |
|
(T1/T2/T3a/T3b/T4) |
8(8.4)/1(1.1)/2(2.1) |
| AJCC N
stage (N0) | 113 (99.1) |
|
| B, Continuous
variables |
|
|
Variablesa | Mean ±
SE |
|
| Age (years) | 55.7±1.09 |
| ICG-15 (%) | 9.62±1.02 |
| Preoperative
α-fetoprotein (ng/ml) |
10,581.94±5,851.93 |
| Preoperative CEA
(ng/ml) |
3.14±0.73 |
| Tumor size
(cm) | 4.18±0.24 |
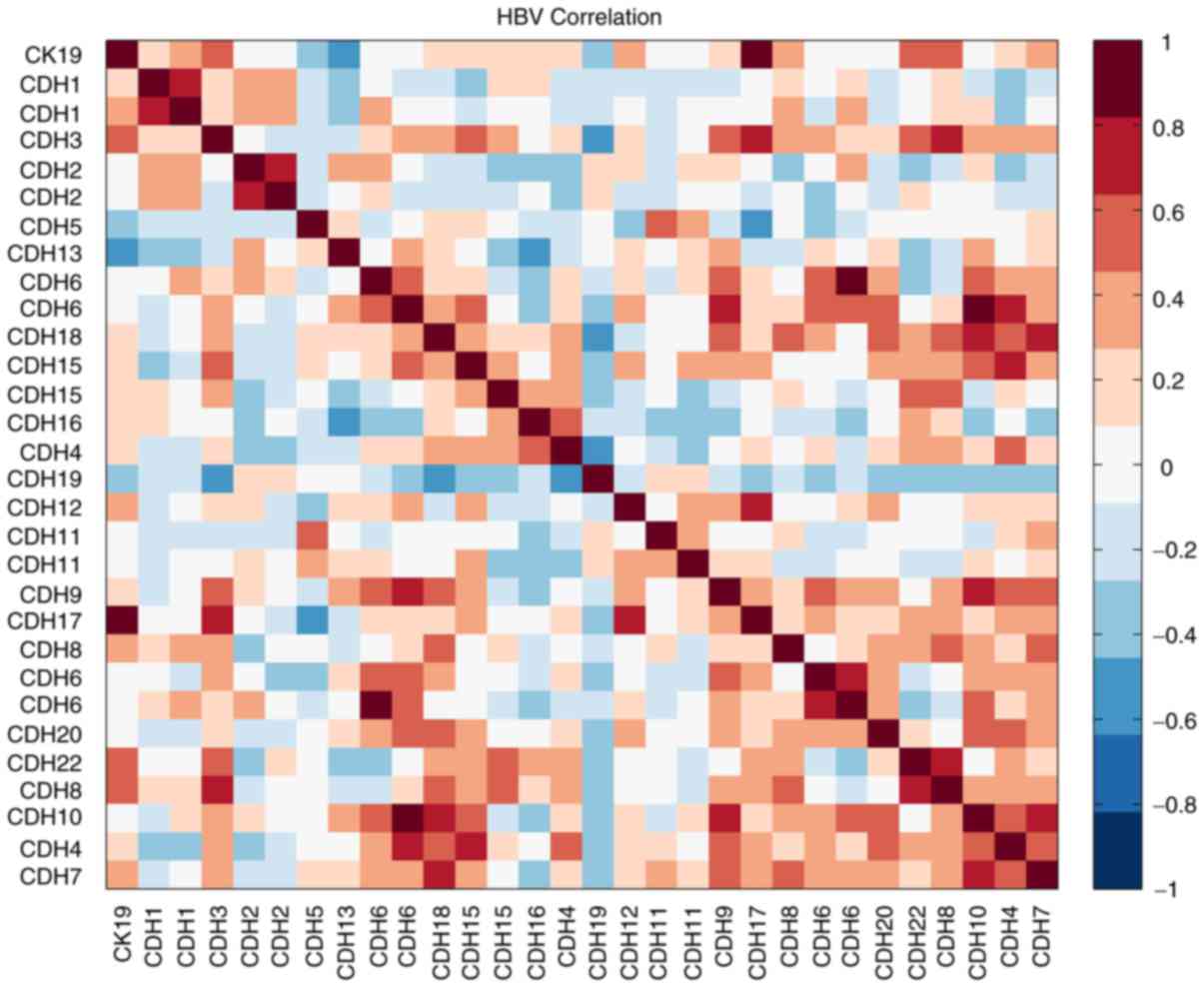
Microarray data mining and
immunohistochemical study
In our earlier study, we have established a dataset
for early stage HBV-HCC (<5 cm) patients (n=20) by using
Affymetrix U133A oligonucleotide microarray (15). We then took the advantage of this
dataset and tried to search for potential genes that might be
correlated with CK19 expression. After correlation analysis, we
found at least one important molecule, CDH17, that was
significantly correlated with CK19 expression in HBV-HCC
(R2: 0.867, P<0.001; Fig.
1).
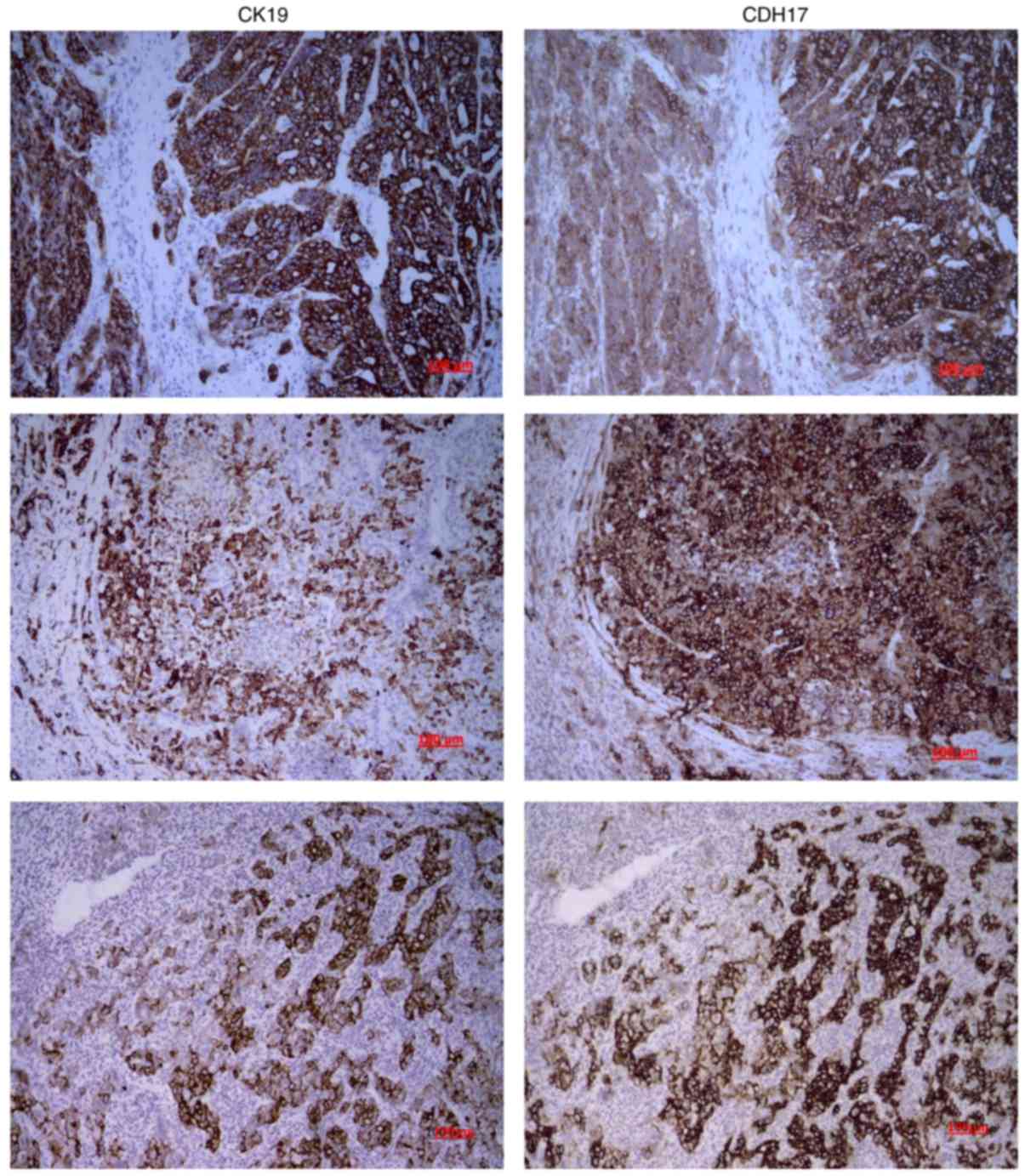
To further examine the correlation between CK19 and
CDH17 expression, immunohistochemical (IHC) study was performed and
the results were interpreted by experienced pathologists. CK19
expression was found in nine tumors (7.9%), and five tumors (4.4%)
showed immunopositivity for CDH17. Three patients showed
immuno-positivity for both CK19 and CDH17. While almost none of the
CK19(−) HCC showed CDH17 expression (2 out of 104 patients, 1.9%),
one-third of CK19(+) HCC had simultaneous CDH17 expression. The
Spearman's correlation coefficient was 0.414 and P-value was
<0.001. As demonstrated in Fig. 2,
the vast majority of the CK19(+) tumor cells in CK19(+) HCC also
had strong CDH17 expression. The expression of CK19 seemed to
coincide with that of CDH17 in these CK19(+) HCC.
Clinicopathological features and
survival analysis of CK19(+) or CDH17(+) HCC
As shown in Table II,
CK19 expression was significantly associated with LNM and CDH17
expression (P<0.001, respectively). In addition, CK19(+) HCC was
more likely to have elevated preoperative AFP >200 ng/ml. In the
meanwhile, CDH17 expression was also significantly associated with
LNM and CK19 expression (P<0.001, respectively). Moreover,
CDH17(+) HCC was more likely to be poorly-differentiated tumors and
have vascular invasion (Table
III).
| Table II.The relationship between
clinicopathological variables and CK19 expression in hepatocellular
carcinoma (n=114). |
Table II.
The relationship between
clinicopathological variables and CK19 expression in hepatocellular
carcinoma (n=114).
|
| CK19a |
|---|
|
|
|
|---|
|
| Negative (%) | Positive (%) | P-value |
|---|
| Age (years) |
|
≤65 | 82 (78.1) | 8 (88.9) | 0.446 |
|
>65 | 23 (21.9) | 1 (11.1) |
|
| Sex |
|
Male | 85 (81.0) | 5 (55.6) | 0.073 |
|
Female | 20 (19.0) | 4 (44.4) |
|
| Child-Pugh
classification |
| A | 99 (97.1) | 9 (100) | 0.564 |
| B | 3 (2.9) | 0 (0) |
|
| ICG-15 (%) |
|
≤10 | 71 (68.3) | 4 (44.4) | 0.147 |
|
>10 | 33 (31.7) | 5 (55.6) |
|
| α-fetoprotein
(ng/ml) |
|
≤200 | 58 (55.2) | 2 (22.2) | 0.057 |
|
>200 | 47 (44.8) | 7 (77.8) |
|
| Size (cm) |
| ≤5 | 85 (81.0) | 6 (66.7) | 0.305 |
|
>5 | 20 (19.0) | 3 (33.3) |
|
| LN metastasis |
|
Yes | 0 (0) | 2 (22.2) | <0.001 |
| No | 87 (100) | 7 (77.8) |
|
| CDH17
expressionb |
|
Positive | 2 (1.9) | 3 (33.3) | <0.001 |
|
Negative | 102 (98.1) | 6 (66.7) |
|
| Encapsulation |
|
Yes | 86 (81.9) | 7 (77.8) | 0.759 |
| No | 19 (18.1) | 2 (22.2) |
|
| Vascular
invasion |
|
Yes | 25 (23.8) | 4 (44.4) | 0.173 |
| No | 80 (76.2) | 5 (55.6) |
|
| Tumor rupture |
|
Yes | 5 (4.8) | 1 (11.1) | 0.413 |
| No | 100 (95.2) | 8 (88.9) |
|
| Daughter
nodules |
|
Yes | 19 (18.1) | 3 (33.3) | 0.266 |
| No | 86 (81.9) | 6 (66.7) |
|
| Resection
margin |
|
Positive | 1 (1.0) | 0 (0) | 0.769 |
|
Negative | 104 (99.0) | 9 (100.0) |
|
| Edmonson and
steiner grade |
|
I/II | 62 (59.6) | 6 (66.7) | 0.678 |
|
III/IV | 42 (40.4) | 3 (33.3) |
|
| Tumor necrosis |
|
Yes | 52 (49.5) | 4 (44.4) | 0.770 |
| No | 53 (50.5) | 5 (55.6) |
|
| Table III.Relationship between
clinicopathological variables and CDH17 expression in
hepatocellular carcinoma. |
Table III.
Relationship between
clinicopathological variables and CDH17 expression in
hepatocellular carcinoma.
| Hepatocellular
carcinoma (n=114) |
|---|
|
|---|
|
| CDH17a |
|---|
|
|
|
|---|
| Variable | Negative (%) | Positive (%) | P-value |
|---|
| Age (years) |
|
≤65 | 86 (79.6) | 4 (80.0) | 0.984 |
|
>65 | 22 (20.4) | 1 (20.0) |
|
| Sex |
|
Male | 85 (78.7) | 4 (80.0) | 0.945 |
|
Female | 23 (21.3) | 1 (20.0) |
|
| Child-Pugh
classification |
| A | 102 (97.1) | 5 (100) | 0.702 |
| B | 3 (2.9) | 0 (0) |
|
| ICG-15 |
|
≤10 | 72 (67.3) | 2 (40.0) | 0.208 |
|
>10 | 35 (32.7) | 3 (60.0) |
|
| α-fetoprotein
(ng/ml) |
|
≤200 | 58 (53.7) | 2 (40.0) | 0.548 |
|
>200 | 50 (46.3) | 3 (60.0) |
|
| Size (cm) |
| ≤5 | 86 (79.6) | 4 (80.0) | 0.984 |
|
>5 | 22 (20.4) | 1 (20.0) |
|
| LN metastasis |
|
Yes | 0 (0) | 2 (40.0) | <0.001 |
| No | 89 (100) | 3 (60.0) |
|
| CK19
expressionb |
|
Positive | 6 (5.6) | 3 (60.0) | <0.001 |
|
Negative | 102 (94.4) | 2 (40.0) |
|
| Encapsulation |
|
Yes | 90 (83.3) | 3 (60.0) | 0.296 |
| No | 18 (16.7) | 2 (40.0) |
|
| Vascular
invasion |
|
Yes | 26 (24.1) | 3 (60.0) | 0.072 |
| No | 82 (75.9) | 2 (40.0) |
|
| Tumor rupture |
|
Yes | 5 (4.6) | 1 (20.0) | 0.134 |
| No | 103 (95.4) | 4 (80.0) |
|
| Daughter
nodules |
|
Yes | 20 (18.5) | 1 (20.0) | 0.934 |
| No | 88 (81.5) | 4 (80.0) |
|
| Resection
margin |
|
Positive | 1 (0.9) | 0 (0) | 0.829 |
|
Negative | 107 (99.1) | 5 (100) |
|
| Edmonson and
Steiner grade |
|
I/II | 67 (62.6) | 1 (20.0) | 0.057 |
|
III/IV | 40 (37.4) | 4 (80.0) |
|
| Tumor necrosis |
|
Yes | 52 (48.1) | 4 (80.0) | 0.164 |
| No | 56 (51.9) | 1 (20.0) |
|
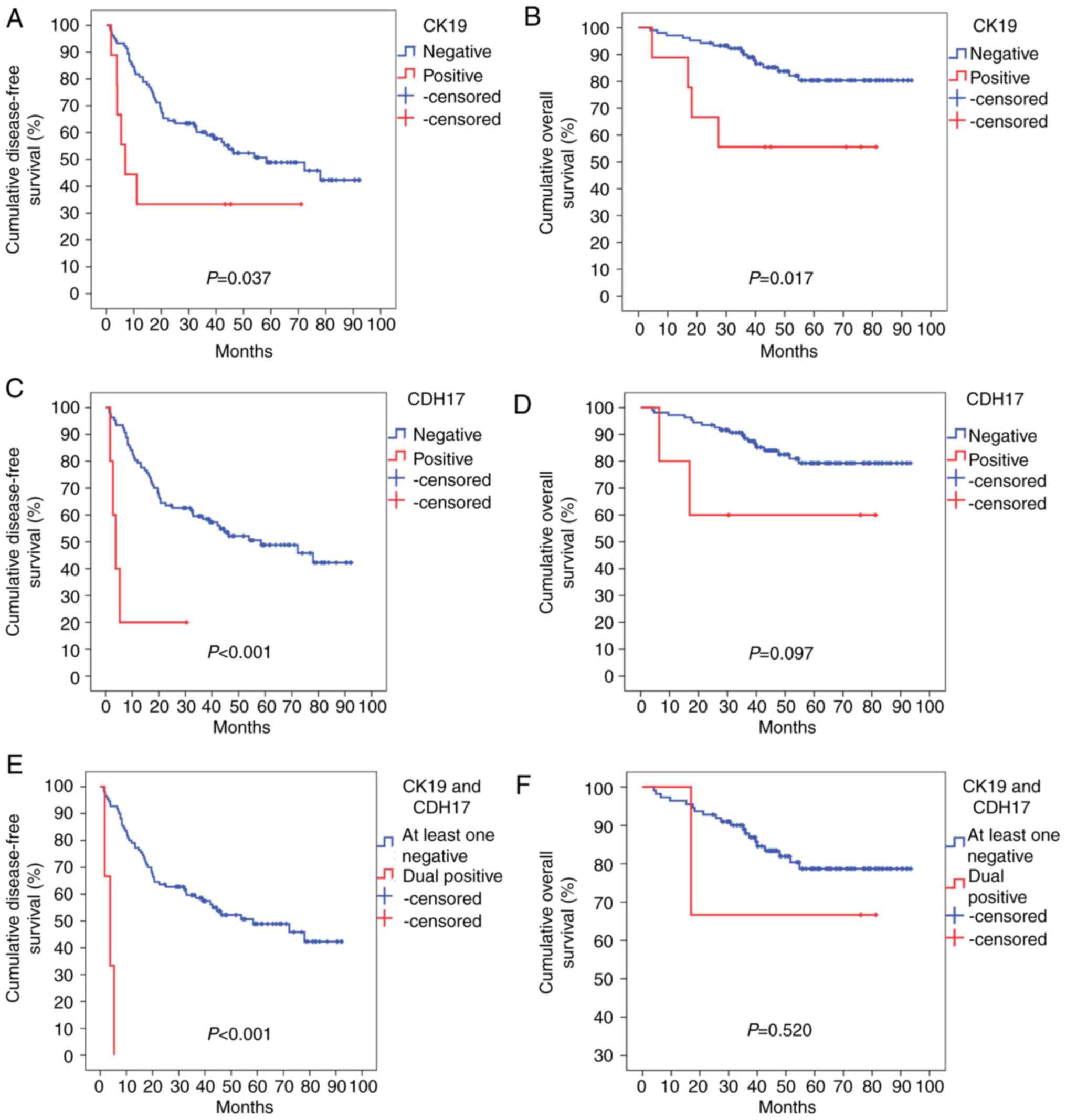
As for survival analysis, CK19(+) HCC had a mean DFS
of only 27.3±10.33 months, while CK19(−) HCC could remain disease
free for a mean of 54.7±3.75 months (P=0.037). CDH17 expression was
also a significantly poor prognostic factor for DFS in HCC, with
CDH17(+) HCC having a mean DFS of only 8.8±4.86 months (vs.
54.4±3.70 months for CDH17(−) HCC, P<0.001). In CK19(+) HCC,
CDH17 expression seemed to further promote tumor recurrence that
DFS was only 3.6±1.06 months (vs. 54.4±3.68 months for dual
negative or single positive HCC, P<0.001). Moreover, the early
recurrence rate was extremely high if HCC expressed both CK19 and
CDH17. The three dual-immunopositive HCC patients all had tumor
relapse within 2 years after the operation, compared to only 36%
(40 out of 111 patients) in dual negative or single positive
patients (P=0.024). CK19 expression was also a poor prognostic
factor for OS, with CK19(+) HCC having a mean OS of 52.6±10.83
months (vs. 81.5±2.62 months for CK19(−) HCC, P=0.017). CDH17
expression, on the other hand, was not significantly related to a
worse OS (53.4±15.32 vs. 80.7±2.65 months for CDH17(+) and CDH17(−)
HCC, respectively, P=0.097). Fig. 3
demonstrated the DFS and OS of respective type of HCC.
After Cox regression multivariate analysis, we
further demonstrated that CDH17 expression and ICG-15 >10% were
the most significant independent poor prognostic factors for DFS
(P=0.010 and 0.002, respectively) (Table
IV). Male sex and CK19 expression, on the other hand, were
independent poor prognostic factors for OS (P=0.030 and 0.041,
respectively) (Table V).
| Table IV.Cox regression multivariate analyses
of factors associated with disease-free survival in hepatocellular
carcinoma after hepatectomy. |
Table IV.
Cox regression multivariate analyses
of factors associated with disease-free survival in hepatocellular
carcinoma after hepatectomy.
|
| Multivariate
analysis |
|---|
|
|
|
|---|
| Variable | Hazard ratio (95%
CI) | P-value |
|---|
| ICG-15,
>10% | 2.375
(1.230–4.587) | 0.010 |
| Tumor size, >5
cm | 1.405
(0.515–3.840) | 0.506 |
| Vascular
invasion | 1.474
(0.434–5.008) | 0.534 |
| Daughter
nodule | 1.664
(0.640–4.326) | 0.296 |
| AJCC T stage |
| 0.422 |
| T2 vs.
T1 | 1.794
(0.578–5.565) | 0.312 |
| T3a vs.
T1 | 2.897
(0.423–19.843) | 0.279 |
| T3b vs.
T1 | 9.842
(0.922–105.059) | 0.058 |
| T4 vs.
T1 | 1.474
(0.248–8.741) | 0.669 |
| AJCC N stage | 2.813
(0.132–59.960) | 0.508 |
| CK19
expression | 2.859
(0.917–8.908) | 0.070 |
| CDH17
expression | 8.894
(2.280–34.701) | 0.002 |
| Table V.Cox regression multivariate analyses
of factors associated with overall survival in hepatocellular
carcinoma after hepatectomy. |
Table V.
Cox regression multivariate analyses
of factors associated with overall survival in hepatocellular
carcinoma after hepatectomy.
|
| Multivariate
analysis |
|---|
|
|
|
|---|
| Variable | Hazard ratio (95%
CI) | P-value |
|---|
| Male sex | 10.088
(1.253–81.197) | 0.030 |
| ICG-15,
>10% | 2.530
(0.938–6.820) | 0.067 |
| Tumor size, >5
cm | 2.385
(0.770–7.386) | 0.132 |
| Tumor rupture | 1.387
(0.255–7.527) | 0.705 |
| Vascular
invasion | 1.941
(0.716–5.265) | 0.193 |
| Daughter
nodule | 1.869
(0.696–5.021) | 0.215 |
| Tumor necrosis | 3.246
(0.933–11.288) | 0.064 |
| CK19
expression | 4.480
(1.066–18.838) | 0.041 |
Causal relationship between CK19 and
CDH17 in HCC
To further explore the causal relationship between
CK19 and CDH17 expressions in HCC, various HCC cell lines were
employed to conduct in vitro studies. The expression
profiles of CK19 and CDH17 in HCC cell lines including Huh7, Hep3B,
HepG2, and PLC5 were determined by Western blot analysis. As shown
in Fig. 4A, Hep3B, Huh7, and PLC5
were strongly positive for CK19 expression, while HepG2 was
essentially a CK19(−) HCC cell line. On the other hand, Hep3B and
Huh7 had strong CDH17 expression, while HepG2 and PLC5 only had
faint CDH17 expression. To induce CK19 expression in CK19(−) HCC
cell line, epidermal growth factor (EGF) was treated to HepG2 cell
line and real-time qPCR as well as western blot analysis were
performed (7). As shown in Fig. 4B and C, the expression of CK19 was
enhanced significantly after EGF treatment, and that of CDH17 was
also increased dramatically under EGF treatment (P<0.001,
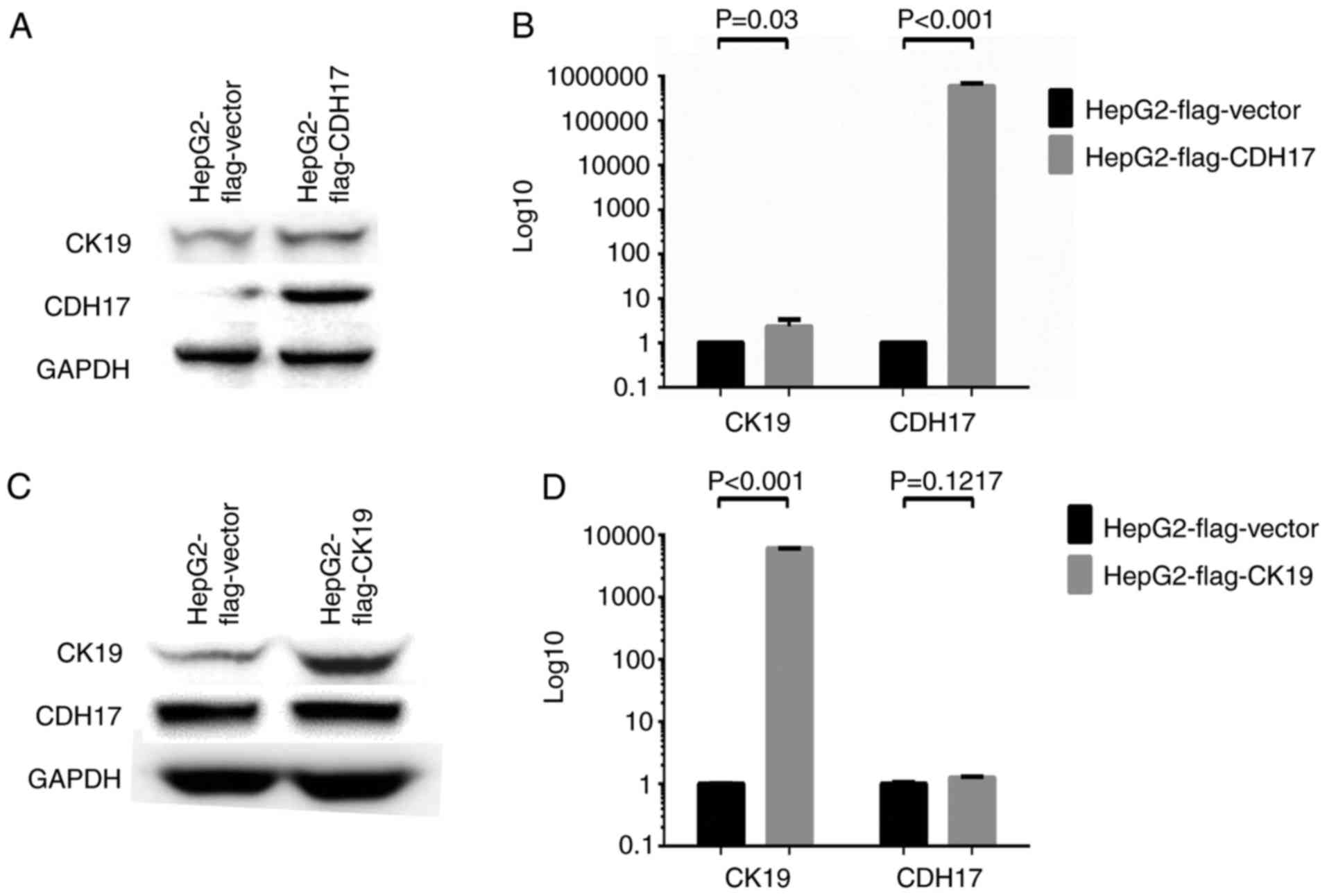
respectively). To further dissect the relationship between these
two molecules, CK19 or CDH17 was overexpressed in HepG2 and the
result was demonstrated in Fig. 5.
The transfection of FLAG®-CDH17 into HepG2 resulted in
enhanced expression of both CDH17 and CK19. The mRNA transcripts of
CDH17 and CK19 increased by 598,918 folds and 2.32 folds,
respectively, after transfection (P=0.03 and <0.001,
respectively) (Fig. 5A and B). On the
other hand, while both CK19 mRNA and protein levels were enhanced
significantly after FLAG®-CK19 transfection in HepG2
(P<0.001), the level of CDH17 remained unchanged after the
transfection (Fig. 5C and D). The
result indicated that CDH17 was not downstream to CK19. In
contrast, it was upstream to CK19 and, like CK19, was regulated by
a common signal such as EGF.
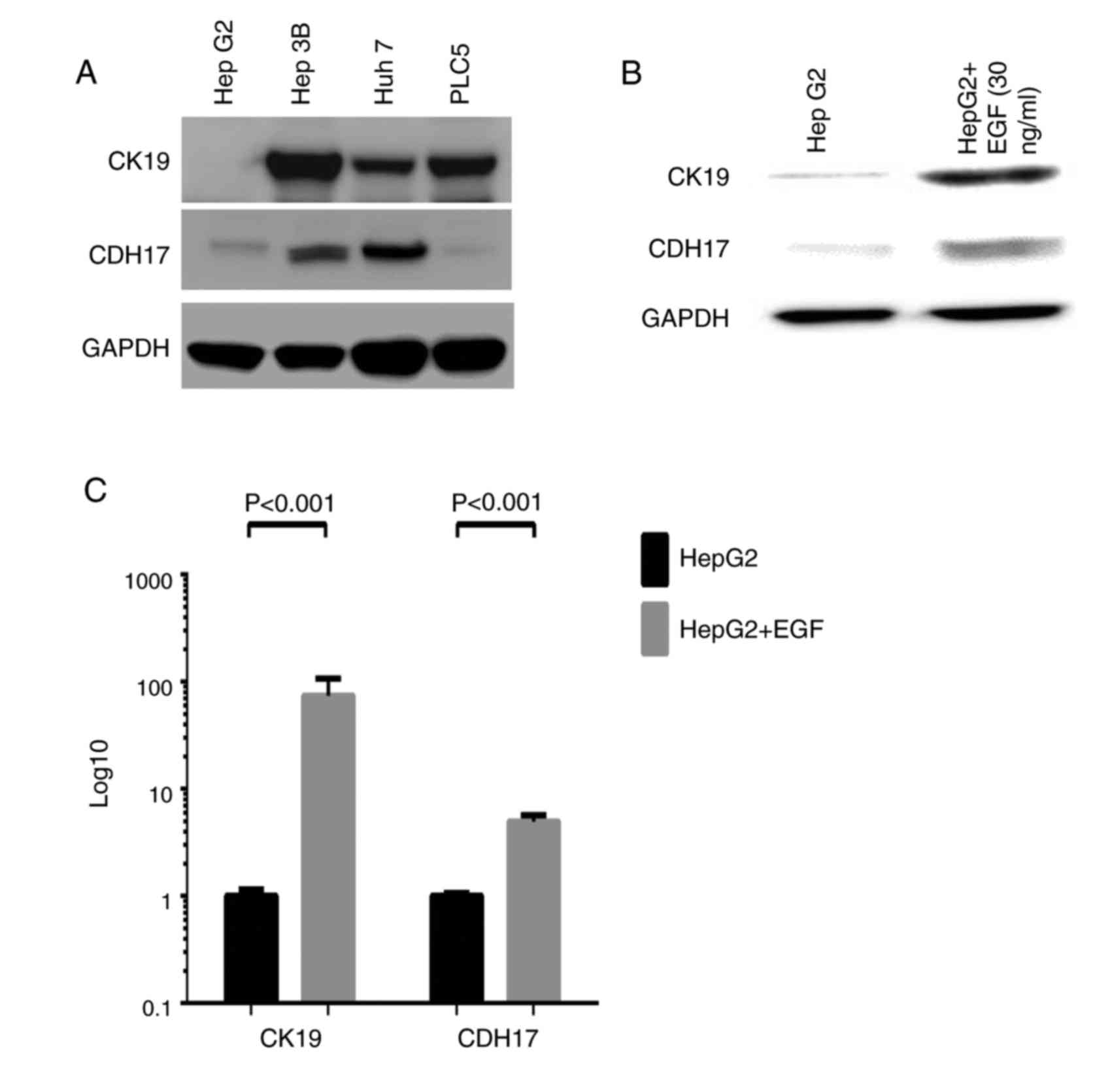 | Figure 4.(A) Western blot analysis of various
HCC cell lines. Primary antibodies were that of CK19 and CDH17 and
a dilution of 1:100,000 and 1:2,000, respectively, were adopted.
GAPDH was used as internal control. Hep3B, Huh7, and PLC5 were
CK19(+) HCC cell lines, while HepG2 was CK19(−) HCC cell line. On
the other hand, Hep3B and Huh7 were CDH17(+) HCC cell lines, while
HepG2 and PLC5 were CDH17(−) HCC cell lines. (B and C) The study of
EGF-treated HepG2 cells (EGF, 30 ng/ml for 5 days). Western blot
analysis confirmed that CK19 can be induced by EGF treatment. In
the meanwhile, the expression of CDH17 was also enhanced after EGF
treatment (B). Real-time qPCR analysis of EGF-treated HepG2 cells
demonstrated that both CK19 and CDH17 transcripts were
significantly elevated (P<0.001 and <0.001, respectively)
(C). In the other words, EGF can induce both CK19 and CDH17
expressions. HCC, hepatocellular carcinoma; CK19, cytokeratin 19;
CDH17, cadherin 17; GAPDH, glyceraldehyde-3-phosphate
dehydrogenase; EGF, epidermal growth factor. |
Discussion
CK19 is generally believed to be a marker for
biliary epithelial cells. Tumor cells from HCC, as a result, should
not express CK19 since they are supposed to originate from
hepatocytes (16). However, previous
studies also showed that about 10% of HCC with typical microscopic
histologic features expressed CK19 (4,6). These
CK19(+) HCC was found to behave more aggressively and had a worse
outcome (4,6–8,17). For example, Takano et al
demonstrated that CK19(+) HCC exhibited higher invasiveness,
metastatic potential, and poorer prognosis (17). Our previous study also illustrated
that CK19 expression in primary liver tumor was associated with
LNM, tumor non-encapsulation, and worse OS (4). The current study verified that CK19
expression in HCC was associated with LNM, poorer DFS, and worse
OS. Due to distinct clinical behavior and poor outcome, CK19(+) HCC
may be a special subtype of HCC that deserves further
investigation. Unfortunately, few studies to date had tried to
dissect the possible mechanism responsible for poor prognosis in
CK19(+) HCC. A previous research indicated that the activation of
the EGF-epidermal growth factor receptor (EGFR) signaling pathway
was associated with the development of CK19-positive HCC, and the
EGF-induced increase in growth abilities of HCC might account for
the poor prognosis of the patients (7). A recent study identified that the poor
clinical outcome of CK19(+) HCC may be attributed to the effect of
CK19 on angiogenesis-related molecules such as vasohibin-1 (VASH1)
and fibroblast growth factor 1 (FGFR1) (17). All of these studies attempt to unravel
the molecular mechanism underlying CK19(+) HCC, and once the
mechanism is identified and explored, a targeted therapy can be
developed to deal with this subset of HCC.
In the current study, we identified that the
expression of CDH17 was significantly associated with that of CK19
at both transcription and translation levels in HBV-HCC. Previous
study has shown that CDH17 could be a biomarker for gastric
carcinoma and attractive therapeutic target for this aggressive
malignancy (18). Recent reports also
demonstrated that the expression of CDH17 in HCC was associated
with vascular invasion, tumor metastasis, advanced tumor stage, and
poor prognosis (12,13,19,20). The
therapeutic significance was determined as well that, by targeting
CDH17, we can inhibit tumor growth in HCC (13,19).
Despite numerous works and reports, however, no study to date has
dealt with the involvement of CDH17 in CK19(+) HCC. Our study is by
far the first one to explore the relationship between CK19 and
CDH17 in HBV-HCC.
The present study demonstrated that CDH17 expression
was one of the most significant poor prognostic factors for DFS in
HBV-HCC. The CDH17(+) HCC patients is expected to have tumor
relapse within 9 months after the operation. For patients who were
treated with curative hepatectomy, early recurrence was proved to
be a poor prognostic factor for OS (21). In addition, CDH17 expression was
associated with LNM and a likelihood of vascular invasion in HCC.
Both LNM and vascular invasion were well known poor prognostic
factors for DFS and OS after hepatectomy (11). Our study, as a result, agreed with
previous reports that CDH17 expression was a poor prognostic factor
for HCC after hepatectomy. Given substantial correlation between
CK19 and CDH17 expressions, we believe that the high recurrence
rate and poor prognosis of CK19(+) HCC may be attributed to CDH17
expression. Since CDH17 has been reported to influence HCC outcome
by targeting Wnt/β-catenin pathway, anti-CDH17 Ab or inhibitors of
Wnt/β-catenin pathway may have promising effects for CK19(+) HCC
(18–20).
In an attempt to dissect the causal relationship
between CK19 and CDH17, we conducted in vitro studies and
confirmed that CK19 can be induced by EGF treatment. In addition to
CK19, CDH17 was also induced upon EGF stimulation. Therefore, we
believe that in CK19(+) HCC, EGF/EGFR may act as an initiator that
induce the expression of both CK19 and CDH17, resulting in worst
prognosis. EGF/EGFR is responsible for a variety of cellular
functions and pathologic processes including cell cycle
progression, gene transcription, cell proliferation, migration, and
adhesion (22,23). The exact mechanism by which EGF/EGFR
influences CK19 and CDH17 expressions mandates further
investigations. Last but not the least, by establishing a stable
CDH17 transfectant in HepG2, we found in the current study that the
expression of CK19 was enhanced by CDH17 over-expression. CK19, as
a result, was regulated by CDH17 in HCC. Our novel findings
explains the significant association between CDH17 and CK19 in
HBV-HCC, and we believe that the poor prognosis of CK19(+) HCC is
partly attributed to this causal relationship. The current study,
subsequently, should be the first one in the English literature to
identify this EGF/EGFR-CDH17-CK19 pathway in HCC. Treatment
targeted against EGF/EGFR or CDH17 may thus be beneficial for
CK19(+) HCC. Further studies are still warranted to validate our
findings and to explore the detailed mechanistic relationships
between these molecules.
In conclusion, our study demonstrated that CK19(+)
HCC was significantly associated with LNM and a worse survival. The
expression of CDH17 was significantly associated with that of CK19
in HBV-HCC. CDH17, a gene known to be associated with vascular
invasion, tumor metastasis, and advanced tumor stage, was found to
have an extremely poor DFS in the current study. As a result, we
believe that in CK19(+) HCC, CDH17 plays an important role in
promoting tumor recurrence and leading to poor prognosis. Lastly,
we found that EGF can induce the expressions of both CK19 and
CDH17, and CDH17 in turn can enhance the expression of CK19 in HCC.
Novel therapeutics by targeting EGF/EGFR or CDH17 may thus be
beneficial for CK19(+) HCC. Further study is warranted to determine
the detailed mechanistic relationships between these molecules.
Acknowledgements
We are grateful to all our colleagues in the
Department of Cancer Center, Department of Pathology, the Genomic
Medicine Research Core Laboratory of Chang Gung Memorial Hospital,
and Graduate Institute of Clinical Medical Sciences, Chang Gung
University for their technical assistance. We are also grateful to
Chun-Hsing Wu, Shu-Chuan Yu, and Jo-Chu Chiu for their laboratory
assistance. This study was supported by Chang Gung Memorial
Hospital (CMRPG3G0051) and Ministry of Science and Technology,
Taiwan, R.O.C. (NMRPG3F0321).
Glossary
Abbreviations
Abbreviations:
|
AFP
|
α-fetoprotein
|
|
AJCC
|
American Joint Committee on Cancer
|
|
CDH17
|
cadherin 17
|
|
CEA
|
carcinoembryonic antigen
|
|
CK19
|
cytokeratin 19
|
|
CT
|
computed tomorgraphy
|
|
DFS
|
disease-free survival
|
|
EGF
|
epidermal growth factor
|
|
EGFR
|
epidermal growth factor receptor
|
|
HBV
|
hepatitis B virus
|
|
HCC
|
hepatocellular carcinoma
|
|
HCV
|
hepatitis C virus
|
|
ICG-15
|
indocyanine green retention at 15
min
|
|
IHC
|
immunohistochemistry
|
|
LNM
|
lymph node metastasis
|
|
OS
|
overall survival
|
|
qRT-PCR
|
quantitative real-time PCR
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sartorius K, Sartorius B, Aldous C,
Govender PS and Madiba TE: Global and country underestimation of
hepatocellular carcinoma (HCC) in 2012 and its implications. Cancer
Epidemiol. 39:284–290. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ministry of Health and Welfare. Executive
Yuan, R.O.C: Report of leading cancer-related death in 2014.
2015.
|
|
4
|
Lee CW, Kuo WL, Yu MC, Chen TC, Tsai CN,
Lee WC and Chen MF: The expression of cytokeratin 19 in lymph nodes
was a poor prognostic factor for hepatocellular carcinoma after
hepatic resection. World J Surg Oncol. 11:1362013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Corcelle V, Stieger B, Gjinovci A,
Wollheim CB and Gauthier BR: Characterization of two distinct liver
progenitor cell subpopulations of hematopoietic and hepatic
origins. Exp Cell Res. 312:2826–2836. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamamoto T, Uenishi T, Ogawa M, Ichikawa
T, Hai S, Sakabe K, Tanaka S, Kato H, Mikami S, Ikebe T, et al:
Immunohistologic attempt to find carcinogenesis from hepatic
progenitor cell in hepatocellular carcinoma. Dig Surg. 22:364–370.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yoneda N, Sato Y, Kitao A, Ikeda H,
Sawada-Kitamura S, Miyakoshi M, Harada K, Sasaki M, Matsui O and
Nakanuma Y: Epidermal growth factor induces cytokeratin 19
expression accompanied by increased growth abilities in human
hepatocellular carcinoma. Lab Invest. 91:262–272. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hoshida Y, Toffanin S, Lachenmayer A,
Villanueva A, Minguez B and Llovet JM: Molecular classification and
novel targets in hepatocellular carcinoma: Recent advancements.
Semin Liver Dis. 30:35–51. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Uenishi T, Hirohashi K, Shuto T, Kubo S,
Tanaka H, Sakata C, Ikebe T and Kinoshita H: The clinical
significance of lymph node metastases in patients undergoing
surgery for hepatocellular carcinoma. Surg Today. 30:892–895. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chu KM, Lai EC, Al-Hadeedi S, Arcilla CE
Jr, Lo CM, Liu CL, Fan ST and Wong J: Intrahepatic
cholangiocarcinoma. World J Surg. 21:301–305; discussion 305–306.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee CW, Chan KM, Lee CF, Yu MC, Lee WC, Wu
TJ and Chen MF: Hepatic resection for hepatocellular carcinoma with
lymph node metastasis: Clinicopathological analysis and survival
outcome. Asian J Surg. 34:53–62. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ding ZB, Shi YH, Zhou J, Shi GM, Ke AW,
Qiu SJ, Wang XY, Dai Z, Xu Y and Fan J: Liver-intestine cadherin
predicts microvascular invasion and poor prognosis of hepatitis B
virus-positive hepatocellular carcinoma. Cancer. 115:4753–4765.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee NP, Poon RT, Shek FH, Ng IO and Luk
JM: Role of cadherin-17 in oncogenesis and potential therapeutic
implications in hepatocellular carcinoma. Biochim Biophys Acta.
1806:138–145. 2010.PubMed/NCBI
|
|
14
|
International Union Against Cancer (UICC),
. TNM Classification of Malignant Tumours. Sobin LH, Gospodarowicz
MK and Wittekind C: 7th. Wiley-Blackwell; Hoboken, NJ: 2009
|
|
15
|
Yu MC, Lee YS, Lin SE, Wu HY, Chen TC, Lee
WC, Chen MF and Tsai CN: Recurrence and poor prognosis following
resection of small hepatitis B-related hepatocellular carcinoma
lesions are associated with aberrant tumor expression profiles of
glypican 3 and osteopontin. Ann Surg Oncol. 3 Suppl 19:S455–S463.
2012. View Article : Google Scholar
|
|
16
|
Libbrecht L, Desmet V, Van Damme B and
Roskams T: The immunohistochemical phenotype of dysplastic foci in
human liver: Correlation with putative progenitor cells. J Hepatol.
33:76–84. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Takano M, Shimada K, Fujii T, Morita K,
Takeda M, Nakajima Y, Nonomura A, Konishi N and Obayashi C: Keratin
19 as a key molecule in progression of human hepatocellular
carcinomas through invasion and angiogenesis. BMC Cancer.
16:9032016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qiu HB, Zhang LY, Ren C, Zeng ZL, Wu WJ,
Luo HY, Zhou ZW and Xu RH: Targeting CDH17 suppresses tumor
progression in gastric cancer by downregulating Wnt/β-catenin
signaling. PLoS One. 8:e569592013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liu LX, Lee NP, Chan VW, Xue W, Zender L,
Zhang C, Mao M, Dai H, Wang XL, Xu MZ, et al: Targeting cadherin-17
inactivates Wnt signaling and inhibits tumor growth in liver
carcinoma. Hepatology. 50:1453–1463. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang Y, Shek FH, Wong KF, Liu LX, Zhang
XQ, Yuan Y, Khin E, Hu MY, Wang JH, Poon RT, et al:
Anti-cadherin-17 antibody modulates beta-catenin signaling and
tumorigenicity of hepatocellular carcinoma. PLoS One. 8:e723862013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamamoto Y, Ikoma H, Morimura R, Konishi
H, Murayama Y, Komatsu S, Shiozaki A, Kuriu Y, Kubota T, Nakanishi
M, et al: Optimal duration of the early and late recurrence of
hepatocellular carcinoma after hepatectomy. World J Gastroenterol.
21:1207–1215. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Seshacharyulu P, Ponnusamy MP, Haridas D,
Jain M, Ganti AK and Batra SK: Targeting the EGFR signaling pathway
in cancer therapy. Expert Opin Ther Targets. 16:15–31. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Blobel CP: ADAMs: Key components in EGFR
signalling and development. Nat Rev Mol Cell Biol. 6:32–43. 2005.
View Article : Google Scholar : PubMed/NCBI
|