Introduction
Gastric cancer (GC) is the second most frequent
cause of cancer-associated mortality in China (1). Due to the majority of patients do not
have specific clinical symptoms and most patients are in late stage
at first presentation, its local infiltration and remote metastasis
lead to difficult radical operation (2). Despite improvements in the surgical
treatment of gastric adenocarcinoma, the recurrence rate remains
high particularly in patients with advanced stage disease and
surgery alone is an insufficient treatment modality (3).
Chemotherapy has beneficial effects on survival
rates in patients with advanced-stage GC; however, overall survival
times remain at ~1 year after diagnosis (2). Toxic side effects of chemotherapy have
motivated the research and development of less harmful
alternatives, including targeted therapy and immunotherapy. Novel
approaches using inhibition of human epidermal growth factor
receptor 2 (HER2) have demonstrated significant improvements in
progression-free and overall survival, compared with chemotherapy
alone, in first-line treatment of patients with an overexpression
of HER2 (3). In addition, second-line
treatment with the vascular endothelial growth factor
receptor-inhibitor ramucirumab demonstrated significant benefits in
terms of overall survival, compared with best supportive care, in
randomized studies (4).
Adoptive cellular immunotherapy (ACI) has been
demonstrated to be a promising cancer therapeutic and has achieved
partial success in numerous countries over the last two decades
(5). In recent years, the importance
of personal antigen-based antitumor immunotherapy has grown
rapidly. The adoptive transfer of in vitro generated tumor
antigen-specific cytotoxic T lymphocytes (CTL) provides a promising
approach to the immunotherapy of cancer (6). Published randomized clinical trials have
established its safety and efficacy in different types of cancer
(6,7).
However, to the best of our knowledge, the disappearance of
multiple bone metastases in chemotherapy-resistant GC with this
type of treatment has not been reported.
The present case report describes a patient with
chemotherapy-resistant GC with multiple bone metastases received
antigen peptide-pulsed dendritic cell (DC)-cytotoxic T lymphocyte
(CTL) therapy combined with oral administration of low-dose
cyclophosphamide, and achieved marked remission lasting >1
year.
Case report
Patient history
Written informed consent was obtained from the
patient for publication of the present case report and any
accompanying results. Ethical approval was obtained from the ethics
committee of Drum Tower Hospital, Nanjing, China. A 62 year-old
female was diagnosed as recurrent GC with multiple bone metastases
at Drum Tower Hospital (Nanjing, China) in September 2013. She had
followed an initial surgical removal of a stage IIIC poorly
differentiated adenocarcinoma 5 years previously. The patient
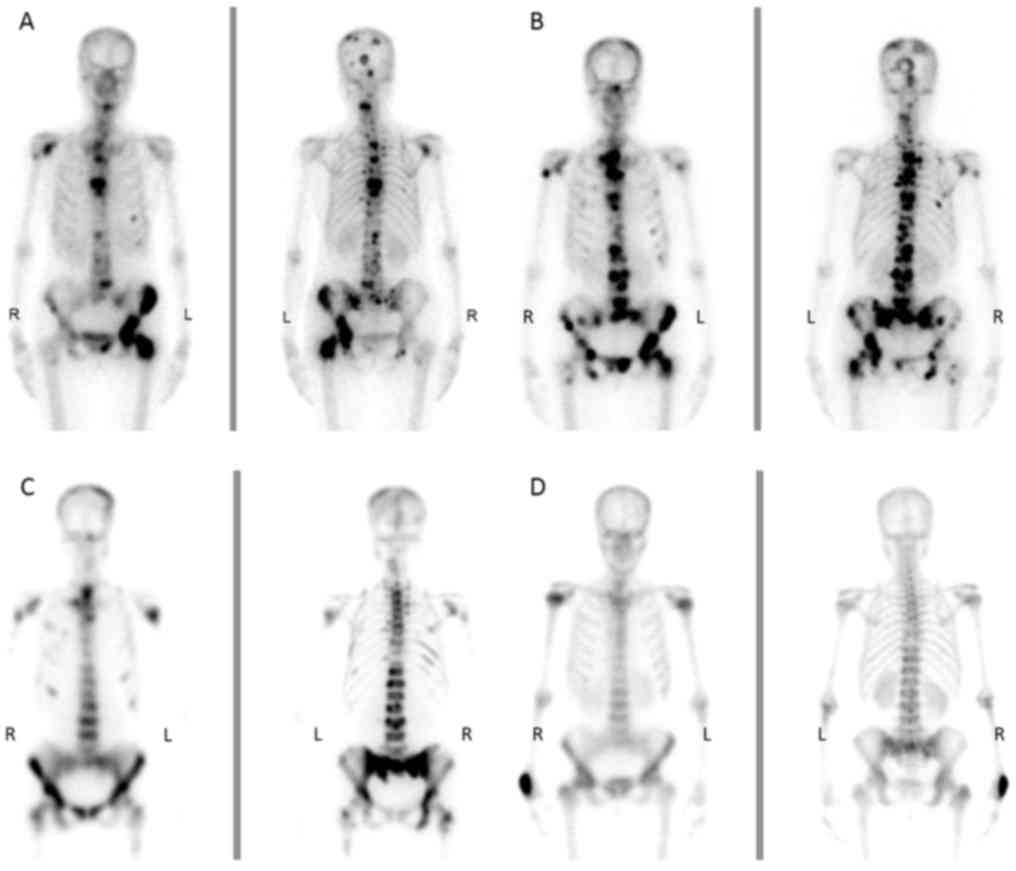
presented with whole body arthralgia and bone pain. Fig. 1 presents the Radionuclide bone imaging
of the patient at four stages of the therapy (Fig. 1A, prior to chemotherapy; Fig. 1B, after chemotherapy and prior to
immunotherapy; Fig. 1C, after 3
cycles of immunotherapy; and Fig. 1D,
after 8 cycles of immunotherapy). Fig.
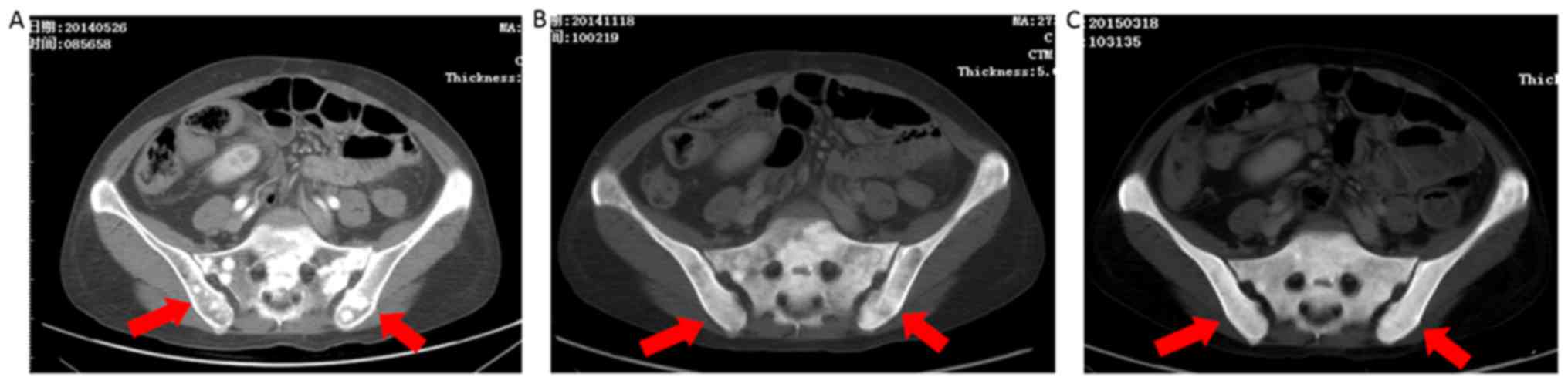
2 presents the enhanced computed tomography (CT) of the patient
at three stages of the therapy (Fig.
2A, prior to immunotherapy; Fig.
2B, after 3 cycles of immunotherapy; and Fig. 2C, after 8 cycles of immunotherapy).
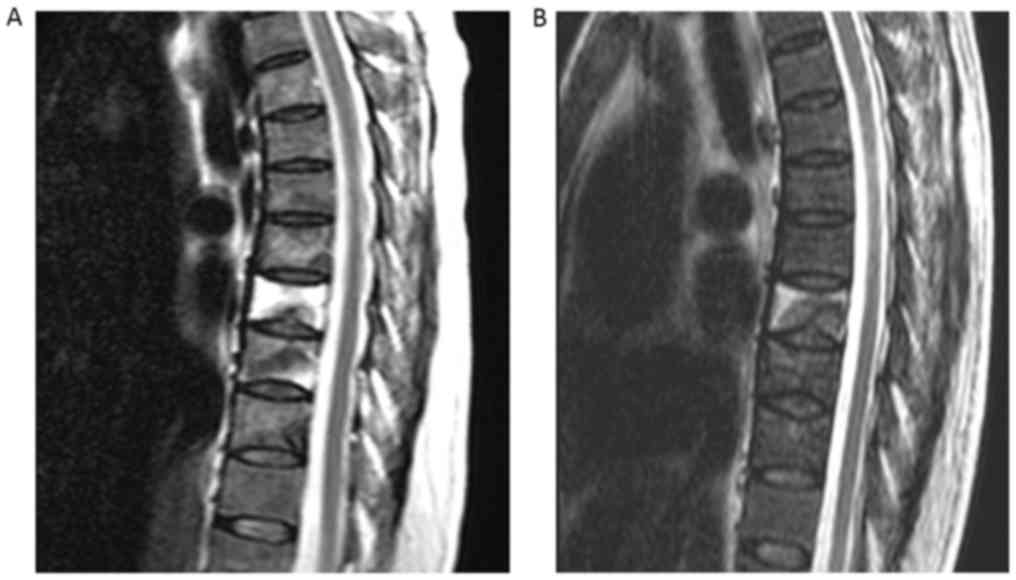
Fig. 3 presents the magnetic
resonance imaging of the patient at two stages of the therapy
(Fig. 3A, prior to immunotherapy, and
Fig. 3B, after 8 cycles of
immunotherapy). Radionuclide bone imaging (Fig. 1A), enhanced computed tomography (CT)
(Fig. 2A) and magnetic resonance
imaging (MRI) (Fig. 3A) revealed
multiple bone metastases. The patient underwent 6 cycles of
combined chemotherapy with S-1 and docetaxel; however, this caused
an increase in metastatic lesions and bone pain. Further
radiological investigation demonstrated disease progression and
resistance to chemotherapy (Fig. 1B).
In addition, the patient experienced severe adverse reactions
including neurotoxicity and nausea [World Health Organization (WHO)
grade III] due to the chemotherapy regime, and was therefore unable
to tolerate the cytotoxic side effects. In June 2014, the patient
was recommended to undergo adoptive immunotherapy with personalized
antigen peptide-pulsed DC-CTLs.
Selection of targeted antigen
peptides
The patient's human leukocyte antigen (HLA)-typed
was performed by sequence-specific primer amplification (PCR-SSP)
using One Lambda DNA generic typing trays (One Lambda; cat. no. Lot
006; Thermo Fisher Scientific, Inc.) pre-coated with primers
specifically designed to detect HLA polymorphism. According to the
manufacturer's protocol. The PCR reaction system was 10 µl in
total, and contained 100 ng DNA template. The amplification
conditions were as follows (8): For
first cycle of denaturation at 96°C for 130 sec and renaturation at
63°C for 10 sec, followed by 9 cycle jumps between 96°C for 10 sec
and 63°C for 1 min. Further 20 cycles of denaturation at 96°C for
10 sec, annealing at 59°C for 50 sec, and polymerization at 72°C
for 30 sec. The PCR amplified products were examined by agarose gel
electrophoresis, and the results were observed under a UV lamp and
photographed. According to the resulting fragment size, the
genotype was determined by contrast with the Micro SSP™ HLA class I
DNA typing interpretation card (One Lambda; Thermo Fisher
Scientific, Inc.) and the One Lambda DNA/LMT software, version 3.98
(One Lambda; Thermo Fisher Scientific, Inc.). The result was
positive for HLA-A*2402. Patient tumor samples (5 µm slices of
paraffin-embedded stomach cancer) were obtained and underwent
immunohistochemical staining analysis. IHC staining was performed
on paraffin-embedded histological sections (thickness, 5 µm) that
were fixed in 10% buffered formalin for 24–48 h, using a polymer
peroxidase method (9) (Envision+/HRP;
Dako; Agilent Technologies, Inc., Santa Clara, CA, USA). The
operation was performed using the Envision™ kit (Dako; Agilent
Technologies, Inc., Santa Clara, CA, USA) according to the
manufacturer's protocol. Briefly, following deparaffnization with
xylene and anhydrous ethanol (95, 85 and 80% for 4 min each), the
tissue sections were treated with 0.3% hydrogen peroxide in
methanol for 30 min at room temperature to block endogenous
peroxidase activity, followed by incubation with the primary
antibodies [carcinoembryogenic antigen (CEA) primary antibody,
rabbit anti-human polyclonal antibody; cat. no. ZA-0063; 1:100; and
vascular endothelial growth factor receptor 2 (VEGFR-2) primary
antibody, rabbit anti-human polyclonal antibody; cat. no. ZA-0287;
1:100; Beijing Zhongshan Jinqiao Biotechnology Co., Ltd., Beijing,
China] in a humidified chamber at 4°C overnight. Slices were the
incubated with horseradish peroxidase-conjugated secondary goat
anti-rabbit antibody (cat. no. SM801; ENvision + kit; Dako; Agilent
Technologies, Inc) for 30 min at room temperature. The
immunoreactivity was visualized using a 3,3′-diaminobenzidine for 5
min and hematoxylin stain for 2 min at room temperature. Expression
of these proteins was evaluated using optical microscopy (BX43;
Olympus Corporation, Tokyo, Japan) as positive when the nucleus of
the cancerous tissue was stained. The staining of each specimen was
evaluated at magnification, ×40 or ×400. The rate of
positive-stained cancer cells was evaluated in three randomly
selected areas (size, 200×200 µm) from the tumor specimens. When
the average positive tumor rate was >10%, the tumor was defined
as being positively stained. Positive controls (tissues known to be
positive for antigen expression) and negative controls (replaced
primary antibody with normal rabbit (rat) serum and the result was
negative) were included in each run. Results demonstrated
overexpression of CEA and VEGFR-2. CEA-652 peptide (TYACFVSNL; cat.
no. 04010007767; GenScript, Co., Ltd., Nanjing, China) (10) and VEGFR-2-169 peptide (RFVPDGNRI; cat.
no. 04010013003; GenScript, Co., Ltd.) (11) were used for DC loading according to
protocols previously described (12).
Ex vivo expansion of DCs and CTLs
obtained from peripheral blood
Peripheral blood mononuclear cells (PBMCs) were
collected using the peripheral blood mononuclear cell collection
program COBE Spectra™ MNC program (Terumo BCT Co., Ltd., Lakewood,
CO, USA) and transported to the laboratory under cold conditions
(4°C). In vitro cell processing and expansion were performed
in a good manufacturing practices-compliant laboratory. DCs and
CTLs were obtained from blood mononuclear cells as described
previously (12,13). DCs were loaded with HLA-A*2402-binding
peptides derived from CEA and VEGFR-2, and CTLs were stimulated
with mature DCs and cultured in complete medium containing 10%
human AB serum (Gibco; Thermo Fisher Scientific, Inc.) and 1–2% T
cell growth factor (Gibco; Thermo Fisher Scientific, Inc.). Cell
counts were estimated using the trypan blue dye-exclusion method
(14). The average cell count of
PBMCs prior to each expansion was 2.7×108, and, after 2
weeks of in vitro expansion, the mean cell count of expanded
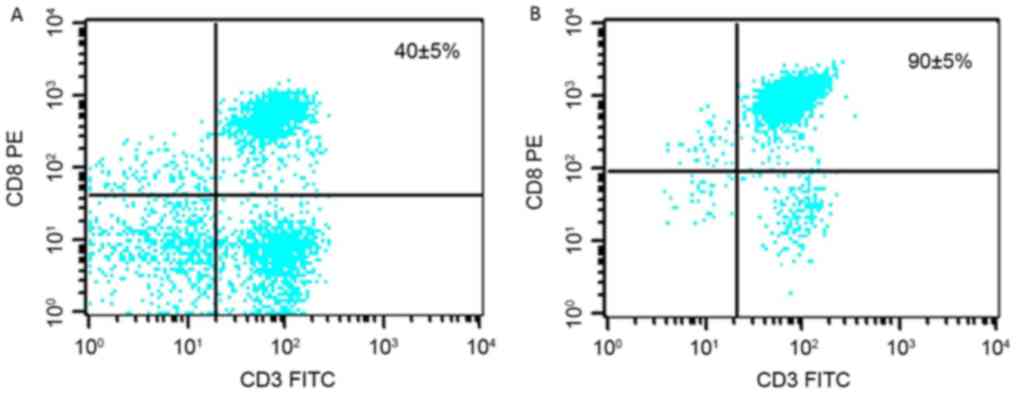
lymphocytes for each injection was 3.9×1010. The mean
frequency of activated CTLs [cluster of differentiation
CD3+/CD8+] was determined using flow
cytometry (BD Biosciences, Franklin Lakes, NJ, USA). FACS Ariar
cell sorter (BD Biosciences) was used to perform fluorescent
expression analysis. Cells were harvested and stained with mouse
anti-human antibody labeled by direct fluorescence antibody for 30
min in 4°C, in darkness as follows: CD3-FITC (HIT3a; cat. no.
561806; BD Biosciences), CD8C-PE (HIT8a; cat. no. 561949; BD
Biosciences). The fluorescence antibody was diluted 1:40 and PBS
containing 1% BSA were used as the dilution and washing buffer.
Cells were washed two times by centrifuging at the speed of 250 × g
for 5 min at 4°C. Data were analyzed using FlowJo software 7.6.1
(Tree Star, Inc., Ashland, OR, USA) following gating for CD3+ T
cells. Results revealed an initial average frequency of 40%;
however, the final culture revealed an average activation of 90%
(Fig. 4). Each CTL infusion was
accompanied by a 5-day course of low-dose interleukin-2 (IL-2;
4×106U daily). Prior to cell transplantation, cells were
tested for endotoxin levels using a Limulus Amebocyte Lysate kit
(Charles River Laboratories, Ltd., Mumbai, India) to ensure that
products were aseptic. Interferon-γ enzyme-linked immunospot
(ELISPOT) assay was conducted using PBMCs periodically obtained
from the patient prior to and following immunotherapy in order to
assess cellular immune responses to CEA and VEGFR-2. IFN-γ ELISPOT
kit (Shenzhen Dakewei Biotechnology Co. Ltd, Anshan, China) was
used to determine the frequency of cytokine-expressing T cells
following overnight activation with peptides at 37°C. The kit was
used according to manufacturer's protocol. Briefly, T cells (105
cells per well) and peptides (50 mg/ml) were added to duplicate
wells and DCs were added at a ratio of 1:10 (DC:T cells) for 18–20
h at 37°C. The plates were washed prior to the addition of the
diluted detection antibody (1:100 dilution) and then incubated for
1 h at 37°C, followed by incubation with streptavidin-alkaline
phosphatase-conjugated antibody (1:100 dilution) was added and
incubated at 37°C for a further 1 h. Aminoethyl carbazole solution
mix was then added to each well, and the plates were left in the
dark for 15–25 min at room temperature followed by deionized water
being added to stop development. Plates were scanned using an
Elispot CTL Reader (Cell Technology Inc., Columbia, MD) and the
results were analyzed using ImmunoSpot 5.0.41 Professional (Cell
Technology Inc., Cleveland, OH, USA). A paired Student's t-test was
applied using Graphpad Prism 5 statistical software (GraphPad
Software, Inc., La Jolla, CA, USA). P<0.05 was considered to
indicate a statistically significant difference.
Treatment plan
The patient received 8 cycles of antigen
peptide-pulsed DC-CTLs with an oral administration of low-dose of
cyclophosphamide (50 mg daily) from June 2014 to May 2015. Each
cycle included the administration of two DC vaccines
(1.2~1.6×107 in 1 ml 0.9% sodium chloride injection) and
four infusions of CTLs (0.8~1.4×1010 in 100 ml 0.9%
sodium chloride injection). The DCs and CTLs were administered
intradermally and intravenously, respectively. Throughout the
course of treatment, the progression of the metastatic bone lesions
was monitored using CT, MRI and ECT. Adverse clinical effects
following large-dosage lymphocyte transfusions were mild and
consisted of chills and fever (WHO grade I) and typically occurred
within 6–8 h of CTL infusion, with recovery following symptomatic
treatment with acetaminophen (0.3–0.6 g each time, orally, three
times a day).
Results
Evaluation of the immune response
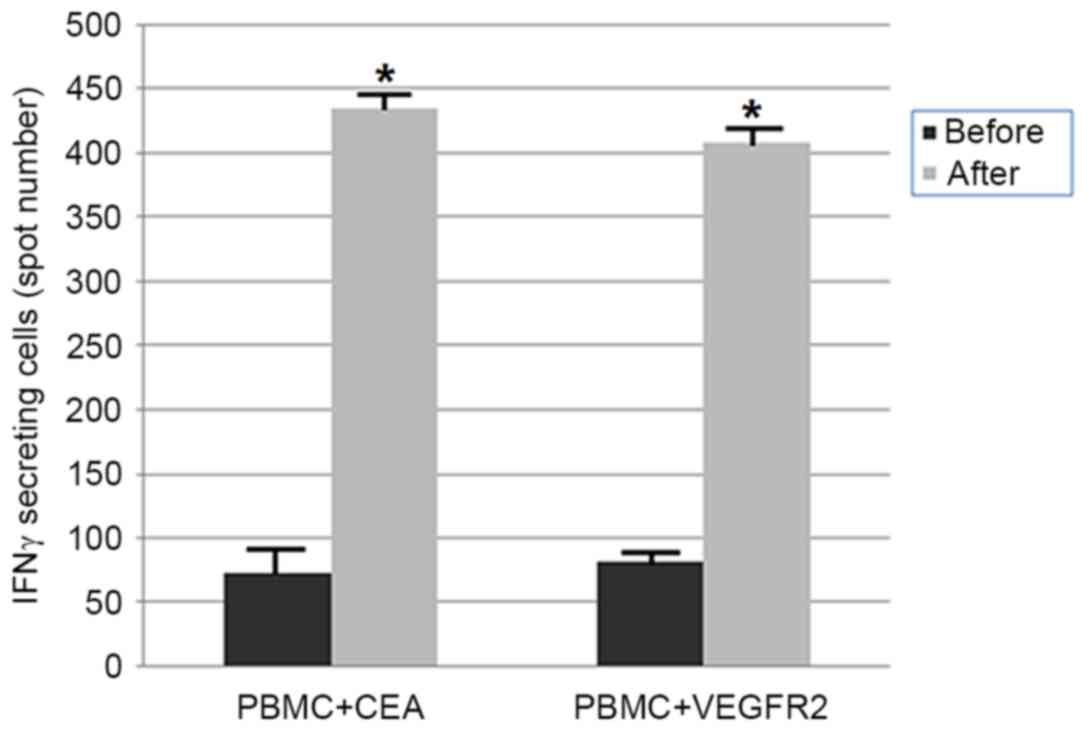
Interferon-γ ELISPOT assays were conducted using
PBMCs periodically obtained from the patient prior to and following
treatment in order to assess cellular immune responses. Positive
CTL responses specific to the vaccinated peptides were determined
as previously described (10).
Interferon-γ secretion was significantly higher on CTL by the
stimulation of HLA-A*2402-binding peptides CEA and VEGFR-2
following 4 cycles of immunotherapy compared with control T cells
prior to immunotherapy (P<0.05) (Fig.
5).
Imaging evaluation of clinical
response
Following 3 cycles of treatment, CT scan
demonstrated a decrease in multiple patchy high-density shadows
located in the pelvis (Fig. 2B). The
radionuclide bone-imaging scan indicated a marked decrease in the
number of multiple bone metastases (Fig.
1C). Following completion of 8 cycles of autologous immune
enhancement therapy, the number of multiple bone metastases was
markedly decreased, this was further confirmed in June 2015 using
CT imaging (Fig. 2C), a radionuclide
bone imaging scan (Fig. 1D) and an
MRI scan (Fig. 3B). Furthermore, the
patient's weight had increased, appetite and quality of life were
improved and the arthralgia and bone pain were also relieved.
Overall, the patient was doing well at the time of writing.
Discussion
The present case was the first report of the
disappearance of almost all bone metastases following antigen
peptide-pulsed DC-CTLs immunotherapy in chemotherapy-resistant
gastric cancer. We also investigated the safety and efficacy of the
ex vivo activated, expanded and adoptively transferred
antigen peptide-pulsed DC-CTLs obtained from the peripheral blood
of a stage IV chemotherapy-resistant patient with GC and multiple
bone metastases, whose bone metastases was markedly decreased
following therapy and without serious adverse reactions.
As an immune-based approach, adoptive therapy has
become an increasingly attractive modality for cancer therapy due
to collectively demonstrating a decreased risk of cross-resistance
compared with conventional therapies, high specificity and
long-term immune protection (15).
Recent success of adoptive T cell therapy using ex vivo
expanded autologous tumor-reactive T cells has increased optimism
that this modality may form a specific therapy for patients with
advanced-stage disease, including those who are refractory to
standard therapies (16,17). Previously, autologous immune cells
intravenously administered to patients with GC have resulted in
improved survival rates compared with controls, as reported by
Zhang et al (18).
CEA and VEGFR-2 are the most commonly expressed
antigens in GC. CEA epitopes and VEGFR-2 epitopes presented in the
HLA-A*0201 and HLA-A*2402 context are frequently recognized by T
cells (10,11) As a result, the majority of recent
adoptive cell therapy protocols have targeted these antigens and
reported encouraging immunological and clinical responses (10,11). Over
the course of an adoptive cell transfer, monitoring
antigen-specific T cell expansion in patient blood is crucial for
predicting the clinical efficacy of such an immunological approach.
The patient was administered with ex vivo generated CEA- and
VEGFR-2-specific CTLs. Following 4 cycles of adoptive transfer, the
ELISPOT results demonstrated that the number of antigen-specific T
cells were markedly increased in the patient's blood.
The clinical efficacy of current tumor immunotherapy
methods is not satisfactory as immunosuppressive mechanisms
[including regulatory T cells (Treg) and myeloid-derived suppressor
cells] are predominant in patients with cancer at an advanced stage
(19–21). A previous study demonstrated that
cyclophosphamide exerted variable effects on depleting suppressive
Tregs, which resulted in enhanced T cell reactivity (22). Research also demonstrated that
cyclophosphamide at a low dose selectively depleted Tregs, whereas
at a high dose, cyclophosphamide led to a loss in specificity of
Treg depletion in patients with cancer (23). Using this strategy, marked clinical
benefits have been obtained, such as a significant delay in tumor
progression. Numerous proof-of-concept clinical trials in patients
with cancer indicated that the efficacy of adoptive cellular
therapy may be enhanced using chemotherapy (24–26). In
the present case report, oral administration of low-dose
cyclophosphamide accompanied by immune cell transfusions resulted
in the almost complete disappearance of all multiple bone
metastases in chemotherapy-resistant GC, which lasted for over one
year. Therefore, optimizing the combination of adoptive cellular
therapy and other immune-based or conventional approaches may
herald a new generation of research and clinical opportunities for
cancer immunotherapy.
In conclusion, specific antigen peptide-pulsed
DC-CTLs combined with low-dose cyclophosphamide administered to the
patient with stage IV chemotherapy-resistant GC, demonstrated its
safety by not exhibiting any severe adverse reactions. There was
also a marked decrease in bone metastatic lesions, improved quality
of life and a prolonged duration of progression-free survival over
one year. This is also in agreement with previous studies (27–29) on
cell-based immunotherapies. Therefore, it is recommended that the
adoptive transfer of personalized antigen peptide-pulsed DC-CTLs
may serve as a promising specific immunotherapy strategy for
patients with malignant disease, and may be considered in
combination with oral administration of low-dose cyclophosphamide
or other modalities of treatment in cases of a similar nature.
Acknowledgements
Not applicable.
Funding
The authors acknowledge the financial support from
National Natural Science Foundation of China (grant nos. 81572601
and 81602077), and the Science and Technology Project Foundation of
Nanjing (grant no. 201715019).
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JD and BL undertook study conception and design. JD,
JW, YY, SS, JS, FC, FM and BL were responsible for the collection
and assembly of data: Data analysis and interpretation were the
responsibilities of JD, SS, JS, FC, FM, ZZ and BL. JD wrote the
manuscript. Final approval of manuscript was given by JD, JW, YY,
SS, JS, FC, FM, ZZ and BL.
Ethics approval and consent to
participate
Ethical approval was obtained from the ethics
committee of Drum Tower Hospital, Nanjing, China. Study
participants provided written informed consent.
Consent for publication
Written informed consent was obtained from the
patient for publication of the present case report and any
accompanying results.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wesolowski R, Lee C and Kim R: Is there a
role for second-line chemotherapy in advanced gastric cancer?
Lancet Oncol. 10:903–912. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kim HJ and Oh SC: Novel systemic therapies
for advanced gastric cancer. J Gastric Cancer. 18:1–19. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Satolli MA, Buffoni L, Spadi R and Roato
I: Gastric cancer: The times they are a-changin’. World J
Gastrointest Oncol. 7:303–316. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gattinoni L, Powell DJ Jr, Rosenberg SA
and Restifo NP: Adoptive immunotherapy for cancer: Building on
success. Nat Rev Immunol. 6:383–393. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yee C: The use of endogenous T cells for
adoptive transfer. Immunol Rev. 257:250–263. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ernst B and Anderson KS: Immunotherapy for
the treatment of breast cancer. Curr Oncol Rep. 17:52015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sheu BC, Chiou SH, Chang WC, Chow SN, Lin
HH, Chen RJ, Huang SC, Ho HN and Hsu SM: Integration of high-risk
human papillomavirus DNA correlates with HLA genotype aberration
and reduced HLA class I molecule expression in human cervical
carcinoma. Clin Immunol. 115:295–301. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Watanabe Y, Saito M, Saito K, Matsumoto Y,
Kanke Y, Onozawa H, Hayase S, Sakamoto W, Ishigame T, Momma T, et
al: Upregulated HOXA9 expression is associated with lymph node
metastasis in colorectal cancer. Oncol Lett. 15:2756–2762.
2018.PubMed/NCBI
|
|
10
|
Sakakibara M, Kanto T, Hayakawa M, Kuroda
S, Miyatake H, Itose I, Miyazaki M, Kakita N, Higashitani K,
Matsubara T, et al: Comprehensive immunological analyses of
colorectal cancer patients in the phase I/II study of quickly
matured dendritic cell vaccine pulsed with carcinoembryonic antigen
peptide. Cancer Immunol Immunother. 60:1565–1575. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Masuzawa T, Fujiwara Y, Okada K, Nakamura
A, Takiguchi S, Nakajima K, Miyata H, Yamasaki M, Kurokawa Y, Osawa
R, et al: Phase I/II study of S-1 plus cisplatin combined with
peptide vaccines for human vascular endothelial growth factor
receptor 1 and 2 in patients with advanced gastric cancer. Int J
Oncol. 41:1297–1304. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mackensen A, Meidenbauer N, Vogl S, Laumer
M, Berger J and Andreesen R: Phase I study of adoptive T-cell
therapy using antigen-specific CD8+ T cells for the treatment of
patients with metastatic melanoma. J Clin Oncol. 24:5060–5069.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kavanagh B, Ko A, Venook A, Margolin K,
Zeh H, Lotze M, Schillinger B, Liu W, Lu Y, Mitsky P, et al:
Vaccination of metastatic colorectal cancer patients with matured
dendritic cells loaded with multiple major histocompatibility
complex class I peptid. J Immunother. 30:762–772. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Strober W: Trypan blue exclusion test of
cell viability. Curr Protoc Immunol. 111:A3.B.1–3. 2015. View Article : Google Scholar
|
|
15
|
Wang M, Yin B, Wang HY and Wang RF:
Current advances in T-cell-based cancer immunotherapy.
Immunotherapy. 6:1265–1278. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Carluccio S, Delbue S, Signorini L, Setola
E, Bagliani A, Della Valle A, Galli A, Ferrante P and Bregni M:
Generation of tumor-specific cytotoxic T-lymphocytes from the
peripheral blood of colorectal cancer patients for adoptive T-cell
transfer. J Cell Physiol. 230:1457–1465. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Khammari A, Labarrière N, Vignard V,
Nguyen JM, Pandolfino MC, Knol AC, Quéreux G, Saiagh S, Brocard A,
Jotereau F and Dreno B: Treatment of metastatic melanoma with
autologous Melan-A/MART-1-specific cytotoxic T lymphocyte clones. J
Invest Dermatol. 129:2835–2842. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang GQ, Zhao H, Wu JY, Li JY, Yan X,
Wang G, Wu LL, Zhang XG, Shao Y, Wang Y and Jiao SC: Prolonged
overall survival in gastric cancer patients after adoptive
immunotherapy. World J Gastroenterol. 21:2777–2785. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Karimi S, Chattopadhyay S and Chakraborty
NG: Manipulation of regulatory T cells and antigen-specific
cytotoxic T lymphocyte-based tumour immunotherapy. Immunology.
144:186–196. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lake RA and Robinson BW: Immunotherapy and
chemotherapy-a practical partnership. Nat Rev Cancer. 5:397–405.
2005. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ghiringhelli F, Menard C, Puig PE, Ladoire
S, Roux S, Martin F, Solary E, Le Cesne A, Zitvogel L and Chauffert
B: Metronomic cyclophosphamide regimen selectively depletes
CD4+CD25+ regulatory T cells and restores T and NK effector
functions in end stage cancer patients. Cancer Immunol Immunother.
56:641–648. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Scurr M, Pembroke T, Bloom A, Roberts D,
Thomson A, Smart K, Bridgeman H, Adams R, Brewster A, Jones R, et
al: Low-dose cyclophosphamide induces antitumor T-cell responses,
which associate with survival in metastatic colorectal cancer. Clin
Cancer Res. 23:6771–6780. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Peng S, Lyford-Pike S, Akpeng B, Wu A,
Hung CF, Hannaman D, Saunders JR, Wu TC and Pai SI: Low-dose
cyclophosphamide administered as daily or single dose enhances the
antitumor effects of a therapeutic HPV vaccine. Cancer Immunol
Immunother. 62:171–182. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Suzuki E, Kapoor V, Jassar AS, Kaiser LR
and Albelda SM: Gemcitabine selectively eliminates splenic
Gr-1+/CD11b+ myeloid suppressor cells in tumor-bearing animals and
enhances antitumor immune activity. Clin Cancer Res. 11:6713–6721.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sevko A, Michels T, Vrohlings M, Umansky
L, Beckhove P, Kato M, Shurin GV, Shurin MR and Umansky V:
Antitumor effect of paclitaxel is mediated by inhibition of
myeloid-derived suppressor cells and chronic inflammation in the
spontaneous melanoma model. J Immunol. 190:2464–2471. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Vincent J, Mignot G, Chalmin F, Ladoire S,
Bruchard M, Chevriaux A, Martin F, Apetoh L, Rébé C and
Ghiringhelli F: 5-Fluorouracil selectively kills tumor-associated
myeloid-derived suppressor cells resulting in enhanced T
cell-dependent antitumor immunity. Cancer Res. 70:3052–3061. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kimura H, Matsui Y, Ishikawa A, Nakajima
T, Yoshino M and Sakairi Y: Randomized controlled phase III trial
of adjuvant chemo-immunotherapy with activated killer T cells and
dendritic cells in patients with resected primary lung cancer.
Cancer Immunol Immunother. 64:51–59. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lutzky VP, Crooks P, Morrison L, Stevens
N, Davis JE, Corban M, Hall D, Panizza B, Coman WB, Coman S and
Moss DJ: Cytotoxic T cell adoptive immunotherapy as a treatment for
nasopharyngeal carcinoma. Clin Vaccine Immunol. 21:256–259. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fournier C, Martin F, Zitvogel L, Kroemer
G, Galluzzi L and Apetoh L.: Trial Watch: Adoptively transferred
cells for anticancer immunotherapy. Oncoimmunology. 6:e13631392017.
View Article : Google Scholar : PubMed/NCBI
|