Introduction
Bladder cancer is the fourth most common tumor among
males in the United States of America (1). The most frequent symptom of bladder
cancer is hematuria, whilst urgency, dysuria and bladder irritation
indicate muscle-invasive bladder tumors or carcinoma in situ
(cis) (2). A problem for the
diagnosis of bladder cancer is that patients with stage
Ta or T1 disease may not manifest any of
these symptoms (1–3).
Numerous patients with bladder diseases may exhibit
a complex of symptoms known as overactive bladder (OAB),
characterized by urgency, frequency and nocturia, with or without
urinary incontinence (4). It was
reported that metastatic breast cancer was also associated with
OAB-like symptoms (4,5). Whether these symptoms are associated
with molecular features or with prognosis of bladder cancer remains
unclear. These data may be beneficial for understanding the onset
and progression of bladder cancer.
Antagonists of muscarinic acetylcholine receptors
(mAChRs) remain the first-line therapy for treating OAB symptoms,
such as urgency (6). Understanding
the role of mAChRs in OAB requires the examination of all five
receptor subtypes (M1R-M5R), all of which being located in the
urothelium (4). The urothelium could
respond to muscarinic agonist stimulation by self-releasing
acetylcholine (ACh), which may modulate afferent activity in turn
(7). The urothelium assists in
filling and distension of the bladder, and it protects the
underlying stroma (8). Of non-muscle
invasive bladder cancer, ~70% were confined to the urothelium
(5).
Muscarinic cholinergic receptor 3 (M3R) is one of
the major receptors associated with micturition in normal human
bladder and OAB (9); however, M3R
transcripts have not been detected in the J82, RT4, T24 and 5,637
urothelial cancer cell lines (10).
Recently, a study also determined that M3R expression was decreased
in the bladder cancer group, compared with non-cancer control
individuals (9). Nevertheless, the
clinical features were not mentioned in these studies, and invasive
bladder cancer was not focused on (9,10).
MAChRs are expressed in several tumor types,
including colon, ovary, lung, breast and prostate cancer, and the
genes encoding M1R and M3R have been demonstrated to function as
conditional oncogenes (11),
activating downstream phosphatidylinositol hydrolysis to induce
cell proliferation (12). In addition
to clarifying the potential role of MAChRs in bladder cancer,
studies are required to explore the potential role of muscarinic
cholinergic signaling. Such signaling serves an important role in
colon cancer (13), but whether it
also participates in bladder cancer is unclear. This signaling can
be partially measured via assays for several enzymes involved in
auto- and paracrine signaling, including acetylcholinesterase
(AChE), butyrylcholinesterase and choline acetyltransferase (ChAT)
(14). Muscarinic signaling in the
urothelium also contributes to OAB-like symptoms (4,15).
To begin to address these gaps in the literature,
data that had been prospectively entered into a multicenter
database, of patients with invasive bladder cancer in China, were
retrospectively analyzed. Possible associations between OAB-like
symptoms and muscarinic cholinergic signaling were examined using
this data.
Patients and methods
Study design and ethical approval
A multicenter database between January 2010 to
December 2015 was established at the Tumor Hospital of Guangxi
Medical University (Nanning, China), Nanfang Hospital of Southern
Medical University (Guangzhou, China) and Guangzhou First People's
Hospital (Guangzhou, China), containing medical records of patients
with OAB, suspected or diagnosed bladder tumors since 2010. The
patients written informed consent were obtained at the time of data
collection. The mean age was 58.2 (7–85) years, 203 were male and
71 were female. The present study was approved by the ethics
committee of institutes aforementioned. Information on OAB-like
symptoms were recorded prospectively in this database, after which
the patients underwent bladder biopsy, transurethral resection or
radical cystectomy. Overall OAB symptom severity was assessed using
the OAB symptom score (OABSS) (15).
Investigators collected symptom data prior to definitive diagnosis
or pathology results became available.
Inclusion criteria and exclusion
criteria
Patients in the database who were confirmed to have
bladder tumors based on bladder biopsy, transurethral resection or
radical cystectomy between January 2010 and December 2015 were
eligible. Patients were excluded from the study if they had
previously been diagnosed with OAB or interstitial cystitis or if
they had a history of severe urinary system infection, pelvic
radiotherapy and sexually transmitted diseases.
Clinical outcomes
Outcomes were time to recurrence, progression free
survival (PFS) and overall survival. Time to recurrence and PFS
were calculated as the date from radical cystectomy to the first
documented recurrence. A single patient was diagnosed with cis, a
type of superficial bladder tumor which is not muscle-invasive, and
was not included in the PFS observation.
Reverse transcription-polymerase chain
reaction (RT-PCR) analysis of MAChRs M1R-M5R
Bladder mucosa specimens were obtained by cystoscopy
from 10 patients with OAB, and total RNA was extracted using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc., Waltham, MA, USA), according to the manufacturer's
instructions. Expression levels of M1R-M5R transcripts were
determined by RT-PCR as previously described (16). Total RNA (1.5 µg) was reverse
transcribed for 60 min at 37°C using random primers from the M-MLV
First Strand kit (Invitrogen; Thermo Fisher Scientific, Inc.). PCR
amplification was performed for 2 min at 50°C, then 10 min at 95°C,
followed by 45 cycles of 15 sec at 95°C and 60 sec at 58°C.
Histopathology and
immunohistochemistry against M1R-M5R
Polyclonal antibodies against M1R-M5R were purchased
from Abcam (Cambridge, UK), and DAB substrate liquid was obtained
from Sigma-Aldrich (Merck KGaA, Darmstadt, Germany). A total of 4
µm-thick sections from tumor tissue and tumor-adjacent tissue were
embedded in paraffin, fixed in 4% paraformaldehyde for 24 h at room
temperature, deparaffinized, subjected to antigen retrieval
(citrate buffer for 30 min at 100°C; rehydration in a descending
ethanol series at 100, 95, 85 and 75% for 10 min), incubated with
3% hydrogen peroxide for 10 min at room temperature and mounted on
slides. Slides were incubated with rabbit antibodies to CHRM1
(1:1,000; Abcam; cat. no. ab180636), CHRM2 (1:500; Abcam; cat. no.
ab188891), CHRM3 (1:100; Abcam, ab150480), CHRM4 (1:1,000; Abcam,
ab150518), CHRM5 antibody (1:1,000; Abcam; cat. no. ab150531)
overnight at 4°C. The following day, these tissues were washed with
PBS three times, and goat anti-rabbit immunoglobulin G horseradish
peroxidase-conjugated (1:1,000; cat. no. HA1001; HuaBio Inc.,
Cambridge, MA, USA) secondary antibody incubated for 1 h at room
temperature. DAB substrate liquid was used for the slides and
visualized under a light microscope (magnification, ×100; cat. no.
CX31-LV320; Olympus Corporation, Tokyo, Japan).
Serum levels of cholinesterase
(ChE)
After patients had been hospitalized for 2 days,
venous blood (2 ml) was collected on an empty stomach, serum was
isolated by centrifugation for 10 min at 1,509 × g at room
temperature. Levels of ChE in serum were assayed using the
cholinesterase kit (CUSABIO, Wuhan, China) and conducted according
to the manufacturer's protocol.
Statistical analysis
Data were plotted using GraphPad Prism 5 (GraphPad
Software, Inc., La Jolla, CA, USA) and presented as the mean ± the
standard deviation. Statistical tests were applied within SPSS 21
(IBM Corp., Armonk, NY, USA). P<0.05 was considered to indicate
a statistically significant difference, and all reported P-values
were two-sided. Differences between patient groups were assessed
for significance using Student's t-test, including comparing serum
levels of ChE and baseline information. Differences in M1R-M5R
expression between muscle-invasive non-muscle-invasive bladder
cancer were analyzed using one-way analysis of variance followed by
the Student-Newman-Keuls post hoc test. When assessing differences
in skewed data using multiple comparisons, the non-parametric test
was used. For Table II,
Kruskal-Wallis test was used to compare three groups, whilst the
Mann-Whitney U test was used to compare two groups.
 | Table II.Differences in overactive
bladder-like symptoms between benign tumor, invasive and
non-invasive bladder cancer. |
Table II.
Differences in overactive
bladder-like symptoms between benign tumor, invasive and
non-invasive bladder cancer.
| Factor | Benigna (n=11) | Non-invasive
(n=55) | Invasive
(n=62) | P-value |
|---|
| No. urgency
(%) |
|
|
| 0.0017b |
| No
urgency | 2 (18.18) | 29 (52.73) | 15 (24.19) |
|
|
Urgency≥1/week | 1 (9.09) | 2 (3.64) | 3 (4.84) |
|
|
Urgency=1/day | 2 (18.18) | 4 (7.27) | 4 (6.45) |
|
|
Urgency=2-4/day | 2 (18.18) | 11 (20) | 15 (24.19) |
|
|
Urgency≥5/day | 4 (36.36) | 9 (16.36) | 25 (40.32) |
|
| No. daytime
frequency (%) |
|
|
| 0.0322b |
| ≤7 | 3 (27.27) | 28 (50.91) | 23 (37.10) |
|
|
8–14 | 5 (45.45) | 24 (43.64) | 23 (37.10) |
|
|
≥15 | 3 (27.27) | 3 (5.45) | 16 (25.81) |
|
| No. nighttime
frequency (%) |
|
|
| 0.0001b |
| 0 | 2 (18.18) | 4 (7.27) | 2 (3.23) |
|
| 1 | 1 (9.09) | 12 (21.82) | 2 (3.23) |
|
| 2 | 4 (36.36) | 18 (32.73) | 12 (19.35) |
|
| ≥3 | 4 (36.36) | 21 (38.19) | 46 (74.19) |
|
| No. OABSS (%) |
|
|
| 0.0016b |
|
Urgency<2 | 0 (0) | 29 (52.73) | 15 (24.19) |
|
|
Mild | 6 (54.55) | 4 (7.27) | 3 (4.84) |
|
|
Moderate | 2 (18.18) | 18 (32.73) | 33 (53.23) |
|
|
|
Factor | Non-muscle-invasive
(n=55) | Muscle-invasive
(n=62) |
|
|
|
| No. urgency
(%) |
|
|
| 0.0005c |
| No
urgency | 29 (52.70) | 15 (24.20) |
|
|
|
Urgency≥1/week | 2 (3.60) | 3 (4.80) |
|
|
|
Urgency=1/day | 4 (7.30) | 4 (6.50) |
|
|
|
Urgency=2-4/day | 11 (20) | 15 (24.20) |
|
|
|
Urgency≥5/day | 9 (16.40) | 25 (40.30) |
|
|
| No. daytime
frequency (%) |
|
|
| 0.0198b |
| ≤7 | 28 (50.90) | 23 (37.10) |
|
|
|
8–14 | 24 (43.60) | 23 (37.10) |
|
|
|
≥15 | 3 (5.50) | 16 (25.80) |
|
|
| No. nighttime
frequency (%) |
|
|
|
<0.0001b |
| 0 | 4 (7.30) | 2 (3.20) |
|
|
| 1 | 12 (21.80) | 2 (3.20) |
|
|
| 2 | 18 (32.70) | 12 (19.40) |
|
|
| ≥3 | 21 (38.20) | 46 (74.20) |
|
|
| No. OABSS (%) |
|
|
| 0.0191b |
|
Urgency<2 | 29 (52.70) | 15 (24.20) |
|
|
|
Mild | 4 (7.30) | 3 (4.80) |
|
|
|
Moderate | 18 (32.70) | 33 (53.20) |
|
|
|
Severe | 4 (7.30) | 11 (17.70) |
|
|
Among 26 patients who underwent radical cystectomy,
PFS was estimated using Kaplan-Meier plots with a log rank test and
multivariate Cox proportional hazards regression.
Results
Differences in OAB-like symptoms
between muscle-invasive and non-muscle-invasive bladder
cancers
The 228 patients included in the retrospective
analysis were classified as having invasive or non-invasive bladder
cancer (Table I). Incidence and
severity of OAB-like symptoms, including urgency, daytime frequency
and nocturia was higher in the invasive group, compared with the
non-invasive group (Table II). The
OAB-like symptoms in patients with malignant tumors were more
severe, compared with those with benign tumors (P=0.00001; Table II).
| Table I.Baseline characteristics of 228
Chinese patients with bladder tumor. |
Table I.
Baseline characteristics of 228
Chinese patients with bladder tumor.
| Variable | Valuea |
|---|
| Age, years |
|
| Mean ±
SE | 0.5±13.53 |
|
Median | 61 |
|
Interquartile range | 50–71 |
| Sex |
|
|
Male | 181 (79.4) |
|
Female | 47 (20.6) |
| Previous
operation |
|
| No | 154 (67.5) |
|
TUR | 45 (19.7) |
| Open
(partial cystectomy) | 29 (12.7) |
| Previous
intravesical instillation |
|
| No | 183 (80.3) |
|
Yes | 45 (19.7) |
| Total bladder
cancer (n=206) |
|
|
Non-muscle-invasive | 109 (47.8) |
|
Muscle-invasive | 97 (42.5) |
| Total bladder
cancer (n=206) |
|
|
Non-invasive | 63 (30.6) |
|
Invasive | 143 (69.4) |
| Grade of bladder
cancer (WHO 2004, n=199) |
|
|
PUNLMP | 10 (4.4) |
|
Low-grade | 90 (39.5) |
|
High-grade | 99 (43.4) |
| N stage of bladder
cancer (n=206) |
|
| N0 | 175 (76.7) |
| N1 | 19 (8.3) |
| N2 | 8 (3.5) |
| N3 | 4 (1.8) |
| Metastasis of
bladder cancer (n=206) |
|
| No | 198 (86.8) |
|
Yes | 8 (3.5) |
| Pathology |
|
| PUNLMP | 9 (3.9) |
| Ta | 54 (23.7) |
| T1 | 41 (18.0) |
|
T2a | 34 (14.9) |
|
T2b | 19 (8.3) |
|
T3a | 14 (6.1) |
|
T3b | 13 (5.7) |
|
T4a | 11 (4.8) |
|
T4b | 10 (4.4) |
|
Tis | 1 (0.4) |
| Benign
tumorb | 22 (9.6) |
The core symptom of OAB is urgency (4). Among 26 patients who underwent radical
cystectomy, those experiencing ‘daily ≥1’ urgency indicated lower
PFS, compared with those with less severe urgency (P=0.04962;
Fig. 1A). Cox regression identified
urgency as an independent predictor of PFS following radical
cystectomy.
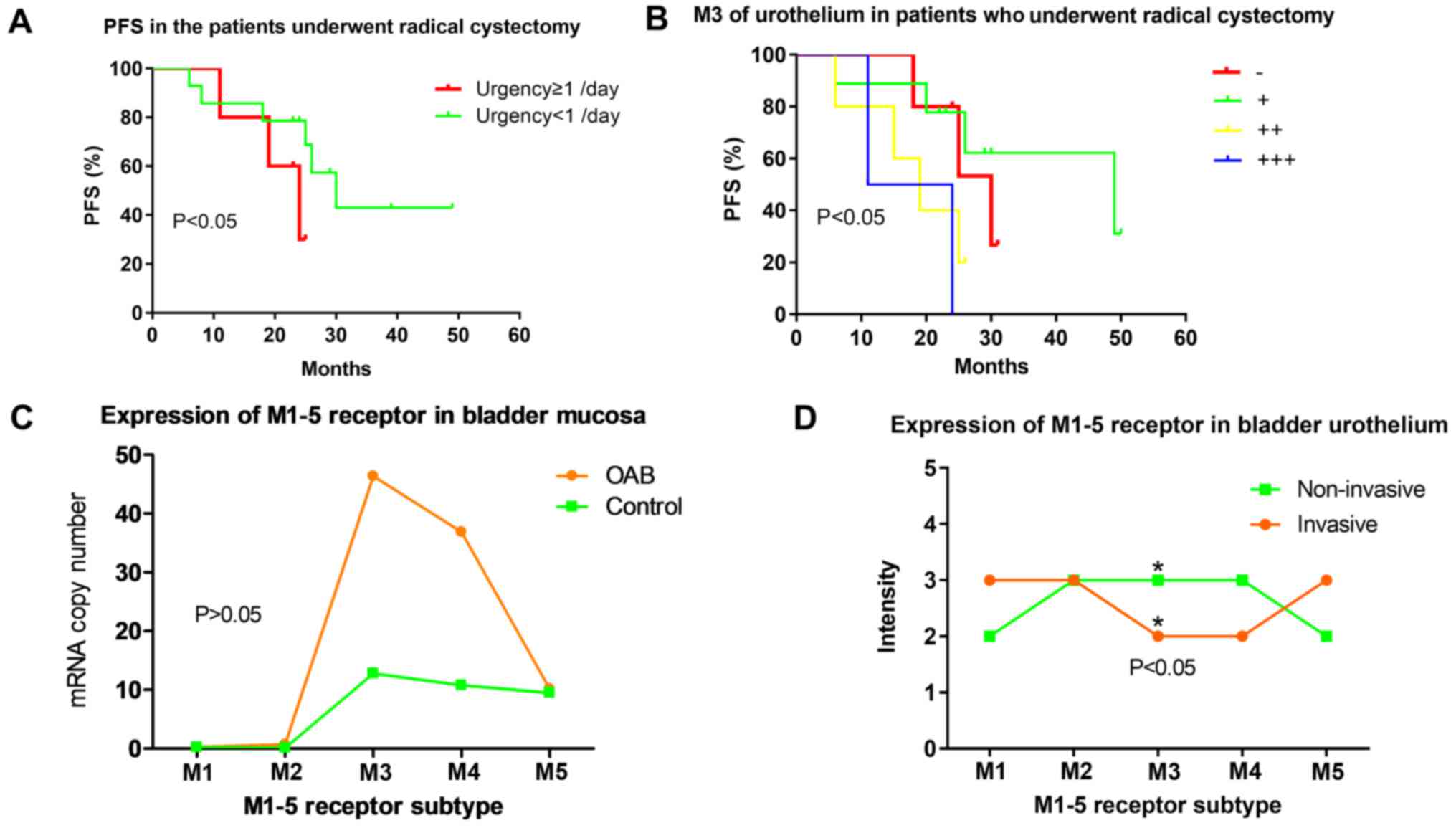 | Figure 1.Expression of M1-5R of urothelium in
OAB and bladder cancer and urgency in PFS. (A) Patients
experiencing ‘daily ≥1’ urgency demonstrated significantly lower
PFS, compared with those experiencing ‘daily <1’ (P=0.0496). (B)
PFS in patients with invasive bladder cancer who underwent radical
cystectomy. M3R expression was negatively associated with PFS
(P=0.032). (C) Expression levels of mAChRs M1-5R in bladder mucosa
of patients with OAB based on reverse transcription-polymerase
chain reaction. (OAB group, M1-5, n=10, 9, 10, 10, 10; Control
group, M1-5, n=11, 9, 11, 11, 11; P=0.56, 0.22, 0.56, 0.43, 0.92).
(D) M1-5R proteins in bladder urothelium of patients with bladder
cancer based on immunohistochemistry. M3R staining (*P<0.05) was
less intense in patients with muscle-invasive bladder cancer, even
though this group had more severe OAB-like symptoms. PFS,
progression free survival; M1-5R, muscarinic cholinergic receptor
1–5; OAB, overactive bladder. |
M3R expression in urothelium and PFS
in patients undergoing radical cystectomy
M3R expression was also observed in PFS study.
Higher M3R expression in the urothelium of the 26 patients with
muscle-invasive bladder cancer who underwent radical resection was
associated with reduced PFS [χ2=8.811, degrees of
freedom (df)=3, P=0.032; Fig. 1B].
Similar results were obtained when M3R expression in the
sub-urothelium was analyzed (χ2=11.651, df=3,
P=0.009).
Differences in M1R-M5R expression
between muscle-invasive and non-muscle-invasive bladder
cancers
Expression levels of M3R transcript in bladder
mucosa was significantly higher in patients with OAB, compared with
the normal group (P=0.00088; Fig.
1C). Among patients with bladder cancer, M3R staining intensity
in immunostained bladder urothelium was lower in the
muscle-invasive group, compared with the non-muscle-invasive group
(Fig. 1D). M3R staining intensity in
the sub-urothelium, as well as the mortality rate, was similar
between the two patient subgroups (Data not shown).
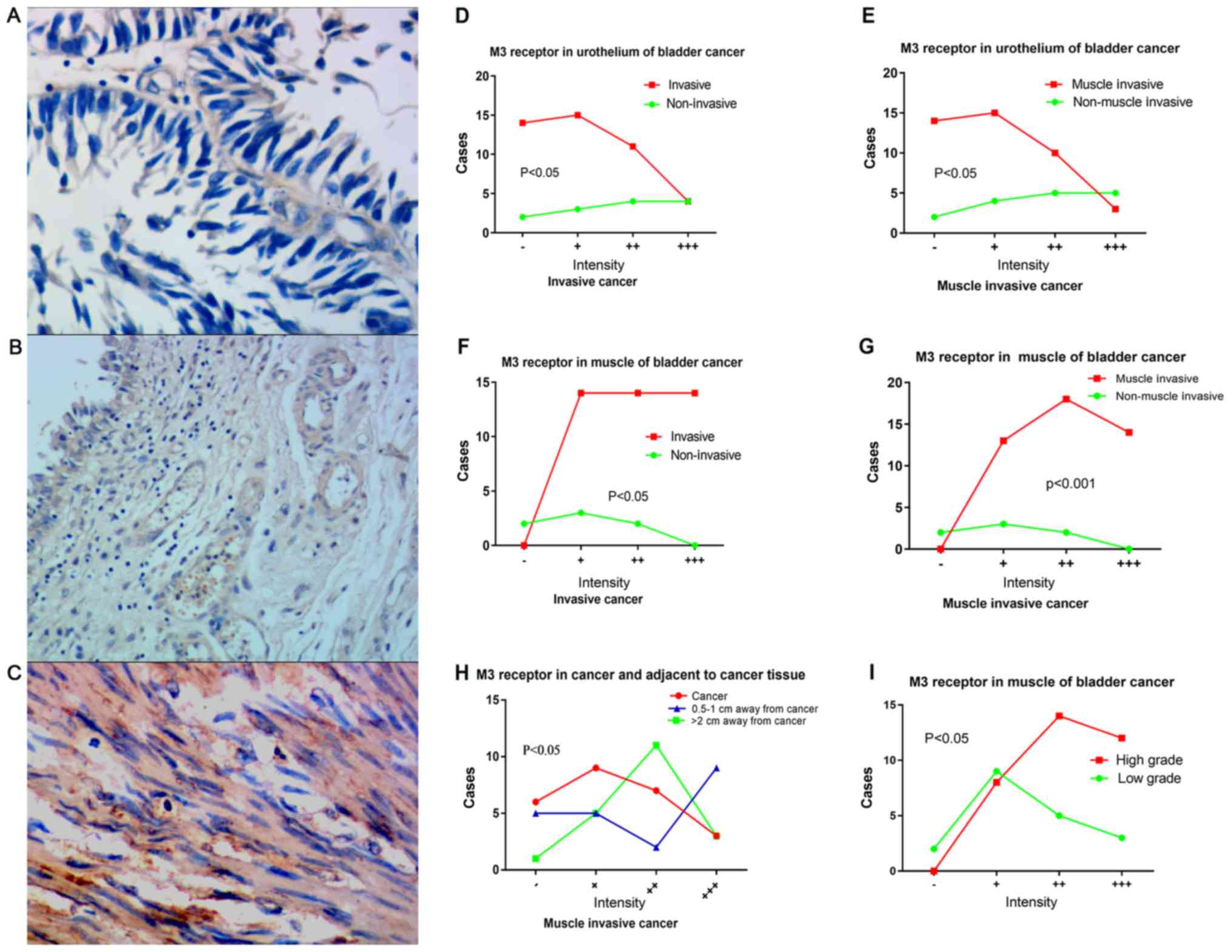
Downregulation of M3R in urothelium of
patients with bladder cancer
M3R expression in bladder urothelium (Fig. 2A), sub-urothelium (Fig. 2B) and detrusor (Fig. 2C) were determined in patients with
bladder cancer. M3R expression in bladder urothelium was lower in
patients with bladder cancer, whether muscle-invasive or invasive,
compared with the non-muscle-invasive or non-invasive group,
respectively (Fig. 2D-G). For
patients with invasive cancer, M3R expression in the urothelium
demonstrated a decreasing gradient in the following order: Adjacent
tissue lying >2 cm from the tumor; adjacent tissue lying 0.5–1
cm from the tumor; tumor tissue (Fig.
2H). M3R expression of detrusor was higher in the
muscle-invasive and invasive groups (Fig.
2I). When patients were classified as low or high-grade,
according to WHO 2004 criteria (17),
M3R expression in detrusor muscle was significantly higher in the
low-grade subgroup (χ2=7.348, P=0.046).
Upregulation of M2R in urothelium of
patients with bladder cancer
Expression levels of M2R in urothelium were
significantly increased in patients with invasive bladder cancer.
In the sub-urothelium, M2R expression was significantly higher in
the invasive group, compared with the non-invasive group
(χ2=10.274, df=3, P=0.016), and significantly higher in
the muscle-invasive group, compared with the non-muscle-invasive
group (χ2=8.289, df=3, P=0.038). Among the 26 patients
who underwent radical cystectomy, the level of M2R expression in
the sub-urothelium negatively associated with PFS
(χ2=14.276, df=3, P=0.003).
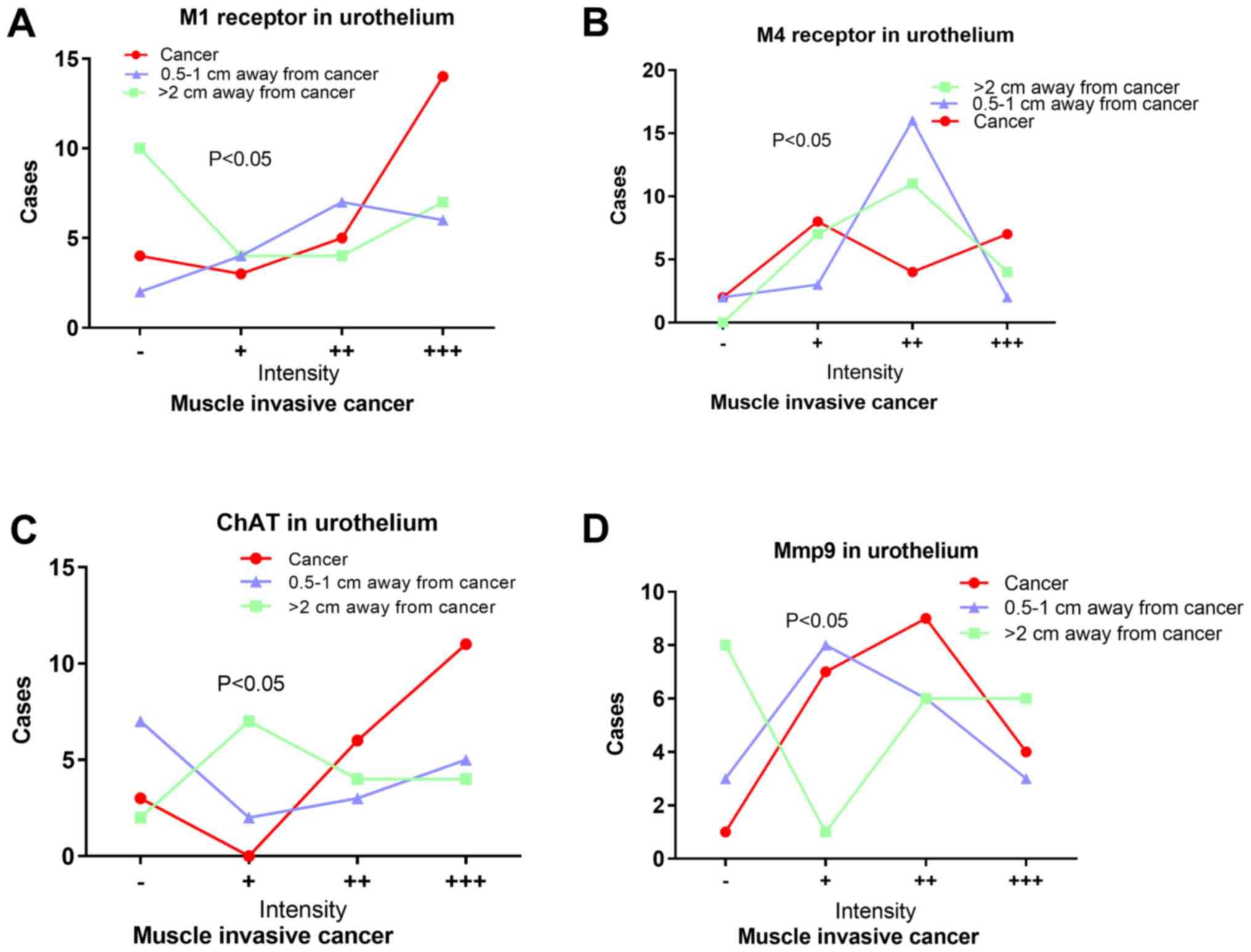
Expression M1R and M4R in patients
with bladder cancer
M1R expression in the sub-urothelium was
significantly higher in the invasive group (χ2=9.151,
P=0.027) and muscle-invasive group (χ2=10.028, P=0.034),
compared with the non-invasive and non-muscle-invasive group. Among
patients with muscle-invasive cancer, M1R expression in urothelium
was significantly lower in tumor, compared with in adjacent tissues
(n=23, χ2=8.982, P=0.01; Fig.
3). In addition, M1R expression in urothelium of patients with
invasive cancer negatively associated with tumor T stage
(χ2=24.73, P=0.029).
M4R expression in the sub-urothelium was
significantly higher in the muscle-invasive group, compared with
the non-muscle-invasive group (χ2=7.770, P=0.049). M4R
expression in invasive sub-urothelial tissue negatively associated
with tumor T stage (χ2=29.472, P=0.009). An increasing
gradient of M4R expression in urothelium also existed in the
following order: Adjacent tissue lying >2 cm from the tumor;
adjacent tissue lying 0.5–1 cm from the tumor; and tumor tissue
(Fig. 3).
Other indicators of cholinergic
signaling in bladder cancer
Serum levels of ChE were significantly lower in
patients with invasive cancer (n=85, 7614.69±2317.75 U/l), compared
with those with non-invasive cancer (n=108, 8570.86±2037.64 U/l)
(t=2.999, P=0.003). Similar results were obtained when patients
with muscle-invasive and non-muscle-invasive cancer (t=2.955,
P=0.004), or patients with low and high-grade cancer (t=3.546,
P=0.001) were compared.
AChE levels in urothelium and sub-urothelium were
similar between patients with invasive or non-invasive cancer.
Among those patients with muscle-invasive cancer who underwent
radical cystectomy, AChE expression levels in the urothelium were
positively associated with PFS. Expression levels of AChE within
the detrusor demonstrated a negative gradient: Adjacent tissue
lying >2 cm from the tumor; tumor tissue; adjacent tissue lying
0.5–1 cm from the tumor (χ2=8.486, df=2, P=0.014).
Among muscle-invasive cancer tissues, rate of ChAT
expression based on immunostaining of urothelium indicated a
negative gradient: Tumor tissue; adjacent tissue lying >2 cm
from the tumor; adjacent tissue lying 0.5–1 cm from the tumor.
Furthermore, the expression of matrix metalloproteinase-9 (MMP-9)
in urothelium demonstrated an increasing gradient in the following
order: Adjacent tissue lying >2 cm from the tumor; adjacent
tissue lying 0.5–1 cm from the tumor; and tumor tissue (Fig. 3).
Discussion
The present study indicated that urgency and other
OAB-like symptoms were more serious in patients with
muscle-invasive bladder cancer than in those with
non-muscle-invasive cancer, based on daytime frequency, nocturia,
urgency and OABSS. Patients with invasive or muscle-invasive cancer
manifested more severe OAB-like symptoms than patients with benign
bladder tumors. The results provided the first evidence that
urgency was more severe in invasive bladder cancer than in
non-invasive cancer, and is associated with reduce prognosis
following radical cystectomy.
Bladder carcinoma invading the detrusor could
produce secondary urgency and frequency. However, it was determined
that the differences existed in invasive or muscle invasive
cancers. This may be because the invasive bladder cancer only
invaded the lamina propria but not the detrusor.
All five subtypes of mAChRs (M1R-M5R) in the patient
tissue were detected, consistent with work in normal urothelium
(4); however, it was determined that
expression of M3R in the urothelium of patients with invasive
bladder cancer was much lower than that of other receptors
(Fig. 1D), consistent with reports of
M3R was decreased in bladder cancer tissues and a gradient of
M1≥M2>M3 in T24 bladder cancer cells (18,19), but
different from a gradient of M3>M4>M5>M2>M1 in a study
of patients with OAB (17). The
current results also contrast with the gradient of
M2>M3=M5>M4=M1 in normal human urothelium (Fig. 1C) (20).
M3R serves an important role in OAB (21). The M3R expression was higher in
bladder mucosa of patients with OAB, compared with the normal group
(17). M3R upregulation was observed
in the detrusor of patients with invasive cancer, and was
associated with the more severe OAB-like symptoms in these
patients, whereas M3R downregulation was observed in the urothelium
of these patients. These results indicated that the mechanisms
leading to OAB-like symptoms may be distinct between OAB and
bladder cancer.
M3R genes are conditional oncogenes (11) frequently expressed in digestive tract
cancer types and considered to serve an important role in
proliferation, differentiation, distant metastasis, transformation
and carcinogenesis (22). They are
considered to serve a key role in the proliferation and metastasis
of cholangiocarcinoma (23), and
their expression is influenced by the extent of differentiation,
distant metastasis and site of cholangiocarcinoma. Whilst several
studies have indicated that M3R upregulation is linked to cancer
processes, others indicate that downregulation is involved
(9,11–13,22,23).
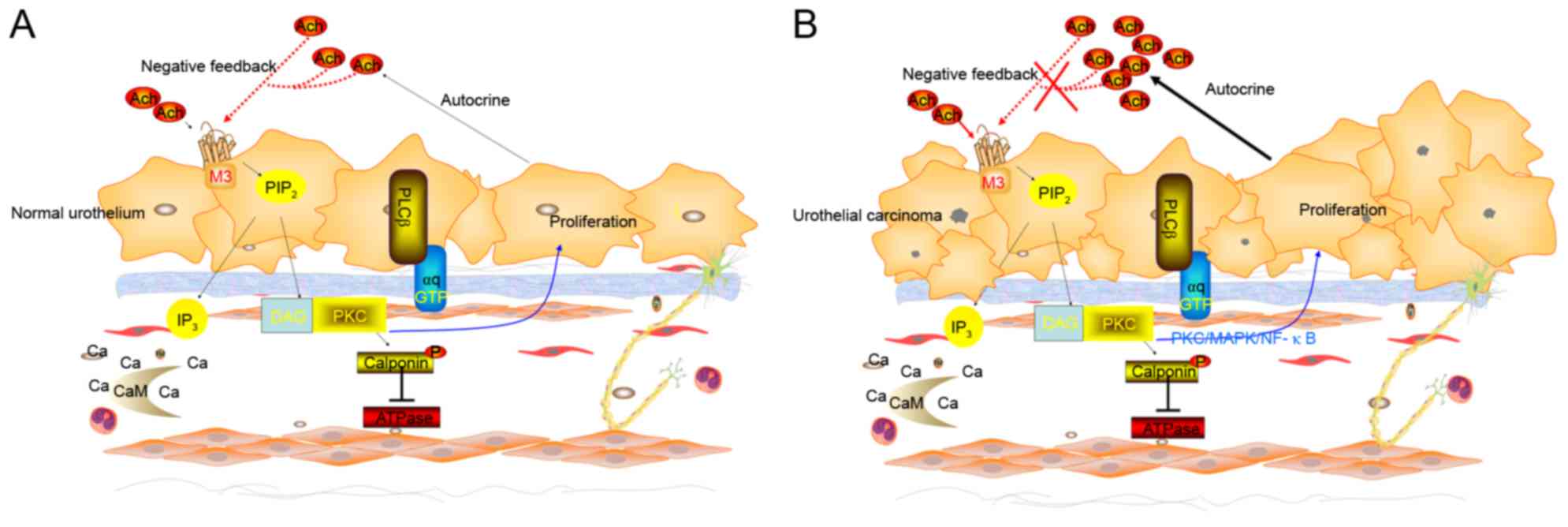
On one hand, M3R activation promotes proliferation,
migration and angiogenesis in several types of cancer cells. It
also promotes proliferation of normal urothelium and of the human
urothelium-derived cell line UROtsa (24), and M3R-selective antagonists inhibit
this effect. On the other hand, knocking down M3R increases
proliferation of UROtsa (10).
Transfecting bladder cancer cell lines such as T24 cells with an
M3R expression plasmid significantly reduces proliferation
(10). These data indicated that
muscarinic M3R may serves a bidirectional regulatory role in normal
urothelial proliferation (Fig. 4A),
and that this regulatory mechanism is altered in bladder cancer
urothelium (10–14) (Fig.
4B).
In the present cohort of patients, M3R appeared to
act primarily as an anti-oncogene. M3R expression was significantly
lower in invasive bladder cancer, compared with non-invasive
cancer, and it was lower in the urothelium of invasive cancer,
compared with tissue adjacent to the tumor. M3R expression
increased with increasing distance from the tumor. In addition, M3R
expression in urothelium negatively associated with PFS in patients
with muscle-invasive cancer who underwent radical cystectomy.
M3R up-regulation promotes the proliferation of
normal bladder detrusor cells (25),
indicating that an observation of M3R expression increased in
bladder cancer detrusor cells should be expected. It was determined
that unlike in the urothelium, M3R expression in the detrusor was
higher in the invasive group, compared with the non-invasive group.
M3R has an established role as oncogene in colon and lung cancer;
however, the present study demonstrated that it may be an
anti-oncogene in urothelium of bladder cancer (7). The results indicated that M3R may serve
different roles in the urothelium and in the detrusor of bladder
cancer. Urgency maybe not just a secondary symptom due to detrusor
invaded.
A previous study determined that mRNA levels of M3R
were significantly upregulated only in low-grade tumor, compared
with normal biopsies tissue, and there were no difference in
high-grade tumors (19). Similar to
this study, the data from the present study also demonstrated that
there were no differences between low-grade and high-grade tumors
in M3R expression.
The results implicated M2R as an anti-oncogene in
bladder cancer. It was determined that M2R expression was highest
in tumor tissue and decreased with increasing distance from the
tumor. It was also higher in the sub-urothelium of patients with
invasive cancer. Among patients who underwent radical bladder
cystectomy, M2R expression associated negatively with PFS. These
results are consistent with study of Pacini et al (19) indicating that M2R helps regulate
bladder cancer proliferation, migration and invasion.
Similar to M2R, the results indicate that M1R and
M4R promote tumorigenesis and progression of bladder cancer. M1R in
sub-urothelium was significantly higher in invasive cancer, and it
was significantly lower in the urothelium of cancer tissue,
compared with adjacent non-cancerous tissue. M1R urothelium and M4R
sub-urothelial expression negatively associated with tumor T stage.
And M4R in sub-urothelium was significantly higher in
muscle-invasive cancer compared with non-muscle-invasive cancer.
Therefore, it was considered that the M1R and M4R also serve an
important role in tumorigenesis and progression of bladder
cancer.
The association of AChE with patient survival and
tumor aggressiveness had been confirmed in brain, lung, head and
neck and hepatocellular cancer (26).
A negative association was determined between ChE levels and PFS in
patients with muscle-invasive cancer who underwent radical bladder
cystectomy. Additionally, ACh interacts with M3R to stimulate
malignant tumor growth in colon tumors (13). In addition, significantly lower
proportions of ChAT-positive cells in the urothelium of
muscle-invasive cancer were determined. This may indicate increased
synthesis of ACh and/or reduced degradation of ACh in cancer
tissue, leading to excessive accumulation of ACh, which promotes
tumor cell proliferation (13,27).
Collectively, these observations indicated that the cholinergic
signaling was over-stimulated in advanced bladder cancer.
Cholinergic signaling may be a novel target to prevent and treat
bladder tumor.
Higher expression of MMP-9 were observed in the
sub-urothelium of muscle-invasive cancer and associated with PFS of
patients who underwent radical cystectomy. These results are
consistent with the hypothesis that MMP-9 acts as a downstream
effector of cholinergic signaling in bladder cancer (28).
The results of the present study should be
interpreted with caution due to several limitations. Although data
were entered prospectively into the patient database, it cannot
exclude that a number of patients with bladder cancer may have had
OAB; however, it is unlikely that the incidence of OAB was high
enough to affect the results. A second limitation is that patients
with OAB-like syndrome were diagnosed using subjective criteria,
including urgency, urinary frequency and nocturia, which may be
interfered with by drink water due to hematuria. Thirdly,
completely normal human bladder urothelium in the experiments were
not used as a control. Future studies should address these
deficiencies in order to verify and extend the data. Additionally,
preoperative clinical staging was performed in a number of
patients, although pathological staging was applied to patients who
underwent radical cystectomy.
The present study demonstrated that M3R expression
was lower in invasive bladder cancer, but it was negatively
associated with PFS. Another possible explanation is that M3R may
serve a more complex biological behavior. Transforming growth
factor-β acts as a tumor suppressor normally, but also function as
a tumor promoter in advanced cancers (29).
In conclusion, the present study indicated that
cholinergic muscarinic signaling is altered in bladder cancer and
is associated with prognosis. Tumorigenesis and development of
bladder cancer appear to involve mAChRs, in particular a change in
the regulatory role of M3R in the urothelium. M3R may act as an
anti-oncogene in bladder cancer, unlike its oncogenic role in
numerous other cancer types.
Acknowledgments
Not applicable.
Funding
This work were supported by Hubei postdoctoral
innovation fund (2016), Wuhan postdoctoral innovation fund (2016),
the self-financing research of the Health Department of Guangxi
Autonomous Region (grant nos. Z2016494 and Z2016499), Scientific
research project in the Guangxi Zhuang Autonomous Region (grant no.
KY2015LX060) and National Natural Science Foundation of China
(grant no. 81560428).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WW and MW participated in the design of the study
and performed the clinical analysis. XY and KX participated in
study design and drafted the manuscript. LX, YL, QM, YT, HL, WY and
QC participated in study design, literature search, and
coordinating and performing the operation. All authors participated
in the conception and design of the study, as well as data
collection and interpretation, manuscript preparation and
literature searches. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient for publication of this report and accompanying images.
Consent for publication
The patients provided written informed consent for
publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stenzl A, Cowan NC, De Santis M, Jakse G,
Kuczyk MA, Merseburger AS, Ribal MJ, Sherif A and Witjes JA: The
updated EAU guidelines on muscle-invasive and metastatic bladder
cancer. Eur Urol. 55:815–825. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Babjuk M, Oosterlinck W, Sylvester R,
Kaasinen E, Böhle A and Palou-Redorta J: European Association of
Urology (EAU): EAU guidelines on non-muscle-invasive urothelial
carcinoma of the bladder. Eur Urol. 54:303–314. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kao LT, Huang CY, Lin HC and Chu CM: No
increased risk of fracture in patients receiving antimuscarinics
for overactive bladder syndrome: A retrospective cohort study. J
Clin Pharmacol. Jan 9–2018.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Balachandran AA and Duckett J: Metastatic
breast cancer presenting as detrusor overactivity. BMJ Case Rep.
2014:pii: bcr2014207920. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Haferkamp A, Schurch B, Reitz A, Krengel
U, Grosse J, Kramer G, Schumacher S, Bastian PJ, Büttner R, Müller
SC and Stöhrer M: Lack of ultrastructural detrusor changes
following endoscopic injection of botulinum toxin type a in
overactive neurogenic bladder. Eur Urol. 46:784–791. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ito Y, Kashiwabara M, Yoshida A, Hikiyama
E, Onoue S and Yamada S: Muscarinic receptor binding in rat bladder
urothelium and detrusor muscle by intravesical solifenacin. Biol
Pharm Bull. 39:1167–1171. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hawthorn MH, Chapple CR, Cock M and
Chess-Williams R: Urothelium-derived inhibitory factor(s)
influences on detrusor muscle contractility in vitro. Br J
Pharmacol. 129:416–419. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang CT, Chen TM, Mei CT, Chang CF, Liu
LL, Chiu KH, Wu TM, Lan YC, Liu WS and Chen YH: The Functional
Haplotypes of CHRM3 Modulate mRNA Expression and Associate
with Bladder Cancer among a Chinese Han Population in Kaohsiung
City. Biomed Res Int. 2016:40528462016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sun Y and Chai T: 319 the role of m3
muscarinic signaling in bladder urothelial cancer cell
proliferation and apoptosis. J Urol. 183:2010. View Article : Google Scholar
|
|
11
|
Gutkind JS, Novotny EA, Brann MR and
Robbins KC: Muscarinic acetylcholine receptor subtypes as
agonist-dependent oncogenes. Proc Natl Acad Sci USA. 88:4703–4707.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ashkenazi A, Ramachandran J and Capon DJ:
Acetylcholine analogue stimulates DNA synthesis in brain-derived
cells via specific muscarinic receptor subtypes. Nature.
340:146–150. 1989. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Von Rosenvinge EC and Raufman JP:
Muscarinic receptor signaling in colon cancer. Cancers (Basel).
3:971–981. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Parnell EA, Calleja-Macias IE, Kalantari
M, Grando SA and Bernard HU: Muscarinic cholinergic signaling in
cervical cancer cells affects cell motility via ERK1/2 signaling.
Life Sci. 91:1093–1098. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Homma Y, Yoshida M, Seki N, Yokoyama O,
Kakizaki H, Gotoh M, Yamanishi T, Yamaguchi O, Takeda M and
Nishizawa O: Symptom assessment tool for overactive bladder
syndrome-overactive bladder symptom score. Urology. 68:318–323.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yi X: Expression and clinical significance
of M1-5 receptor subtype of bladder mucosa in patients with OAB
[D]. Guang Zhou South Med Univ. 2011.
|
|
17
|
Humphrey PA, Moch H, Cubilla AL, Ulbright
TM and Reuter VE: The 2016 WHO classification of tumours of the
urinary system and male genital organs-part B: Prostate and bladder
tumours. Eur Urol. 70:106–119. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tully BT, Li M, Sun Y, Berkowitz J and
Chai TC: Defects in muscarinic receptor cell signaling in bladder
urothelial cancer cell lines. Urology. 74:467–473. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pacini L, De Falco E, Di Bari M, Coccia A,
Siciliano C, Ponti D, Pastore AL, Petrozza V, Carbone A, Tata AM
and Calogero A: M2muscarinic receptors inhibit cell proliferation
and migration in urothelial bladder cancer cells. Cancer Biol Ther.
15:1489–1498. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bschleipfer T, Schukowski K, Weidner W,
Grando S, Schwantes U, Kummer W and Lips K: Expression and
distribution of cholinergic receptors in the human urothelium. Life
Sci. 80:2303–2307. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamanishi T, Kaga K, Fuse M, Shibata C,
Kamai T and Uchiyama T: The role of muscarinic receptor subtypes on
carbachol-induced contraction of normal human detrusor and
overactive detrusor associated with benign prostatic hyperplasia. J
Pharmacol Sci. 128:65–70. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Park YS and Cho NJ: Enhanced proliferation
of SNU-407 human colon cancer cells by muscarinic acetylcholine
receptors. BMB Rep. 41:803–807. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Feng YJ, Zhang BY, Yao RY and Lu Y:
Muscarinic acetylcholine receptor M3 in proliferation and
perineural invasion of cholangiocarcinoma cells. Hepatobiliary
Pancreat Dis Int. 11:418–423. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Arrighi N, Bodei S, Lucente A, Michel MC,
Zani D, Simeone C, Cunico SC, Spano PF and Sigala S: Muscarinic
receptors stimulate cell proliferation in the human
urothelium-derived cell line UROtsa. Pharmacol Res. 64:420–425.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Arrighi N, Bodei S, Zani D, Michel MC,
Simeone C, Cunico Cosciani S, Spano P and Sigala S: Different
muscarinic receptor subtypes modulate proliferation of primary
human detrusor smooth muscle cells via Akt/PI3K and map kinases.
Pharmacol Res. 74:1–6. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Campoy FJ, Vidal CJ, Muñoz-Delgado E,
Montenegro MF, Cabezas-Herrera J and Nieto-Cerón S: Cholinergic
system and cell proliferation. Chem Biol Interact. 259:257–265.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Spindel ER: Muscarinic receptor agonists
and antagonists: Effects on cancer. Handb Exp Pharmacol.
208:451–468. 2012. View Article : Google Scholar
|
|
28
|
Peng Z, Heath J, Drachenberg C, Raufman JP
and Xie G: Cholinergic muscarinic receptor activation augments
murine intestinal epithelial cell proliferation and tumorigenesis.
BMC Cancer. 13:2042013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Liu WT, Huang KY, Lu MC, Huang HL, Chen
CY, Cheng YL, Yu HC, Liu SQ, Lai NS and Huang HB: TGF-β upregulates
the translation of USP15 via the PI3K/AKT pathway to promote p53
stability. Oncogene. 36:2715–2723. 2017. View Article : Google Scholar : PubMed/NCBI
|