Introduction
Breast cancer is the most common cancer in females
globally, with the incidence rate increasing 0.5% every year. In
addition, a gradual trend is forming for the cancer to occur in
females of a younger age and the morbidity rate is increasing,
which severely threatens the health of women around the world
(1,2),
although its precise mechanism is presently unclear. Growing
evidence has suggested that the tumor microenvironment serves a
role in the development of cancer and its prognosis (3,4).
Cell adhesion molecules are a type of glycoprotein
mediating cell-cell and cell-extracellular matrix adhesion, and
they serve an important role in the genesis, development, invasion
and metastasis of tumors (5). The
decrease in tumor cell adhesion appears to easily affect tumor
invasion and metastasis. Epithelial-cadherin (E-cadherin) is an
important member of the cadherin family and serves an important
role in the cell adhesion process. It has been reported that
E-cadherin is underexpressed in a variety of tumors, and that it
could participate in the growth, differentiation, metastasis and
prognosis of breast cancer (6–8).
To investigate the expression of the E-cadherin
protein in invasive breast cancer and its possible clinical
significance, 450 cases of invasive ductal carcinoma of the breast
were assessed. The expression of E-cadherin was detected using
immunohistochemistry, and the association between lymph node
metastasis, clinicopathological features and molecular typing was
analyzed. In addition, the roles of E-cadherin in lymph node
metastasis and the prognosis of breast cancer were
investigated.
Patients and methods
Patients
A total of 512 patients with primary invasive ductal
carcinoma of the breast were enrolled at the Affiliated Tumor
Hospital of Xinjiang Medical University (Urumqi, China) between
January 2001 and January 2011. The patients were randomly selected
and 62 cases with non-conforming specimens were excluded from the
study. All specimens were fixed using 10% formaldehyde at 36–38°C
for 6–8 h, embedded in paraffin and sliced into 4-μm continuous
pathological sections.
Case inclusion criteria
Case inclusion criteria were as follows: Diagnosis
according to breast pathology; no history of radiotherapy,
chemotherapy or endocrine therapy prior to admission; Karnofsky
performance status score of ≥80 points and surgery performed with
all samples identified by three pathology experts for
histopathological identification of breast invasive ductal
carcinoma; no other malignancy history; preoperative consent
specimens collected and informed consent obtained; and approval
provided by the Xinjiang Medical University Affiliated Cancer
Hospital Ethics Committee.
Case exclusion criteria
Case exclusion criteria were as follows: Breast
invasive lobular carcinoma and carcinoma in situ; and
preoperative chemotherapy, radiotherapy or endocrine therapy. In
addition, other exclusions were breast cancer metastases and other
specific types of breast tumors (sarcoma, micropapillary carcinoma,
lymphoma, inflammatory breast cancer, male breast carcinoma and
gestational breast cancer).
Basic information of case data
The breast cancer patients were between 28 and 75
years of age, with a mean age of 49.30±10.48 years, and the median
age was 48 years. There were 317 premenopausal patients and 133
postmenopausal patients. All patients were female.
Methods
Immunohistochemical staining of the SP
(streptavidin-peroxidase) method
Breast cancer specimens were treated with dewaxing
and hydration, according to the manufacturer's protocol for
immunohistochemical SP method staining (cat. no. SP0041; Beijing
Solarbio Science and Technology Co., Ltd., Beijing, China), and the
microwave method was used to repair antigens. Specimens of 30
benign fibroadenoma cases were obtained from patients at the
Affiliated Tumor Hospital of Xinjiang Medical University, with a
positive result for E-cadherin was considered as a positive
control, and five fields of view were randomly selected under the
microscope. Each field counted for 100 cells. Patients with benign
fibroadenoma were enrolled at the Affiliated Tumor Hospital of
Xinjiang Medical University between January 2001 and January 2011.
The patients were randomly selected. The patients with benign
fibroadenoma were between 19 and 51 years of age, and the median
age was 32 years. All patients were female and there were 30
patients in the group.
Case inclusion criteria
Case inclusion criteria were as follows: Samples
from surgery were observed by three pathology experts via
histopathological identification to confirm fibroadenoma of the
breast; Karnofsky performance status score of ≥80 points; no
history of tumors; and no family history of tumors.
Case exclusion criteria
Case exclusion criteria were as follows: Breast
fibroadenoma with a history of breast cancer; breast fibroadenoma
with a history of other malignant tumors; and breast fibroadenoma
with mastitis disease.
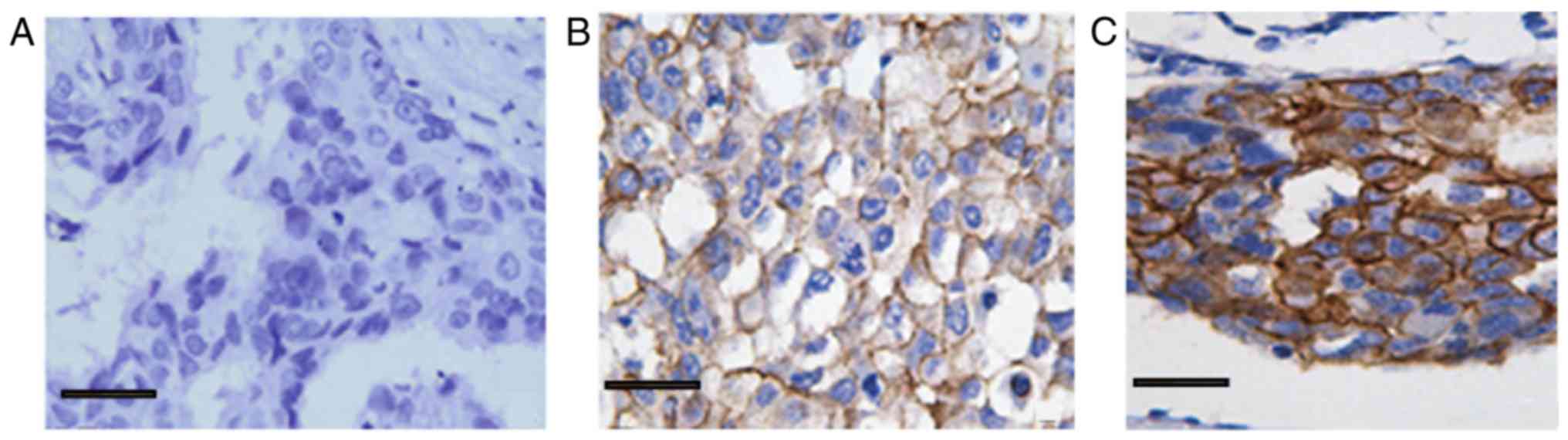
Standard of E-cadherin staining
criteria
The immunohistochemical staining results of the
study were determined by three pathologists, and five ×400
magnification visual fields were randomly observed. E-cadherin
expression was determined by a semi-quantitative method according
to the following score standard for the percentage of cell
staining: 0–10%, 0 points, (−); 11–25%, 1 point, (+); 26–50%, 2
points, (++); 51–75%, 3 points, (+++); and >75%, 4 points,
(++++). Those cells with a score of ≤2 were considered to be
negative for E-cadherin and those with a score of ≥3 were
considered to be positive.
Follow-up method
Telephone follow-up calls were conducted to identify
associated information, the information recorded in the case was
approved by the patient. Patient medical records were used to
record identity, phone numbers, addresses and other personal
information, including postcode, sex and history of breast cancer.
Three phone calls were made to follow-up each patient, and for the
patients who could not be contacted, their last discharge time was
used. The follow-up calendar period was until January 31, 2016, and
the follow-up time period was 1–72 months.
Tumor, Node, Metastasis staging of breast cancer was
performed according to the American Joint Committee on Cancer
Staging of Breast Cancer (7th Edition) (1). The histological grading of breast cancer
was primarily evaluated according to the degree of glandular tube
formation, nuclear polymorphisms and mitosis counts. These three
aspects were scored between 3–5 points (level I; differentiation),
6–7 (level II; moderately differentiated) and 8–9 (grade III; poor
differentiation) (2).
Statistical analysis
All data were shown as the mean ± standard deviation
and analyzed using a univariate analysis, χ2test or
exact probability method. A survival analysis was performed using
the Kaplan-Meier method, with the log-rank test, and the SPSS 18.0
statistical software (SPSS, Inc., Chicago, IL, USA) was used.
P<0.05 indicated that the difference was statistically
significant.
Results
Expression of E-cadherin in benign
breast hyperplasia tissue
E-cadherin was mainly distributed in the gland duct
epithelium and acinar epithelial cell membrane in the benign breast
fibroadenoma samples, and was observed as the positive
brownish-yellow granules (Fig. 1).
The 30 cases of breast fibroadenoma were enrolled at the Affiliated
Tumor Hospital of Xinjiang Medical University (Urumqi, China)
between January 2001 and January 2011. The patients were randomly
selected. The 30 cases of breast fibroadenoma were positive for
E-cadherin.
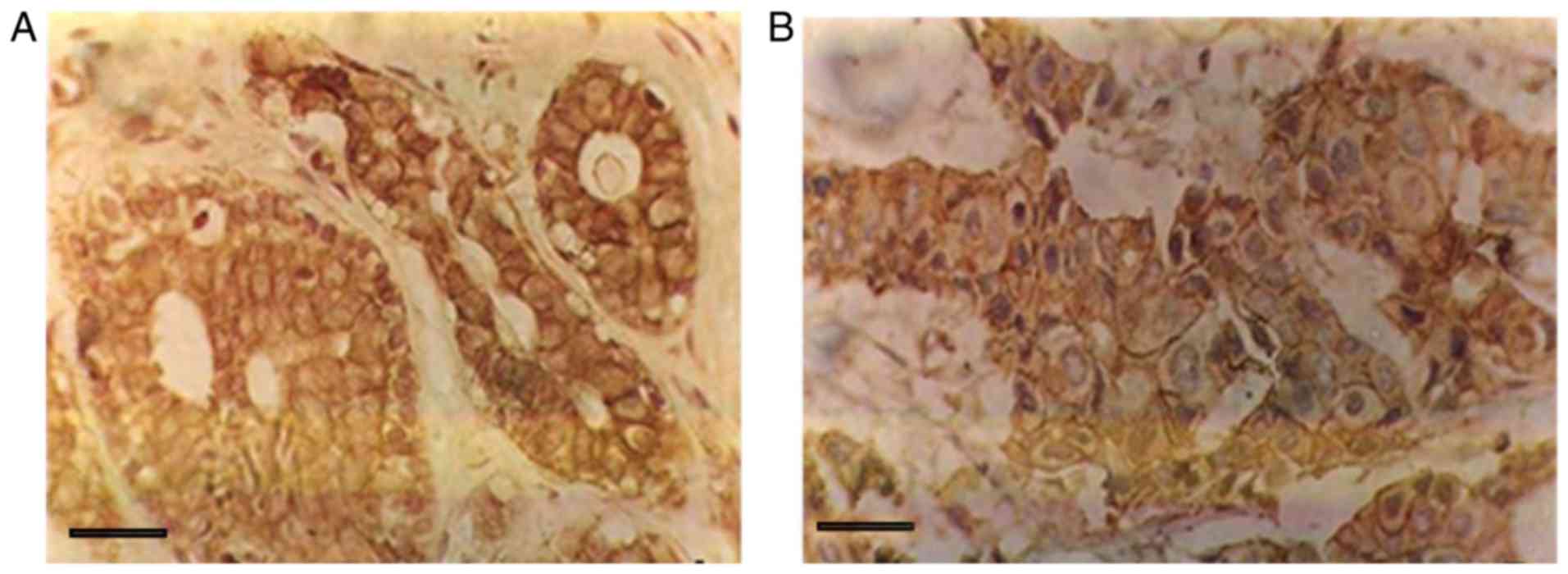
Comparing the expression of E-cadherin
in invasive ductal carcinoma of the breast and benign mammary gland
hyperplasia
As shown in Fig. 1,
E-cadherin staining was positive in breast epithelial cells and
stromal cells (brownish-brown particles; SP, ×400 magnification).
The expression of E-cadherin in the membranes of infiltrating
breast carcinoma cells is shown in Fig.
2. The positive expression rate of E-cadherin was 36.44% in the
450 cases of invasive ductal carcinoma. The high expression rate
was 77/157 (49.04%) in 157 non-metastatic cancer tissues and 87/293
(29.69%) in 293 lymph nodes with lymph node metastasis. This
finding indicated that E-cadherin expression in breast cancer
tissue is significantly lower in the lymph node metastasis of
breast invasive ductal carcinoma than the breast cancer without
lymph node metastasis (χ2=16.528, P<0.001; Table I). The low expression of E-cadherin
was associated with metastatic lymph node metastasis.
 | Table I.Association between E-cadherin
expression and lymph node metastasis. |
Table I.
Association between E-cadherin
expression and lymph node metastasis.
|
|
| Lymph node
metastasis, n (%) |
|
|
|---|
|
|
|
|
|
|
|---|
| E-cadherin | n | Yes | No | χ2 | P-value |
|---|
| High expression | 164 | 87 (53.0) | 77 (47.0) | 16.528 |
<0.001a |
| Low expression | 286 | 206 (72.0) | 80 (28.0) |
Expression of E-cadherin in breast
invasive ductal carcinoma and its association with the
clinicopathological features of breast cancer
As presented in Table
II, the expression of E-cadherin exhibited significant
differences with regard to the age of the patient, lymph node
metastasis, tumor size, estrogen receptor (ER) expression,
molecular classification and tumor cell classification. Patients
aged >60 years were significantly associated with the positive
expression of E-cadherin. However, there were no significant
differences in tumor stage, whether the patients were menopausal or
premenopausal, or the expression of receptor tyrosine-protein
kinase erbB-2 and proliferation marker protein Ki-67.
| Table II.Expression of E-cadherin in
clinicopathological features of breast cancer. |
Table II.
Expression of E-cadherin in
clinicopathological features of breast cancer.
|
|
| E-cadherin
expression, n |
|
|
|
|---|
|
|
|
|
|
|
|
|---|
| Clinicopathological
factors | n | High expression | Low expression | High expression rate,
% | χ2 | P-value |
|---|
| Total patients | 450 | 164 | 286 | 36.444 |
|
|
| Age, years |
|
|
|
|
|
|
| ≤35 | 87 | 40 | 47 | 45.977 | 8.373 | 0.015a |
|
35–60 | 253 | 95 | 158 | 37.549 |
|
|
| ≥60 | 110 | 29 | 81 | 26.364 |
|
|
| Number of positive
lymph nodes No transfer | 157 | 77 | 80 | 49.044 | 18.796 |
<0.001a |
| 1–3 | 203 | 66 | 137 | 32.512 |
|
|
| ≥4 | 90 | 21 | 69 | 23.333 |
|
|
| TNM staging |
|
|
|
|
|
|
| I | 65 | 20 | 45 | 30.769 | 2.162 | 0.339 |
| II | 234 | 94 | 140 | 40.171 |
|
|
| III | 151 | 54 | 97 | 35.762 |
|
|
| Breast mass size,
cm |
|
|
|
|
|
|
| ≤2 | 107 | 53 | 54 | 49.533 | 10.520 | 0.005a |
| 2–5 | 274 | 90 | 184 | 32.847 |
|
|
| ≥5 | 69 | 21 | 48 | 30.435 |
|
|
| Menopause |
|
|
|
|
|
|
| No | 317 | 114 | 203 | 35.962 | 0.108 | 0.743 |
| Yes | 133 | 50 | 83 | 37.594 |
|
|
| c-erbB-2 |
|
|
|
|
|
|
|
Positive | 85 | 25 | 60 | 29.411 | 2.238 | 0.135 |
|
Negative | 365 | 139 | 226 | 38.082 |
|
|
| ER |
|
|
|
|
|
|
|
Positive | 167 | 44 | 123 | 26.347 | 11.688 |
<0.001a |
|
Negative | 283 | 120 | 163 | 42.403 |
|
|
| Ki-67,% |
|
|
|
|
|
|
|
≤14 | 41 | 20 | 21 | 48.780 | 2.964 | 0.085 |
|
>15 | 409 | 144 | 265 | 35.208 |
|
|
| Molecular
typing |
|
|
|
|
|
|
| Luminal
A | 62 | 22 | 40 | 35.484 | 17.466 |
<0.001a |
| Luminal
B | 249 | 84 | 165 | 33.735 |
|
|
|
HER-2-positive | 47 | 30 | 17 | 63.830 |
|
|
|
Triple-negative | 92 | 28 | 64 | 30.435 |
|
|
| Histological
grade |
|
|
|
|
|
|
| I | 90 | 51 | 39 | 56.667 | 22.770 |
<0.001a |
| II | 258 | 88 | 170 | 34.109 |
|
|
|
III | 102 | 25 | 77 | 24.510 |
|
|
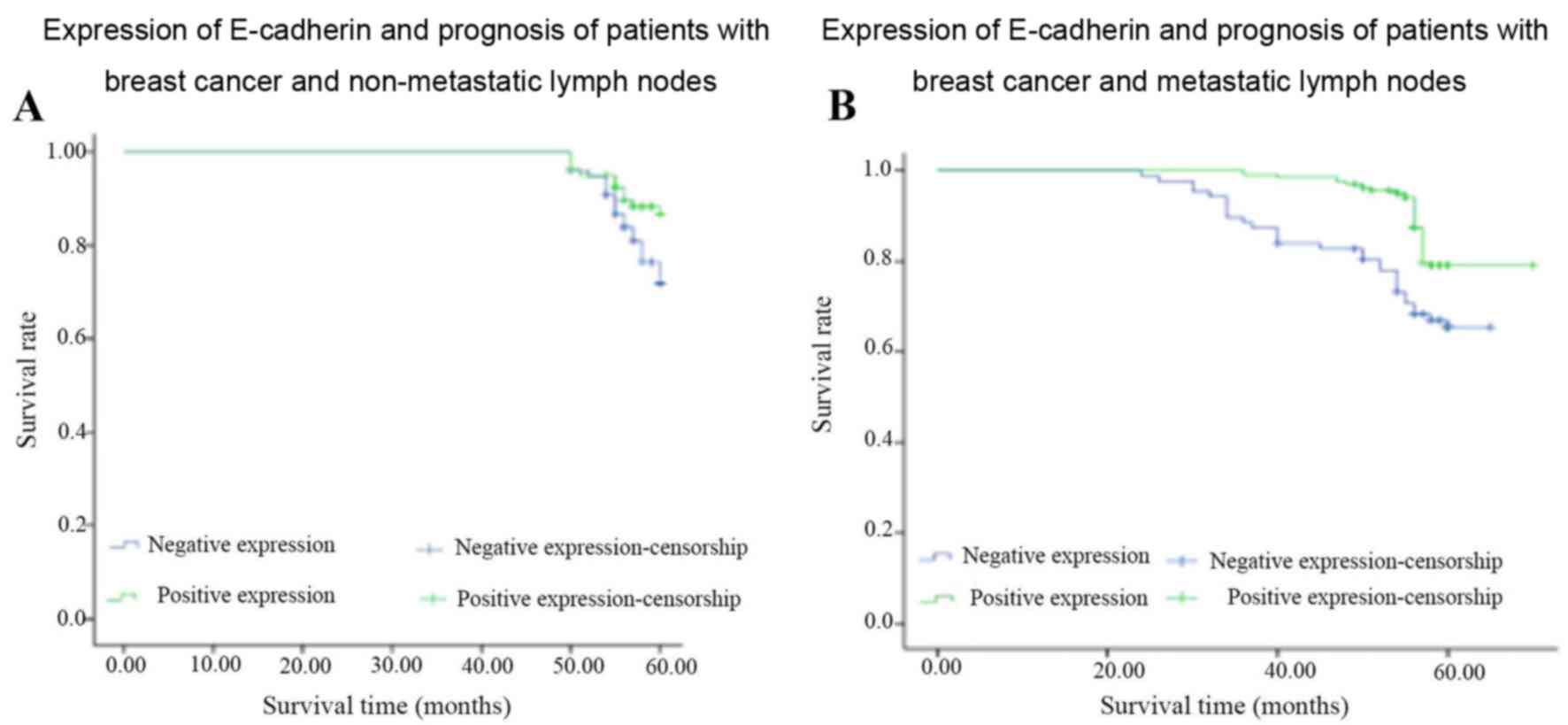
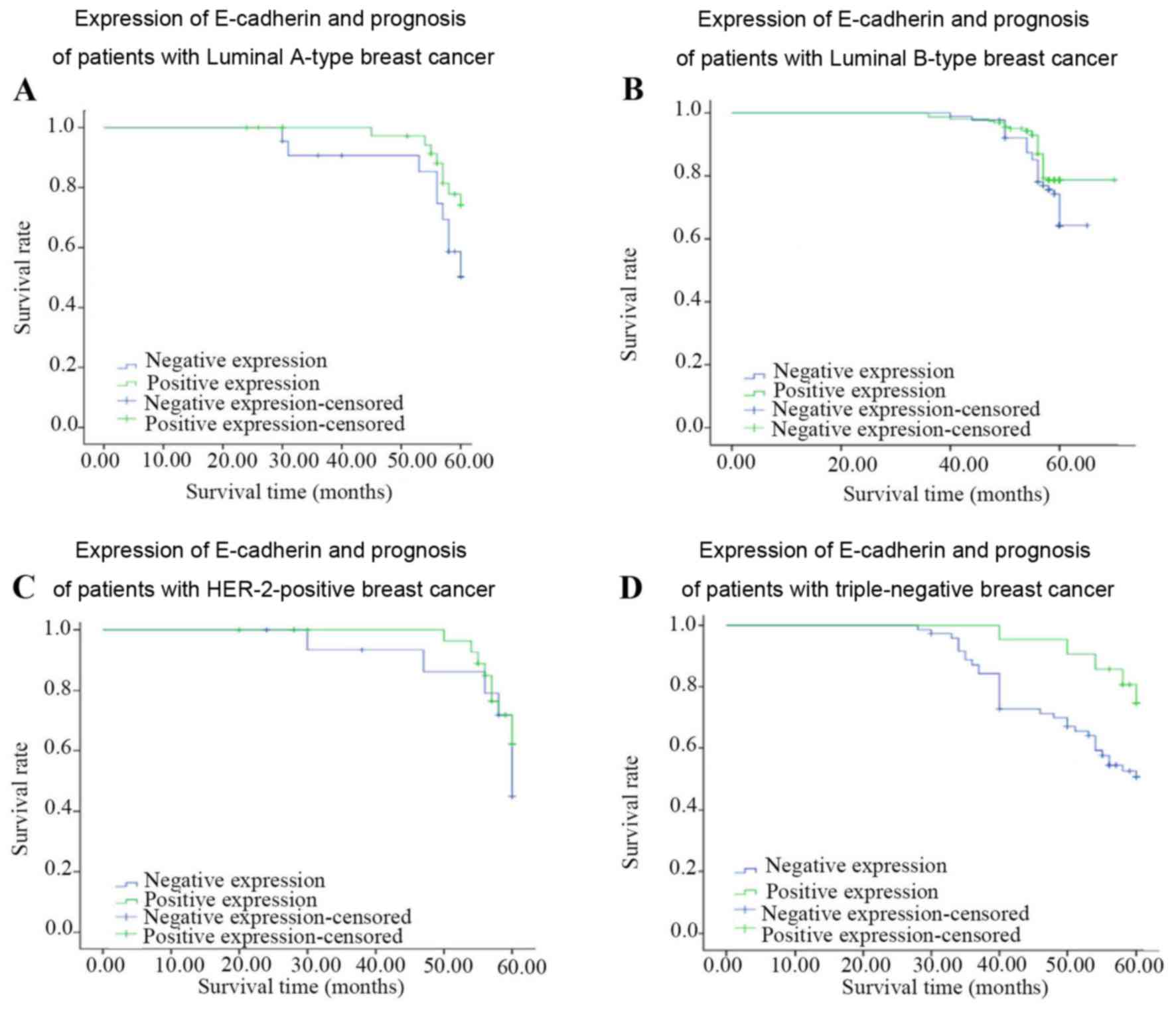
Expression of E-cadherin in breast
invasive ductal carcinoma and its association with the prognosis of
breast cancer
As shown in Tables
III and IV, and Figs. 3 and 4,
survival analysis identified that there were significant
differences in the expression of E-cadherin in the patients with
lymph node metastasis (χ2=9.546, P=0.002) and in
those with TNBC (χ2=4.48, P=0.03). The low expression of
E-cadherin inpatients with TNBC is associated with poorer
prognosis. There was no significant difference in the prognosis of
the untreated lymph node group, or the Luminal A, Luminal B or
human epidermal growth factor receptor 2 (HER-2)-positive
group.
| Table III.Expression of E-cadherin in lymph
node metastasis and non-metastasis of breast cancer was analyzed by
statistical analysis (Kaplan-Meier method). |
Table III.
Expression of E-cadherin in lymph
node metastasis and non-metastasis of breast cancer was analyzed by
statistical analysis (Kaplan-Meier method).
|
| Non-breast lymph
node metastasis group | Breast cancer lymph
node metastasis group |
|---|
|
|
|
|
|---|
| Test statistic | df | χ2 | P-value | df | χ2 | P-value |
|---|
| Log-rank
(Mantel-Cox) | 1 | 3.628 | 0.057 | 1 | 9.546 | 0.002a |
| Breslow
(generalized Wilcoxon) | 1 | 3.191 | 0.074 | 1 | 12.234 |
<0.001a |
| Tarone-Ware | 1 | 3.417 | 0.065 | 1 | 10.862 | 0.001a |
| Table IV.Expression of E-cadherin in different
molecular types of breast cancer: Survival analysis (Kaplan-Meier
method). |
Table IV.
Expression of E-cadherin in different
molecular types of breast cancer: Survival analysis (Kaplan-Meier
method).
|
|
| Luminal A | Luminal B | HER-2-positive |
Triple-negative |
|---|
|
|
|
|
|
|
|
|---|
| Test statistic | df | χ2 | P-value | χ2 | P-value | χ2 | P-value | χ2 | P-value |
|---|
| Log-rank
(Mantel-Cox) | 1 | 2.87 | 0.09 | 4.33 | 0.04 | 0.61 | 0.43 | 4.48 | 0.03a |
| Breslow
(generalized Wilcoxon) | 1 | 2.87 | 0.09 | 3.31 | 0.07 | 0.51 | 0.48 | 5.42 | 0.02a |
| Tarone-Ware | 1 | 2.87 | 0.09 | 3.75 | 0.05 | 0.51 | 0.46 | 5.03 | 0.02a |
Discussion
The incidence of breast cancer continues to grow,
and it is currently the most common form of malignant tumor among
Chinese women (3). Breast cancer
metastasis seriously affects the prognosis of patients and is the
leading cause of mortality (4). Of
those patients who receive an early diagnosis of breast cancer
subsequent to receiving adjuvant therapy, ~30% will eventually
develop recurrence or metastasis (5,6). Breast
cancer recurrence and metastasis are severe clinical problems.
Changes in cell adhesion are the main mechanism of
invasion and metastasis of a malignant tumor. Changes in adhesion
molecules may reduce the adhesion of tumor cells, contributing to
tumor infiltration and metastasis. Therefore, the decline of cell
adhesion is an important factor leading to tumor metastasis
(7).
E-cadherin is a type of cell adhesion glycoprotein;
it is not only a tumor cell invasion and metastasis inhibitor, but
it is also a normal cell growth inhibitor. Studies have found that
when epithelial-mesenchymal transition occurs in cancer cells,
E-cadherin expression decreases or shows a functional loss, thus
causing decreased cell adhesion, loss of polarity and infiltration
of the surrounding tissue growth, and it may be transferred to
bone, liver, lung and brain tissue (8). E-cadherin has become one of the research
hotspots among the cadherin family members. Studies have found that
E-cadherin is involved in the early occurrence, infiltration and
metastasis of different tumors (9–12). The
expression is of E-cadherin is closely associated with the invasion
and metastasis of a number of tumors and their clinical prognoses
(13–15).
The present study results suggested that low
expression or deletion of E-cadherin was positively associated with
lymph node metastasis. The negative expression rate was
significantly higher in breast cancer patients with local lymph
node metastasis than in patients without local lymph node
metastasis, and the differences were statistically significant.
Presumably, under normal circumstances, E-cadherin serves a role in
maintaining cell morphology within the body (16). The present findings further suggested
that E-cadherin was closely associated with the infiltration and
metastasis of breast ductal carcinoma and could be used as a marker
to predict the lymph node metastasis of invasive ductal carcinoma.
The study results suggested that E-cadherin expression was
associated with the prognosis of patients with breast cancer. The
5-year survival rate was higher in the E-cadherin-positive group
than that in the E-cadherin-negative group in lymph node metastatic
invasive ductal carcinoma, and the differences were statistically
significant (χ2=16.53, P<0.001). E-cadherin
expression was associated with the molecular typing of breast
cancer. E-cadherin exhibited low expression in breast cancer and
TNBC, which was closely associated with the invasion and metastasis
of TNBC. The expression of E-cadherin in HER-2-negative and
ER-positive samples was high, indicating that ER-positive
expression may be involved in the regulation of E-cadherin
expression.
Understanding these mechanisms and further
investigating the findings of this study will aid in confirming
these results and determining other associated important findings.
Further research is required to adequately understand the decrease
in cell adhesion.
Acknowledgements
Not applicable.
Funding
This study was supported by funds from the Xinjiang
Uygur Autonomous Region Natural Science Foundation (grant no.
2016D01C353).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XYW designed the experiment; LY, LPZ, BW and QZ
performed the experiments; XWW collected, analyzed and interpreted
data; LY drafted the manuscript and revised it critically for
important intellectual content, giving final approval of the
version to be published; HLW performed analysis and interpretation
of data, and modified the paper.
Ethics approval and consent to
participate
All subjects provided written informed consent. The
present study was approved by the Ethics Committee of the
Affiliated Tumor Hospital, Xinjiang Medical University (Urumqi,
China).
Consent for publication
All patients agreed to the publishing of the
data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cabioglu N: Staging of Breast Cancer.
Breast Disease. Springer International Publishing; Basel. p; pp.
13602016
|
|
2
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: Experience from a large study with
long-term follow-up. C. W. Elston & I. O. Ellis. Histopathology
1991; 19; 403–410. Histopathology. 41:403–410. 2002. View Article : Google Scholar
|
|
3
|
Miller KD, Siegel RL, Lin CC, Mariotto AB,
Kramer JL, Rowland JH, Stein KD, Alteri R and Jemal A: Cancer
treatment and survivorship statistics, 2016. CA Cancer J Clin.
66:271–289. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Milioli HH, Santos Sousa K, Kaviski R, Dos
Santos Oliveira NC, de Andrade Urban C, de Lima RS, Cavalli IJ and
de Souza Fonseca Ribeiro EM: Comparative proteomics of primary
breast carcinomas and lymph node mastases outlining markers of
tumor invasion. Cancer Genomics Proteomics. 12:89–101.
2015.PubMed/NCBI
|
|
6
|
Berman AT, Thukral AD, Hwang WT, Solin LJ
and Vapiwala N: Incidence and patterns of distant metastases for
patients with early-stage breast cancer after breast conservation
treatment. Clin Breast Cancer. 13:88–94. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li DM and Feng YM: Signaling mechanism of
cell adhesion molecules in breast cancer metastasis: Potential
therapeutic targets. Breast Cancer Res Treat. 128:7–21. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Paredes J, Figueiredo J, Albergaria A,
Oliveira P, Carvalho J, Ribeiro AS, Caldeira J, Costa AM,
Simões-Correia J, Oliveira MJ, et al: Epithelial E-and P-cadherins:
Role and clinical significance in cancer. Biochim Biophys Acta.
1826:297–311. 2012.PubMed/NCBI
|
|
9
|
Ye Y, Tian H, Lange AR, Yearsley K,
Robertson FM and Barsky SH: The genesis and unique properties of
the lymphovascular tumor embolus are because of calpain-regulated
proteolysis of E-cadherin. Oncogene. 32:1702–1713. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xue S and Chen YX: Progression on the
roles of E-cadherin in invasion and metastasis of gastric cancer.
Chin Clin Oncol. 6:555–558. 2015.(In Chinese).
|
|
11
|
Tian MY, Wang LH and Zhang X: Expressions
of E-cadherinand Vimentin in Lung Cancer Tissueand Their
Relationship to Epithelial-Mesenchymal Transition. Chin J Biol.
24:1068–1071. 2011.(In Chinese).
|
|
12
|
Wendt MK, Taylor MA, Schiemann BJ and
Schiemann WP: Down-regulation of epithelial cadherin is required to
initiate metastatic outgrowth of breastcancer. Mol Biol Cell.
22:2423–2435. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang YM, Wang YC, Wang RF, Wang LG and Tao
N: Expressions of MicroRNA-221 and E-cadherin in gastric cancer and
their relationship with clinical significance. Progress in Modern
Biomedicine. 31:6088–6091. 2017.(In Chinese).
|
|
14
|
Iseki Y, Shibutani M, Maeda K, Nagahara H,
Ikeya T and Hirakawa K: Significance of E-cadherin and CD44
expression in patients with unresectable metastatic colorectal
cancer. Oncol Lett. 14:1025–1034. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Spachmann PJ, Otto W, Vergho D, Kalogirou
C, Prohaska S, Weber F, Evert M, Burger M, Denzinger S, Kübler H
and Breyer J: High expression of E-cadherin and β-catenin is
associated with development of metastases and predicts worse
survival in renal cell carcinoma with invasion of the vena cava.
European Urology Supplements. 16:e28462017. View Article : Google Scholar
|
|
16
|
Humar B and Guilford P: Hereditary diffuse
gastric cancer: A manifestation of lost cell polarity. Cancer Sci.
100:1151–1157. 2009. View Article : Google Scholar : PubMed/NCBI
|